Sir,
Theories can be “macro” and attempt to explain a wide range of phenomena, or “micro” and aim to provide a mechanistic explanation for specific phenomena. A theoretical model is a “description or analogy used to help visualize something that cannot be directly observed” and is “specified in a form in which actual computations about outcomes can be made” (1). Whyte (1) argues that theory has a much larger role in rehabilitation science than simply “constraining choices in clinical trials”. He suggests that theories can serve as “general postulates”, anchored on limited empirical evidence with “implications far beyond those anchoring points”. He doubts it will be possible to develop a unifying theory of rehabilitation, since even within the field of theoretical physics it has not been possible to unify theories of gravity, acceleration and time with particle physics and electromagnetism.
The World Health Organization (WHO) International Classification of Functioning, Disability and Health (ICF) provides a framework for considering health, disability and function based on various domains within the components of body structure and function, impairment, activity, participation and environment (2). Functional problems can be specified in terms of activity limitations and participation restrictions. Environmental factors can be facilitators or barriers. Numeric qualifiers apply to the severity of a problem or degree to which an environmental factor is a facilitator or a barrier. Whyte suggests that the ICF is a taxonomic system of human function, and can be used to predict changes in one domain from changes in another and interactions between variables. However, he argues that there are unlikely to be quantitative, linear relationships between variables and that the theory does not predict how to make useful changes.
An ICF-based theoretical model for rehabilitation practice and research
Work has begun on an ICF-based theoretical model for rehabilitation practice and research (3). Reinhardt & Stucki (4) outline a visual theoretical model that can be applied “from basic to professional research”. This circular model has a central core of rehabilitation sciences, including physiotherapy, speech therapy, and rehabilitation medicine. This core is encircled by integrative rehabilitation sciences, surrounded by human functioning sciences. Each circle is transected by spokes pertaining to biomedical aspects, personal aspects and environmental aspects. Along these spokes there are scientific disciplines relevant to each of the 3 major components. To develop this further it would be interesting to assess whether the model can be used to make theoretically relevant predictions and be considered a general principle from which logical extensions can be made.
Further development of an ICF-based model of rehabilitation sciences
Theoretical physics models suggest that gravity can be accounted for by postulating that masses sink into the space-time continuum. An ICF-based model could be represented visually as a series of circles with varying distances below a baseline according to whether the issue was a mild, moderate, severe or complete problem to the individual or system being considered, via the use of the ICF concept of qualifiers. This would provide a dynamic framework, as the most significant issue would always be central to the model, whether the issue was to do with a body structure, function, activity, participation or environment. Issues of equal significance could coalesce, and be worked on together. Other, less significant issues would be represented peripherally. The model could be applied to individuals, rehabilitation teams, rehabilitation services, rehabilitation networks and research.
The model could be used for individuals to help prioritize the different aspects of the rehabilitation process. It could also be used to suggest the composition of a rehabilitation team for a given population sub-group with level of need defined in terms of impairment, activity, participation and environment. Figs 1 and 2 provide a suggested pictorial representation of this concept. The y axes provide a numeric value to the qualifiers applied to the different issues considered. The number “4” denotes a complete problem, facilitator or barrier. Zero indicates that the issue has no impact on the individual, team, service or network assessed while “1” indicates a mild issue, “2” a moderate issue, and “3” a severe or substantial issue.
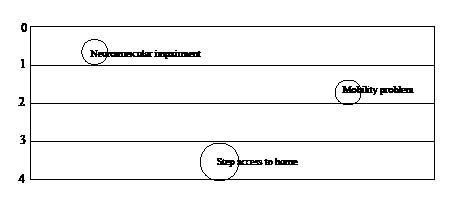
Fig. 1. An individual with a mild neuromusculoskeletal functional impairment, a moderate mobility problem, who is unable to return home from hospital because steps to the house are causing a barrier to access. The model illustrates that modification of the environment is the primary management strategy required for this individual.
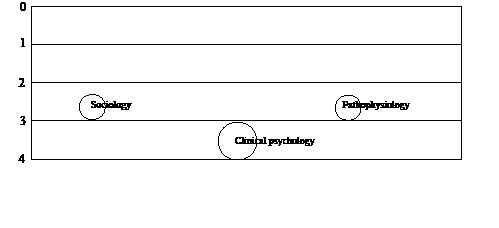
Fig. 2. For rehabilitation research pertaining to individuals with traumatic brain injury residing in the community, clinical psychology may be the key research area, with substantial inputs from sociology and pathophysiology.
A variety of scientific methods may be used within this model. Randomized controlled trials and single-case methodology studies are well-established methods of researching individuals and populations, where the effectiveness of treatments are investigated. Surveys, focus groups, qualitative analyses, field tests and retrospective collection of clinical indicators and outcome data may all be used to measure factors within the various ICF domains. However, each of these methods focuses on a limited range of domains and may specifically ignore the influence of external, environmental or personal factors, treating them as random error.
A description of the behaviour of a system using mathematics that may usefully be applied to an ICF-based model of rehabilitation is game theory. Game theory is a mathematical tool for analysing people and other factors interacting dynamically while making self-determined choices. It has been applied to areas relevant to rehabilitation, such as assignment of accommodation (5), medical staff placement schemes (6) and financing of public facilities (7).
Perach et al. (5) outline a model for assigning student accommodation according to student needs and disabilities. A similar model could be used to propose methods of allocating rehabilitation service users to different services and predicting the types of rehabilitation services that are likely to be required for given population subgroups. Unver (6) reviewed different models of allocating interns to jobs. This framework could be used in rehabilitation workforce planning and allocation of service users to appropriate facilities. Bogomolnaia et al. (7) propose models for determining the likely impact of different models of financing public facilities. These could be used to propose methods of siting and funding rehabilitation services. The ICF-based model of rehabilitation could be used as a source of appropriate variables for assessment and the concept of qualifiers could be used as a basis for the weighting of variables.
In conclusion, the ICF-based model of rehabilitation can therefore be considered a “macro” theory, explaining a wide range of phenomena, and a “micro” theory providing a mechanistic explanation of specific events, such as the multifactorial causes of disability. It can generate testable hypotheses, such as the optimal composition of the rehabilitation team for a given population sub-group. As a theoretical model it helps to visualize something that cannot be observed directly. It can be used to make theoretically relevant predictions, for example, that removing a barrier will have an expected influence on the dynamic relationship between activity, participation and environmental factors for an individual or population. With the use of a suitable mathematical tool, such as game theory, it can be put in a form in which computation about outcomes can be made. It can be considered as a starting point, originally anchored on theories pertaining to individuals, that has implications beyond those original anchoring points. It can be logically extended to apply to rehabilitation services, networks and research. It has the potential to provide a theory of how change is achieved in rehabilitation and can make specific predictions that can be empirically validated or refuted.
References
Submitted July 18, 2010; accepted September 20, 2010
Susan Graham, BM, PhD, FAFRM (RACP)1 and
Ian Cameron, MBBS, PhD, FAFRM (RACP)2
From the 1School of Medicine, University of Queensland, Brisbane and 2School of Medicine, University of Sydney, Sydney, Australia. E-mail: susan-graham@ausdoctors.net

