Vitor Oliveira Carvalho, PT, PhD1, Rachel Garrod, PT, PhD2, Edimar Alcides Bocchi, MD, PhD1, Fabio Pitta3 and Guilherme Veiga Guimaraes, PhD1
From the 1Laboratório de Insuficiência Cardíaca e Transplante do Instituto do Coração do Hospital das Clínicas da Faculdade de Medicina da USP (InCor HC-FMUSP), São Paulo, Brazil, 2Kings College Hospital, Denmark Hill, London, UK and 3Departamento de Fisioterapia, Universidade Estadual de Londrina, Brazil
BACKGROUND: The Minnesota Living with Heart Failure Questionnaire (MLHFQ) is a well-validated, commonly-used tool to assess quality of life in patients with heart failure. However, it lacks specific information concerning breathlessness during daily activities.
OBJECTIVE: To determine the validity of the London Chest Activity of Daily Living (LCADL) scale for use in patients with heart failure.
METHODS: Forty-seven patients with heart failure (57% males, mean age 50 years (standard deviation 9), mean left ventricle ejection fraction 29% (SD 6), New York Heart Association (NYHA) functional class I–III) were included. All subjects first performed a cardiopulmonary exercise test and then responded to the LCADL and the MLHFQ, with guidance from the same investigator. The re-test for the LCADL was applied one week later.
RESULTS: LCADL was correlated with MLHFQ (r = 0.88; p < 0.0001). LCADL and MLHFQ were also correlated with exercise capacity (r = –0.75 and r = –0.73, respectively; both p < 0.0001). The LCADL was shown to be reproducible (ri = 0.98). There was a significant difference (p < 0.05) in the LCADL scores between NYHA functional classes I and II, as well as classes I and III, but not between classes II and III.
CONCLUSION: The LCADL was shown to be a valid measurement of dyspnoea during daily activities in patients with heart failure. This scale could be an additional useful tool for the assessment of patients’ dyspnoea during activities of daily living.
Key words: exercise; heart failure; activities of daily living; quality of life.
J Rehabil Med 2010; 42: 715–718
Correspondence address: Vitor Oliveira Carvalho, Av. Dr. Enéas de Carvalho Aguiar, 44, Laboratório de Insuficiência Cardíaca, Bloco 1, 10 Andar, InCor, São Paulo, Brazil. E-mail: vitor.carvalho@usp.br
Submitted October 22, 2009; accepted April 27, 2010
BACKGROUND
Heart failure can be considered the last stage of heart disease and is a significant cause of mortality and morbidity worldwide (1–3). It is characterized by persistent activation of the circadian neurohormonal system (4–6), endothelial dysfunction (7), exercise intolerance (8–12), high mortality (13), and an impaired quality of life (14). Patients experience cardiopulmonary and musculoskeletal limitations that greatly reduce their ability to exercise and impair their quality of life (15). In patients with heart failure there is a strong relationship between quality of life, exercise capacity and morbidity/mortality (13, 14). These three are the main end-points of any heart failure treatment. For this reason, it is important that the impact of heart failure on an individual’s quality of life and activities of daily living (ADL) can be fully quantified.
The most commonly used tool to assess quality of life in patients with heart failure is the Minnesota Living with Heart Failure Questionnaire (MLHFQ); however, this tool provides limited information concerning the patient’s functional status, i.e. the patient’s performance during ADL. The London Chest Activity of Daily Living scale (LCADL) is a tool that was initially validated to measure breathlessness during daily activities in patients with severe chronic obstructive pulmonary disease (COPD) (16–18). However, since breathlessness during ADL is also a feature of heart failure, the LCADL could feasibly be applied in this population in order to provide important information concerning breathlessness and functional activity. The evaluation of these outcomes may enable the development of further intervention strategies to address breathlessness during ADL in this rather disabled population.
The aim of this study was to determine the validity and reproducibility of the LCADL in patients with heart failure, as well as to investigate the ability of the instrument to discriminate between patients with different functional impairments as determined using New York Heart Association (NYHA) functional class.
METHODS
Study population
Forty-seven patients with heart failure (57% males), mean age 50 years (standard deviation (SD) 9), and left ventricular ejection fraction 29% (SD 6) (by echocardiography) were recruited from a tertiary cardiology hospital during the period October 2007 to June 2008. All patients had been in a stable clinical condition for 3 months with no change in medication during this period. Patients with non-cardiovascular functional limitations, such as osteoarthritis, stroke and COPD, were excluded from the study. The study was approved by the institution’s ethics committee, and all patients provided informed consent before participation. Baseline characteristics are shown in Table I.
| Table I. Group characterization of patients with heart failure |
| Characteristics | |
| Sex, % | |
| Male | 57 |
| Female | 43 |
| Aetiology, % | |
| Ischaemic | 40 |
| Non-ischaemic | 60 |
| NYHA functional class, % | |
| I | 32 |
| II | 34 |
| III | 34 |
| Left ventricle ejection fraction, %, mean | 29 (6) |
| Peak VO2, mlO2/kg/min, mean (SD) | 18.1 (5.5) |
| Time of CPX, min, mean (SD) | 11.3 (4.1) |
| MLHFQ, mean (SD) | |
| Total score | 50.2 (25.4) |
| Physical score | 20.6 (11.4) |
| LCADL, mean (SD) | |
| Total score | 35.9 (21.9) |
| Physical score | 7.3 (3.0) |
| Domestic score | 15.7 (9.7) |
| Personal score | 8.0 (6.2) |
| Leisure score | 5.2 (4.4) |
| Current medications; %, mg/day, mean (SD) | |
| Diuretics | |
| Furosemide | 60%, 44 (16) |
| Hydrochlorothiazide | 44%, 35 (13) |
| Angiotensin converting enzyme inhibitors | |
| Enalapril | 61%, 32 (11) |
| Captopril | 22%, 41 (25) |
| Angiotensin II AT1 receptor antagonists (losartan) | 17%, 75 (27) |
| ß-adrenergic receptor blocker (carvedilol) | 100%, 57 (36) |
| Spironolactone | 30%, 25 (0) |
| Digoxin | 45%, 0.25 (0) |
| Isosorbide 5-mononitrate | 24%, 51 (32) |
| NYHA: York Heart Association; VO2: oxygen consumption; CPX: cardiopulmonary exercise test; MLHFQ: Minnesota Living with Heart Failure Questionnaire; LCADL: London Chest Activity of Daily Living scale; SD: standard deviation. |
Study design
This was a cross-sectional design to evaluate the use of LCADL in patients with heart failure. Firstly, all subjects performed a cardiopulmonary exercise test to determine their exercise capacity objectively. Patients then responded to the LCADL and the MLHFQ, supervised by the same investigator. The LCADL was reapplied via a telephone call after one week to evaluate the scale’s reproducibility. An analysis of the LCADL, stratified by the patients’ functional limitation according to the NYHA classification (19), was performed, as well as for the MLHFQ.
Cardiopulmonary exercise test
All subjects underwent the cardiopulmonary exercise test on a programmable treadmill (Series 2000, Marquette Electronics, Milwaukee, WI, USA) in a temperature-controlled room (21–23ºC) between 10:00 h and 15:00 h with a standard 12-lead continuous electrocardiogram monitor (Max 1, Marquette Electronics). Blood pressure monitoring was performed by the auscultation method. Minute ventilation, oxygen uptake, carbon dioxide output and other cardiopulmonary variables were acquired breath-by-breath by a computerized system (Vmax 229 model, SensorMedics, Yorba Linda, CA, USA). Peak effort (peak oxygen consumption) and peak heart rate were the mean values of the final 30 s of effort before exhaustion. The respiratory exchange ratios were recorded as the averaged samples obtained during each stage of the protocol used (modified Naughton protocol). A satisfactory cardiopulmonary exercise test was characterized by a peak of respiratory exchange ratio > 1.05 and symptoms of maximum effort.
London Chest Activity of Daily Living scale
This 15-item questionnaire was designed to measure dyspnoea during routine daily activities in patients with COPD. It is divided in 4 domains: self-care (4 items), domestic (6 items) physical activity (2 items) and leisure (3 items). The patient reports on the perception of dyspnoea during the past few days for these 15 items. For each activity the patient reports a score between 0 and 5 (0 = I wouldn’t do it anyway, 1–4 are varying degrees of breathlessness and 5 indicates a need for someone else to carry out the activity) (16).
Minnesota Living with Heart Failure Questionnaire
This 21-item questionnaire was designed to measure daily limitations in patients with heart failure. It is divided into two domains: emotional and physical. The patient must consider the last month and report how their heart failure interferes in these 21 items, choosing a score between 0 (no limitation) and 5 (maximal limitation) for each activity, as described previously (14).
Statistical analysis
Data were analysed using the Statistical Package for Social Sciences for Windows, 11.5 (SPSS Inc., Chicago, IL, USA). Relationships between ordinal data (questionnaires) were studied by the Spearman’s correlation coefficient. To compare the LCADL between the NYHA Functional Class I, II and III we used analysis of variance (ANOVA) with a post-hoc Bonferroni test. Intraclass correlation coefficients (ri) with 95% confidence interval (95% CI) and Cronbach’s alpha were calculated in order to test the agreement between the test and re-test. Bland-Altman plots with 95% limits of agreements were also derived. Statistical significance was set at p < 0.05.
RESULTS
All patients with heart failure were limited functionally, as expressed by a mean peak VO2 of 18.1 (SD 5.5) mlO2/kg/min and a mean score of MLHFQ 50.2 (SD 25.4) (Table I). The MLHFQ was highly correlated with LCADL. MLHFQ and LCADL were also highly correlated with exercise capacity variables (Table II).
| Table II. Correlation between studied variables |
| Exercise | MLHFQ | r | p | Exercise | LCADL | r | p | MLHFQ | LCADL | r | p |
| Peak VO2 | Total Physical | –0.73 –0.76 | < 0.0001 < 0.0001 | Peak VO2 | Total | –0.75 | < 0.0001 | Total | Total | 0.88 | < 0.0001 |
| Self-care | –0.72 | < 0.0001 | Self-care | 0.81 | < 0.0001 |
| Domestic | –0.76 | < 0.0001 | Domestic | 0.86 | < 0.0001 |
| Physical | –0.73 | < 0.0001 | Physical | 0.88 | < 0.0001 |
| Leisure | –0.72 | < 0.0001 | Leisure | 0.81 | < 0.0001 |
| Time of CPX | Total Physical | –0.68 –0.70 | < 0.0001 < 0.0001 | Time of CPX | Total | –0.71 | < 0.0001 | Physical | Total | 0.82 | < 0.0001 |
| Self-care | –0.67 | < 0.0001 | Self-care | 0.83 | < 0.0001 |
| Domestic | –0.72 | < 0.0001 | Domestic | 0.87 | < 0.0001 |
| Physical | –0.67 | < 0.0001 | Physical | 0.90 | < 0.0001 |
| Leisure | –0.66 | < 0.0001 | Leisure | 0.76 | < 0.0001 |
| VO2: oxygen consumption; CPX: cardiopulmonary exercise test; MLHFQ: Minnesota Living with Heart Failure Questionnaire; LCADL: London Chest Activity of Daily Living scale. |
Table III shows a statistically significant difference in the LCADL scores between NYHA functional classes I and II, as well as classes I and III, but not between classes II and III. Despite this, LCADL total score (r = 0.68), and sub-scores self-care (r = 0.65), domestic (r = 0.69), physical (r = 0.67) and leisure (r = 0.60) correlated with NYHA functional class (p < 0.0001 for all).
| Table III. Stratified data according to the NYHA functional class |
| NYHA | MLHFQ total Mean (SD) | MLHFQ physical Mean (SD) | LCADL total Mean (SD) | LCADL physical Mean (SD) | LCADL domestic Mean (SD) | LCADL leisure Mean (SD) | LCADL self-care Mean (SD) |
| I II III | 22 (21)*,** | 8 (8)*,** | 12 (14)*,** | 3 (2)*,** | 5 (7)*,** | 1 (3)*,** | 2 (3)*,** |
| 62 (15) | 25 (5) | 43 (14) | 9 (1) | 19 (6) | 6 (4) | 10 (5) |
| 64 (13) | 28 (8) | 51 (13) | 9 (1) | 22 (6) | 8 (3) | 12 (5) |
| *p < 0.05 between NYHA I and II, **p < 0.05 between NYHA I and III. NYHA: York Heart Association; MLHFQ: Minnesota Living with Heart Failure Questionnaire; LCADL: London Chest Activity of Daily Living scale; SD: standard deviation. |
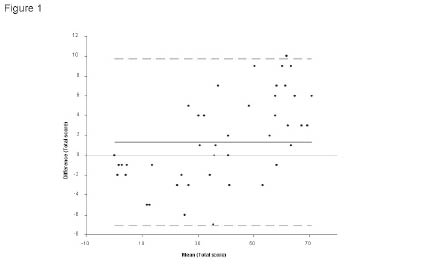
The LCADL was strongly reproducible in all domains. Total score showed a Cronbach’s alpha of 0.99, ri of 0.98 (95% CI 0.92–0.97); self-care domain showed a Cronbach’s alpha of 0.97, ri of 0.95 (95% CI 0.92–0.97); domestic domain showed a Cronbach’s alpha of 0.99, ri of 0.97 (95% CI 0.95–0.98); physical domain showed a Cronbach’s alpha of 0.96, ri of 0.91 (95% CI 0.85–0.95); and leisure domain showed a Cronbach’s alpha of 0.98, ri of 0.96 (95% CI 0.93–0.97) (Fig. 1).
Fig. 1. Bland-Altman plot for LCADL test and re-test. The continuous line is the mean and the dotted line the 95% of the confindence limit agreement.
DISCUSSION
The main finding of this study was the validity of the LCADL as a useful tool in the assessment of dyspnoea during ADL in patients with heart failure. The LCADL was reproducible and was shown to be able to stratify the patients’ functional limitation according to the NYHA classification.
The evaluation of the quality of life of patients with heart failure is an important factor in prognostic stratification and intervention strategies (13). However, there is a lack of information regarding breathlessness during ADL assessed the MLHFQ. We therefore proposed that the LCADL might address this deficiency in the MLHFQ.
In our study, patients had no difficulties in completing the LCADL. Some factors may have influenced this: the score of each question ranging between 0 and 5, used by both MLHFQ and LCADL, and the fact that the activities included in the LCADL are familiar and represent frequent complaints by patients with heart failure. The LCADL was correlated well with the MLHFQ, especially for the physical domain. These results are not surprising, since heart failure and COPD are chronic disturbances that cause breathless and show a number of previously identified common features (20).
The LCADL represented the functional status of patients with heart failure, as noted by strong correlations with exercise capacity variables, MLHFQ and NYHA classification. These data suggest that the LCADL scores are a good reflection of the patient’s functional limitation caused by dyspnoea, which is a complex outcome influenced by a diversity of other interconnected outcomes.
The impairment of ADL in patients with heart failure is classically assessed using the 6-min walk test, since the distance covered on the test is considered to be a good marker of functional capacity to perform daily activities (9, 21). However, due to a lack of sufficiently sensitive measures of ADL in heart failure, ours is the first study adequately to describe breathlessness during daily activities in this population.
The NYHA functional class is the most commonly used method to stratify patients with heart failure based on breathlessness and functional limitations during daily activities. However, the NYHA functional classification was not designed specifically to consider ADL. In our study, LCADL scores were able to stratify the patients according to the NYHA functional class, in the case of classes I–II and I–III. Differentiation between NYHA functional class II and III was not possible by LCALD in the present study. We speculate that subjective variations in the classification of more severely limited patients into class II or III, which routinely occur during daily clinical practice, could have influenced this result. Despite this, the LCADL was well-correlated to the NYHA functional class, which corroborates its usefulness in this population.
The use of the LCADL could contribute more specifically to clinical studies to assess the impact of an intervention (physical or pharmacological) on ADL of patients with heart failure. Moreover, the identification of the major limitations in ADL, could lead to more specific interventions in the rehabilitation process.
Study limitations
This study is limited by the small sample size, the fact that it is a single-centre study, and the need for studies of the responsiveness, interpretability and prognostic significance of the LCADL.
Conclusion
In conclusion, the LCADL was shown to be a valid and reproducible measure of dyspnoea during ADL in patients with heart failure. This scale could be an additional important tool for the assessment of patients’ dyspnoea sensation during ADL and to discriminate/categorize patients with different functional impairments. We propose the use of the MLHFQ followed by the LCADL in order to obtain a better evaluation of patients with heart failure, and not the substitution of the MLHFQ by the LCADL.
Acknowledgements
This study was partially supported by “Coordenação de Aperfeiçoamento de Pessoal de Nível Superior” (CNPq/Brazil).
References