Hartwig Woldag, MD, Katharina Stupka and Horst Hummelsheim, MD
From the Neurologisches Rehabilitationszentrum Leipzig, University of Leipzig, Germany
Hartwig Woldag, MD, Katharina Stupka and Horst Hummelsheim, MD
From the Neurologisches Rehabilitationszentrum Leipzig, University of Leipzig, Germany
OBJECTIVE: Repetitive training of simple upper limb movements is effective in stroke rehabilitation. For the repetitive training of complex movements, however, results are inconsistent. The aim of this study was to determine whether repetitive training of complex upper limb movements, focussing on strength and velocity as shaping elements, is effective in stroke rehabilitation.
DESIGN: Longitudinal study, A–B–A design.
Patients: Fifteen first-ever stroke patients.
METHODS: Phases (A): “house-typical” therapy and repetitive training of: (i) grasping and transport movements; and (ii) sawing movements of the affected arm with shaping elements and focussing on velocity over 10 min each, twice daily, 5 days per week. Phase B: “house-typical” occupational and physiotherapy. Each phase lasted 3 weeks.
RESULTS: Patients experienced continuous functional improvement. Voluntary forces improved significantly during the first training phase. Sawing movement improved significantly only during phases A. The grasping and transport movement improved considerably during phase A with a trend of further improvement during the other phases. The transported weight clearly increases only during phases A.
CONCLUSION: Repetitive training of complex movements results in motor improvement in stroke patients without relevant transfer to functional improvement if strength and velocity are to be enhanced as shaping elements.
Key words: repetitive training; stroke; arm; rehabilitation.
J Rehabil Med 2010; 42: 582–587
Correspondence address: Hartwig Woldag, Neurologisches Rehabilitationszentrum Leipzig, University of Leipzig, Muldentalweg 1, DE-04828 Bennewitz bei Leipzig, Germany. E-mail: woldag@sachsenklinik.de
Submitted August 23, 2009; accepted February 8, 2010
INTRODUCTION
Impairment of arm and hand function in patients after stroke contributes considerably to disability and dependency on caregivers. Based on the knowledge of long-term potentiation after tetanic stimulation of corticocortical neurones as a fundamental neural basis of motor learning (1, 2) the repetitive training of stereotyped simple hand and finger movements has been introduced, which has proved effective in improving the function of the centrally paretic upper limb (3). Since more and more physiotherapeutic concepts focus on motor training in a real-world environment (4, 5) and most everyday arm and hand movements are complex, the question arises as to whether a repetitive training of complex movements of hand and arm is beneficial for functional recovery after stroke. We therefore conducted a study using the multiple-baseline-across-individuals design. A house-specific physiotherapy was given during baseline, followed by repetitive training of 2 different complex movements (grasping and transport movement, sawing movement of the arm in the sagittal plane) during the training phase (6). In fact, this study failed to show any advantage of repetitive training of complex movements compared with house-specific therapy. Patients recovered significantly, but continuously, over the entire study time. Two major reasons for this negative result were discussed: (i) the training programme did not include shaping elements; and (ii) patients were instructed to perform the movements as precisely, but not as rapidly, as possible. Shaping is an operant conditioning method of learning in which a desired motor or behavioural objective is approached in small steps of increasing difficulty or increasing demand. A second constitutional element of shaping is the immediate feedback on task performance and positive reinforcement of improvements. Shaping is an essential element of constraint-induced movement therapy (CIMT), an efficacious therapeutic approach with a very high degree of evidence (7–10). Precise reaching movements require well-coordinated and timed movements of body parts (hand, arm, shoulder). However, studies on reaching and grasping in stroke patients have consistently shown that reaching movements are slower, less accurate and not as well coordinated as in healthy controls (11– 13). Precision of reaching movement seems to be a parameter that should be addressed in the late rehabilitation process. Parameters that should be integrated earlier in shaping procedures in stroke patients are movement velocity and strength (14–16).
We hypothesized that focussing on movement velocity and strength and the use of shaping strategies are crucial elements for an efficient repetitive training of complex movements of upper limb. Based on these hypotheses a new study was conducted using the same complex movements and assessments, but this time focussing on movement velocity and shaping elements during the training.
METHODS
Subjects
Inclusion criteria was a first-ever stroke (cerebral, subcortical lesions) confirmed by computed tomography (CT) or magnetic resonance imaging (MRI), resulting in a mild to moderate paresis of the upper limb (3–4 according to Medical Research Council). Exclusion criteria were: patients presenting with major sensory deficits (pallaesthesia ≤ 3 on the C64 tuning fork, anaesthesia in clinical testing), complete paralysis of the hand, upper limb contractures (unrestricted in passive range of motion), additional lesions of cerebellum or peripheral nervous system, aphasia leading to severe deficits in the understanding of instructions, neglect phenomena (patients must be able to shift their attention to the paretic arm) or other serious neuropsychological deficits (particularly severe cognitive, attention or executive deficits).
Twenty-five patients from our rehabilitation centre were screened as eligible and enrolled in the study. Ten patients finished the study pre-term (for reasons see Results). Data for the remaining 15 patients are summarized in Table I.
The study protocol was approved by the local ethics committee, and all patients gave their written informed consent.
Experimental protocol
The studies of repetitive simple (3) and complex movement trainings (6) followed a multiple-baseline-across-individuals design. This design has the advantage that each patient serves as his or her own control. Nevertheless, considering some design weaknesses, we decided to use a classical A1–B–A2 design for this study, with A as training phase. This design has the advantage that, in case of a significant training effect, the difference from standard therapy will be shown twice, independent of time. During all phases, lasting 3 weeks each, every patient received house-specific physiotherapy and occupational therapy. House-specific physiotherapy consisted of functional voluntary performances to enhance strength, active and passive range of motion and motor skills of both upper and lower limbs. Occupational therapy involved in particular the activities of daily living (ADL) (putting on clothes, washing, preparing meals) and fine motor activities of the hand. Both the occupational therapy and the physiotherapy were administered for 45–60 min per day as individual and group therapy 6 days a week. During the training phases (A1 and A2) patients additionally had to perform 2 different complex movements with the affected arm 10 min each, twice daily, for 5 days a week. We regarded movements as complex if they required a coordinated activation of at least 2 adjacent joints. The first task consisted of reach, grasp and transport movements. Patients had to reach and grasp a mug (diameter 7 cm, distance 40 cm), lift and move it from 1 point to another point following a given direction in the patient’s frontal plane and put it down at that point. Between the transport movements the hand rested at a third point on the table near the patient’s body. The 3 points formed an equilateral triangle with a side length of 40 cm with one corner directed to the patient. In this way the direction of reach and transport movements alternated between towards the affected and towards the unaffected side. The second task was a sawing movement of the arm in a sagittal plane with the same mug. So far, the training was identical to our previous study (6). The main difference was that we now introduced shaping elements by increasingly filling the mug with weights depending on the patients’ functional improvement. Before starting the training the number of movement repetitions (grasping and transport movement and sawing movement, respectively) performed during 1 min was counted. The mug was filled with an additional 100 g if the patient performed one repetition more than during the previous training. Within one training session the weight was kept constant. Additionally, we asked the patients to move the mug as fast as possible. Precision of movements was not a focus of the training. After each movement session we gave a feedback about the performance as terminal knowledge of results of movement time, number of repetitions and transported weight. Every improvement was positively reinforced.
Assessments
The Rivermead Motor Assessment, arm section (17, 18) was used to evaluate the functional motor capacity of the upper limb. This is a validated test providing a strong correlation between increasing score and functional relevance. Assessments were carried out by trained and experienced occupational therapists and physiotherapists. Measurements and assessments were performed by therapists who were not involved in the training of the same patient.
Grip strength
Grip strength was measured using a digital pinch/grip analyser (Digital Multi-Myometer, MIE medical research Ltd, Leeds, UK), which consisted of 2 bars mounted parallel to each other in the shape of a tuning fork. The distance between the bars was adjusted according to the size of the patients’ paretic hand and their ability to squeeze the bars with that hand. The position of the hand and the distance between the bars were kept constant for each patient throughout the entire measurement series. Patients were asked to squeeze the bars as rapidly and strongly as possible. Ten contractions were recorded with a resting time of 10 s after each contraction to prevent fatigue. The force signals were stored on the laboratory computer for offline analysis. Mean values were used for further analysis.
Rapid isotonic hand extension
For analysis of rapid isotonic hand extensions a piezoelectric accelerometer (Type 8303A10, Kistler Instrument Corp., Winterthur, Switzerland) was taped 3 cm distal to the styloid process of the ulna on the dorsal surface of the paretic hand. Patients were instructed to perform an isotonic extension at the wrist as fast as possible. Ten contractions were recorded and analysed using a commercial data acquisition system (MP100 Workstation, Biopac Systems, Inc., Santa Barbara, Canada). Mean values were used for further analysis.
Movement analysis
The complex movements described above were recorded using a 3-dimensional ultrasonic motion analysing system (CMS 70 by Zebris®, Isny, Germany). This device continuously calculates the 3-dimensional spatial positions of small ultrasound emitting markers attached via flexible cables to moving body parts (sampling frequency 66 Hz). Three markers were positioned on the arm: marker 1 on the radial side of the wrist over the styloid process, marker 2 on the elbow, and marker 3 on the shoulder. All markers had to be in visual contact with the panel containing 3 receiving microphones positioned on the patient’s paretic side and inclined downwards at an angle of 45°. The panel stood on the paretic side of the patient in an upright position. At least 20 repetitions of each movement were recorded in one measurement session.
Data acquisition was done using the “Win Data” software version 2.11 (Zebris®, Isny, Germany) and data analysis using “3DA” version 1.3 (MedCom, Munich, Germany). The reliability and validity of this measurement system was tested with a test-retest correlation of r = 0.89 and an intraclass correlation (ICC) of between 0.77 and 0.96 (19–21).
The weight of the mug was increased only during the training sessions, while the 3-dimensional movement analysis was always performed with an empty mug.
All measurements were taken once prior to starting and at the end of the study and once a week during all phases of the study.
Statistical analysis
The data were tested for normal distribution by the Kolmogorov-Smirnov test. Since not all parameters were normally distributed non-parametric tests were used for further analysis. To test for changes in outcome parameters the Friedmann test was used as a global test. To detect the effects of the different phases, the data for the 1st (prior study start), 4th (end of phase A1), 7th (end of phase B) and 10th (end of phase A2) measure points were compared using the paired Wilcoxon test, with p < 0.05, considering Bonferroni correction. Since we knew the direction of changes from former studies, we performed the tests as 1-tailed tests.
RESULTS
Subjects
The data for 15 patients could be analysed (Table I). Reasons for pre-term study termination of 10 patients were:
• termination of the in-patient rehabilitation for personal reasons: 4 patients;
• increasing pain and stiffness in elbow and fingers: 3 patients;
• deterioration due to concomitant illness: 1 patient;
• protocol violation: 1 patient;
• data loss: 1 patient.
Two of the 3 patients who had increasing pain and stiffness terminated the study during the first training week (A1) and the third patient during phase B. The increase in pain and stiffness may be caused by the intensive training and should be carefully monitored during practice.
Rivermead Motor Assessment
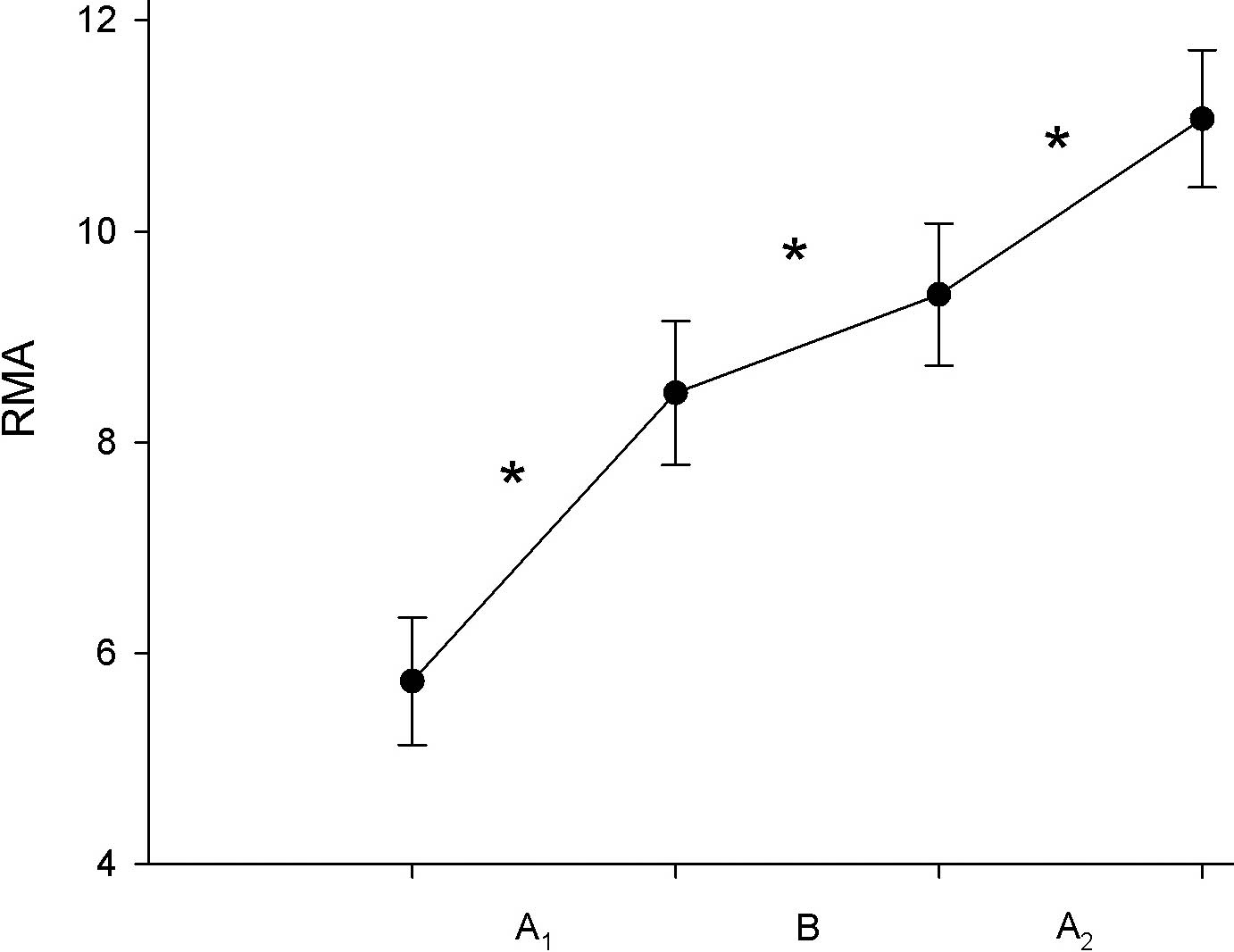
The Friedmann test showed a highly statistically significant global increase for the arm section of the Rivermead Motor Assessment (RMA) (p < 0.0001). Further analysis by the paired Wilcoxon test showed a significant increase during phase A1 (p = 0.001, Z = –2.814), phase B (p = 0.004, Z = –2.588) and phase A2 (p = 0.008, Z = –2.371). Thus, the functional capacity of the impaired upper limb improved throughout the study without a detectable additional effect of the repetitive training of complex movements during phases A1 and A2 (Fig. 1).
Fig. 1. Mean (± SEM) of the Rivermead Motor Assessment, arm section. A1, A2: training phase; B: house-specific therapy. Asterisks indicate significant improvements. SEM: standard error of the mean.
Isometric grip strength and rapid isotonic hand extension
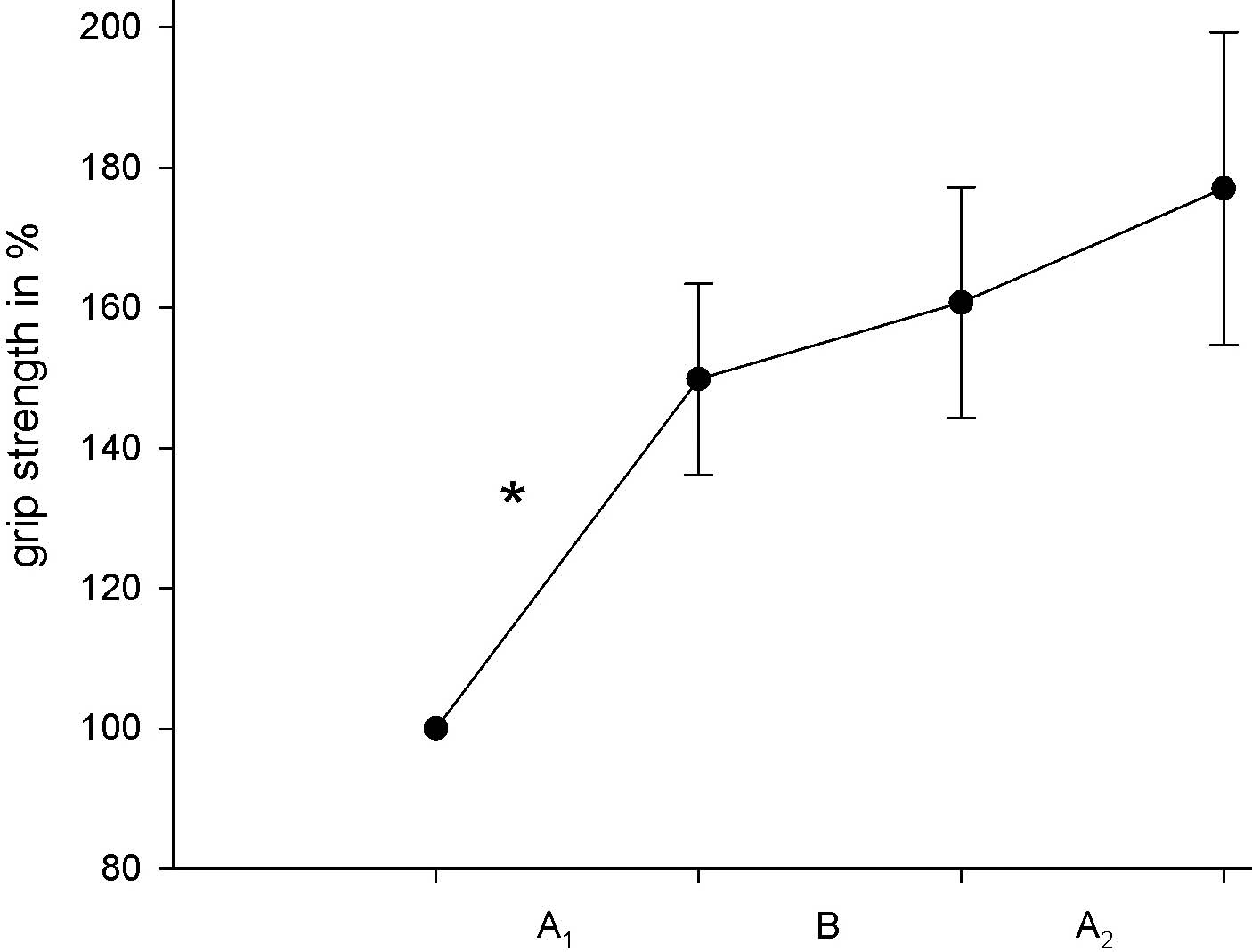
The data of both parameters showed an improvement in all 3 phases and we found a statistical significant global increase for isometric grip strength (Friedmann test, p < 0.0001) and acceleration of rapid isotonic hand extension (Friedmann test, p = 0.001). The paired Wilcoxon test revealed a significant increase (grip strength: p < 0.0001, Z = –3.237, isotonic hand extension: p = 0.001, Z = –2.840) only for phase A1. During phases B and A2 a trend of further improvement in both parameters was seen that did not reach statistical significance (Table II and Fig. 2).
Fig. 2. Mean (± SEM) of the grip strength expressed relative to the initial value. A1, A2: training phase; B: house-specific therapy. Asterisks indicate significant improvements. SEM: standard error of the mean.
Movement analysis
Both complex movements showed a qualitative improvement during the study. The movements became smoother and the variability of the trajectories declined (Fig. 3).
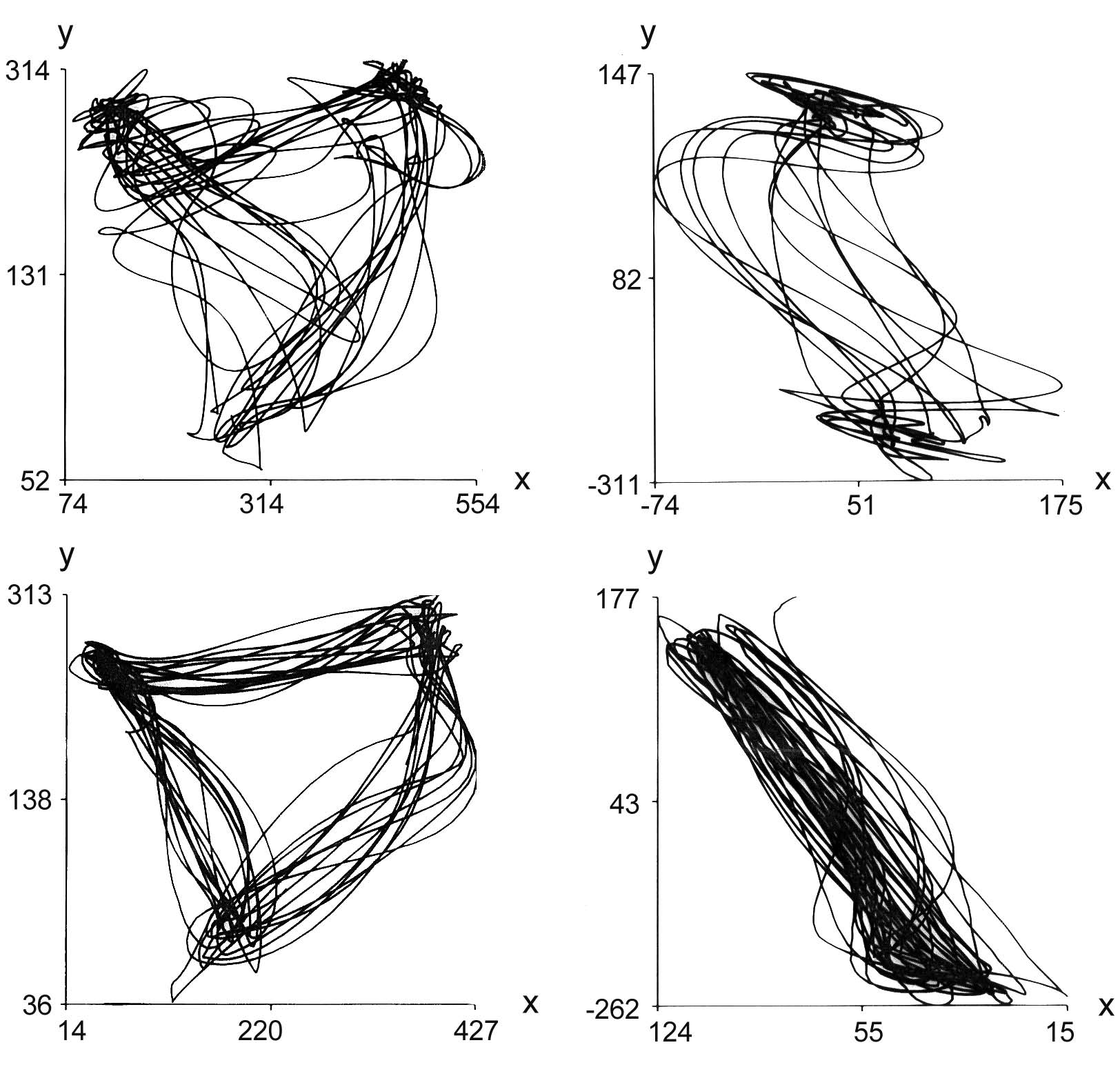
Fig. 3. Movement trajectories of a patient with the right arm affected in spatial coordinates (x–y in mm, absolute values with respect to the measurement system in the horizontal plane). Reach, grasp and transport movement (left-hand column) and sawing movement (right-hand column) before (upper row) and at the end of the study (bottom row). Sampling time: 60 s. The edge of the triangle (left-hand column) near the x-axis represents the resting point of the hand (refer to Methods).
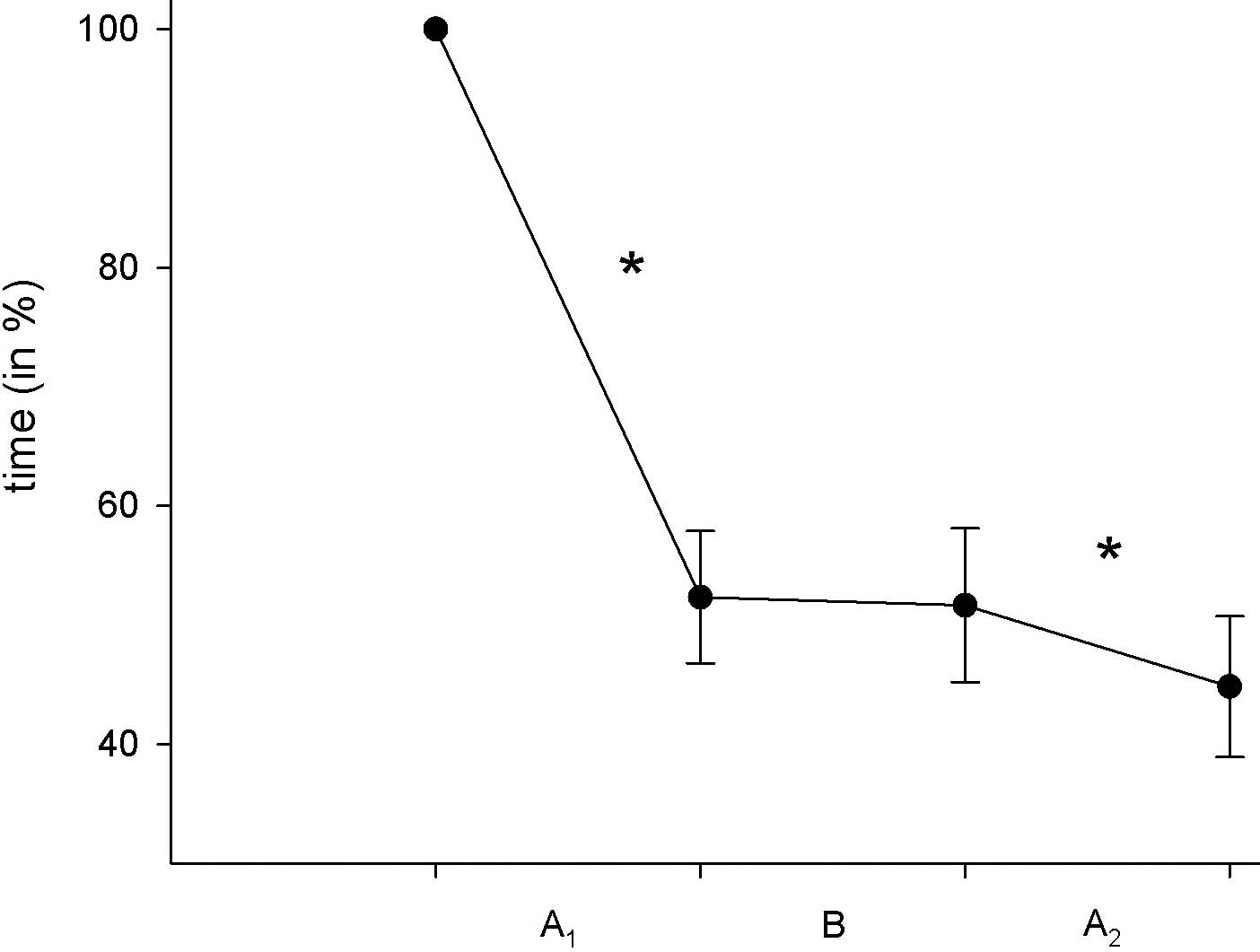
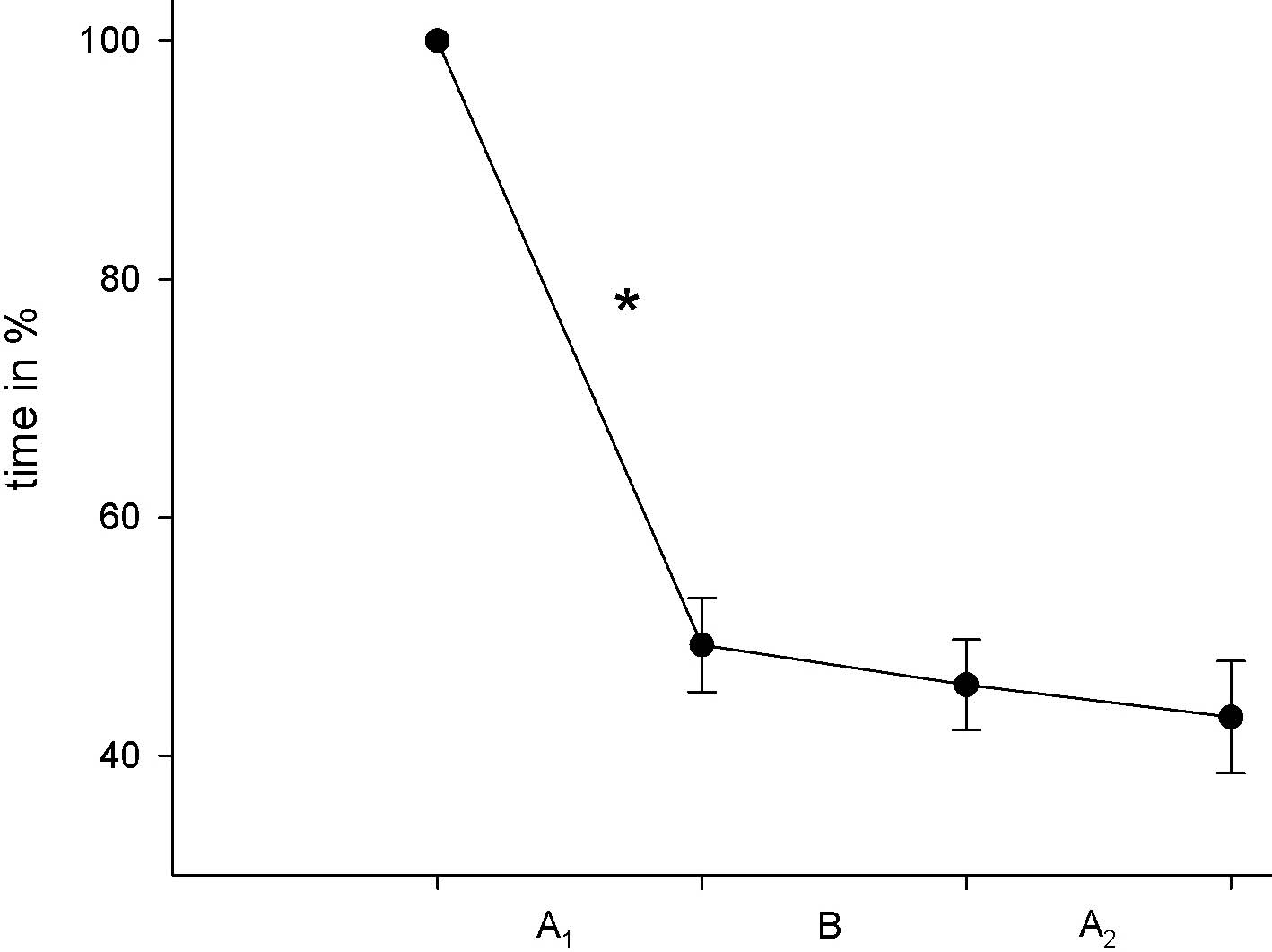
The sawing movement is a complex movement with accelerating and decelerating phases and one change of direction. Analysis of these different movement parts did not seem appropriate, as the study focussed on functional improvement and not on movement precision. Thus, we concentrated on 2 simple parameters: (i) the time needed for 20 complete movement repetitions (from start point forward and backward to the start point); and (ii) the peak velocities of the forward and backward movements, respectively. We found a considerable decrease of repetition time during the study (Friedmann test, p < 0.0001) with a significant improvement only during the training phases (A1: p < 0.0001, Z = –3.408, B: p = 0.244, Z = –0.783, A2: p = 0.006, Z = –2.442).
Since the peak velocities of forward and backward direction of the sawing movement were equivalent we analysed the pooled data of both directions. The movement velocity improved (Friedmann test, p < 0.0001) comparable with the repetition time, but showed a significant increase only during the training phases (A1: p < 0.0001, Z = –4.782, B: p = 0.320, Z = –0.483 and A2: p = 0.005, Z = –2.540). These results point to a specific effect of the repetitive training of complex movements (Fig. 4).
Fig. 4. Mean (± SEM) of time needed for 20 repetitions of the sawing movement expressed as ratio to the initial value. A1, A2: training phase; B: house-specific therapy. Asterisks indicate significant improvements. SEM: standard error of the mean.
For the grasping and transport movement we focussed on the peak velocities of the movement, as well as on the time needed for 20 complete movement repetitions (from start point moving towards the mug, grasping and transporting it to the next point and moving the hand back to the resting point). The analysis of the transport movement revealed significant velocity differences depending on movement direction (Wilcoxon, 2-tailed, p < 0.005). Movements from the affected side in the direction of the unaffected side in the frontal plane took more time than in the opposite direction.
The Friedmann test showed a highly significant improvement (p < 0.0001) for all these parameters during the study. This significant improvement took place during the first training phase A1 (p < 0.0001). During the phases B and A2 a further improvement occurred, but it did not reach statistical significance (Fig. 5).
Fig. 5. Mean (± SEM) of time needed for 20 repetitions of the reach, grasp and transport movement expressed as ratio of the initial value. A1, A2: training phase; B: house-specific therapy. Asterisks indicate significant improvements. SEM: standard error of the mean.
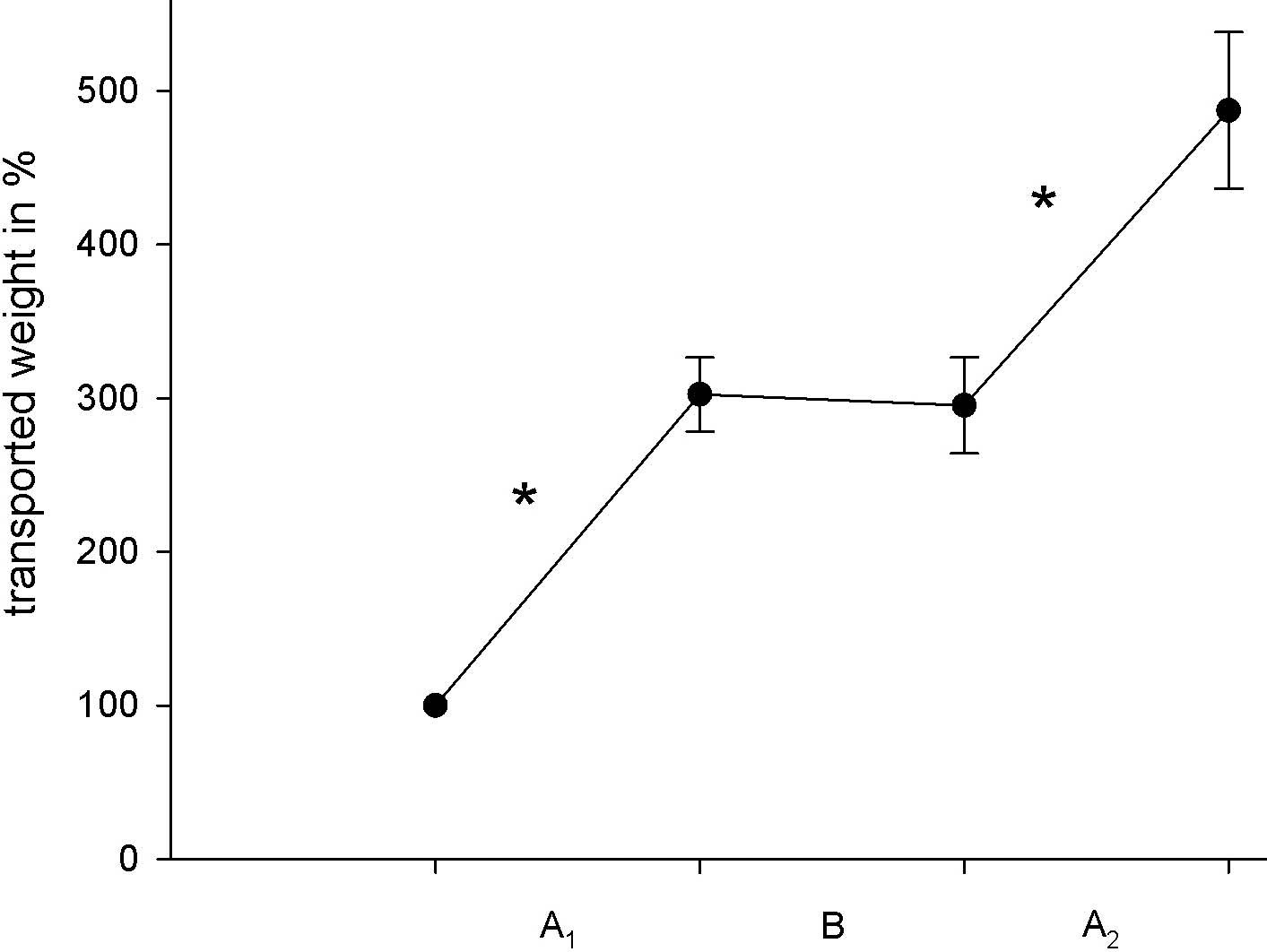
A central shaping element was increasing the weight of the transported mug. The training resulted in a highly significant increase in the weight during the training phases (A1 and A2, p < 0.0001) and a lack of further improvement during phase B (p = 0.727) (Fig. 6).
Fig. 6. Mean (± SEM) of the transported weight (sawing movement) expressed as ratio of the initial value. A1, A2: training phase; B: house-specific therapy. Asterisks indicate significant improvements. SEM: standard error of the mean.
DISCUSSION
This study is a sequel of our former study, in which we showed that repetitive training of complex arm movements did not result in a superior functional outcome compared with house-specific therapy (6). As a consequence of this negative finding we conducted the present study integrating shaping elements into the training paradigm and focussing on strength and velocity. Both studies showed a considerable improvement in all parameters during the whole observation time. The main difference was that, in the present study, we showed an advantage of repetitive training of complex movements incorporating shaping elements, since we found a highly significant improvement in biomechanical and movement parameters compared with house-specific therapy. At the start of phase B (house-specific therapy) the slope of the curves fell off, showing only a trend of further improvement (see Fig. 2, 4–6). In the second training phase (A2) the slope of the curves increased again. It was significant for the sawing movement and the transported weight only. Interestingly, the functional assessment (RMA) revealed a continuous increase throughout the whole study.
These results are in accordance with other studies using repetitive training of complex movements with shaping elements (9, 10, 22, 23) and a recent review pointing towards the effect of training of simple and complex movements on neuronal plasticity (24). The arm ability training introduced by Platz et al. (22) consists of 8 different complex tasks (tapping, turning coins, picking up bolts and nuts, placing objects, etc.) with an individually standardized workload. The initially performed repetitions during 1 min were considered as one block and the shaping element was the reduction of time needed for one block. For this training a significant functional improvement compared with the control group was shown. Shaping is also an essential part of CIMT, in its favour the therapeutic approach with the most of scientific evidence. Sterr & Freivogel (23) showed that even in low-functioning chronic hemiparesis a repetitive training of complex tasks lead to considerable functional improvements. As a shaping element they increased the difficulty of the tasks in small steps. A recent study analysing the contribution of shaping vs the restraint component of CIMT drew the tentative conclusions that shaping and task-practice may be equivalent training methods and that restraining the less-impaired arm may not be a critical therapeutic factor (25). In summary there is growing evidence, that shaping is a crucial element of successful therapeutic approaches. Our study supported this aspect, as the main difference of the training paradigm between the recent study and the study that failed to show effectiveness was the inclusion of shaping. However, this conclusion has to be drawn with caution because there are differences in the study design, and the impact of shaping elements was not studied within one controlled trial.
Movement analysis showed a reduced velocity of transport movements to the less affected side. Levin et al. (13) described more segmented and poorly coordinated movements to a contralateral target as a result of lack of coordination between shoulder and elbow joint movements. This disruption of coordination was obvious for movements within extensor synergies and, therefore, might be an explanation for the reduced velocity of the transport movement to the less affected side.
Patients received additional (40 min/day) therapy during the training phases, which added approximately 10 further hours of therapy during the training phase. The functional improvement might therefore be a result of higher therapeutic intensity. The amount of therapy is an important factor in stroke rehabilitation, but it has only a small impact on ADL and neuromuscular and functional outcome variables (26, 27). Another review stated that at least a 16 h difference in treatment time between experimental and control group administered during the first 6 months after stroke is needed to obtain a significantly different improvement in ADL (28). Furthermore, the effect of intensity was most pronounced during the first 12 weeks after stroke and the differences in efficacy subsequently became smaller (26). All patients were enrolled in this study within 12 weeks post-stroke. In a recent study, Platz et al. (29) compared passive therapy with active arm motor therapy as either individualized best conventional therapy or standardized impairment-oriented training. They concluded that specificity of active training seemed more important for motor recovery than intensity (therapy time). In the light of these data an intensity effect may have contributed to the results. On the other hand this argument also holds true for our former study with negative findings and the difference in treatment time is below the cut-off found by Kwakkel et al. (28). Therefore, it seems plausible to attribute the differences between phases A and B to the specific training rather than to the intensity.
Our training focussed on strength (increasing weight) and velocity, and these parameters improved most. Furthermore, we found the most evident training effect for the transported weight and the velocity of the sawing movement. This improvement was not reflected in grip strength or in RMA. The fact that the improvement in trained parameters is not transferred to other closely related parameters could be an expression of exercise-specificity. This is well known from sports, and means that the highest improvement can be achieved in that exercise-type that has been trained (30). Our house-specific therapy, in particular the occupational therapy, is task-specific and focuses on ADL. This may be an explanation for the continuous improvement in the RMA during all 3 phases.
The weakness of the present study is the small sample size, which could have caused the lack of significant improvement in the second training phase (A2) for some parameters. Nevertheless, the effect of the first training phase (A1) is remarkable and there is clear decline of the slopes with the beginning of phase B pointing towards a specific effect of the repetitive training of complex movements with shaping.
Crossover designs have the disadvantage of carry-over effects. Yet, the time course of the improvements and the length of phases make a relevant carryover effect unlikely. Phase A2 started after 6 weeks of intensive neurological rehabilitation. Therefore, we cannot rule out ceiling effects during phase A2, even though the RMA values show a continuous improvement.
In conclusion, repetitive training of complex movements including shaping elements leads to a significant improvement in the trained parameters. A relevant transfer to an improvement on a more functional level (RMA) could not be demonstrated. We conclude that, for the rehabilitation of the centrally paretic upper limb, a step-by-step approach starting with repetitive training of simple movements and continuing with complex movements, while each time incorporating shaping elements, is beneficial for functional outcome. To examine the contribution of single training parameters to functional improvement future investigations should focus on direct comparisons in randomized controlled trial (RCT) studies.
Conflict of interest
This is an investigator driven study without any funding. There are no financial or other conflicts of interest to be declared.
REFERENCES

