OBJECTIVE: To assess participation and health-related quality of life in adults with bilateral spastic cerebral palsy, and explore associations with self-efficacy.
DESIGN: Cross-sectional study.
SUBJECTS: A sample of 56 adults with bilateral spastic cerebral palsy (mean age 36.4 (standard deviation 5.8) years; 62% male).
METHODS: Daily activities and social participation (Life Habits 3.0), health-related quality of life (SF-36 Health Survey), demographic and clinical characteristics, and self-efficacy (General Self-Efficacy Scale (GSES-12)) were assessed. Associations were studied using multivariate logistic regression analyses.
RESULTS: At least 60% of the sample had difficulties with mobility, recreation and housing, and 44% had difficulty with personal care and employment. They perceived low health-related quality of life for physical functions, but not for mental functions. Corrected for demographic and clinical characteristics, general self-efficacy explained 49% of the variance in outcome on social participation, and the subscale Effort (GSES-12) 32% of the variance for the physical health-related quality of life and 16% of the mental health-related quality of life.
CONCLUSION: A significant number of adults with bilateral spastic cerebral palsy encountered difficulties in social participation and had a low perceived health-related quality of life for physical functions. Higher general self-efficacy or a greater willingness to expend effort in achieving behaviour was related to better participation and a higher physical and mental health-related quality of life.
Key words: cerebral palsy; adults; participation; quality of life, self-efficacy; rehabilitation.
J Rehabil Med 2010; 42: 528–535
Correspondence address: W. M. A. van der Slot, Rijndam Rehabilitation Centre, Westersingel 300, NL-3015 LJ Rotterdam, The Netherlands. E-mail: w.vanderslot@erasmusmc.nl
Submitted July 8, 2009; accept February 10, 2010
INTRODUCTION
In the past few years, adults with cerebral palsy (CP) have gained increasing attention (1–4). In general, emphasis has been placed on health issues and functional deterioration. Poor health may result in restrictions in activities and participation (2, 5, 6) and may affect quality of life (6–8). Participation and quality of life can be considered as relevant outcomes with regards to functioning. This study examines these outcomes in adults with CP and investigates associated factors.
According to the International Classification of Functioning, Disability and Health (ICF), participation is defined as the involvement of a person in life-situations and is determined by impairment or limitations of activity, as well as by environmental or contextual factors (9, 10). For adults with CP, restrictions in participation have been demonstrated in several areas of day-to-day living, including employment, independent living, and social and leisure activities (1, 5). Adults with unilateral CP performed relatively well in these areas (11), indicating less restricted participation than adults with bilateral CP (1). Objective information about adults with bilateral CP is scarce. The present study focuses on adults with bilateral CP, who seem to be more at risk of restrictions to participation.
Quality of life is defined as the individual’s perception of their position in life in the context of the culture and value systems in which they live, and in relation to their goals, expectations, standards and concerns (12). Health-related quality of life (HRQoL) refers to those aspects of life that are related to a person’s health status. Little is known about the standard of HRQoL in adults with CP. Two studies have been published so far; Gaskin & Morris (13) studied HRQoL in relation to physical activity in an Australian CP population and demonstrated that, in general, the patients had low levels of physical functioning and vitality. Jahnsen et al. (7, 8) reported that their results in most domains of HRQoL were significantly lower in adults with CP than those in a Norwegian reference sample.
For both outcomes of functioning, associated factors were assessed in previous studies, and a few of these also explored associations with self-efficacy. The concept of self-efficacy was introduced by Bandura (14) and is considered to be the belief of a person in his or her ability to organize and execute behaviours that are necessary for producing outcomes that the person desires. Self-efficacy does not reflect a person’s skills, but rather a person’s judgement of what they can do with their skills. There is evidence that self-efficacy is an important predictor for academic success, motivation and the functional well-being of people with disabilities, and that it is improvable by psychosocial interventions such as mentoring (15). In young adults with a disability, including CP, a higher level of self-efficacy was associated with participation (16). In the literature, several other associated factors for participation were addressed, including demographic factors, CP-related characteristics and environmental factors. Severe cognitive impairment, a low level of education, severe physical disability, and epilepsy were regarded as negative factors for being competitively employed and living with a partner (2, 6, 17). For HRQoL, physical functioning (13), pain and fatigue (4, 7) seemed to be important associated factors in adults with CP. Knowledge of associated factors is a prerequisite for the development of interventions needed successfully to rehabilitate patients with CP.
The aims of the present study were to study participation and HRQoL in adults with bilateral spastic CP without severe cognitive impairment, and to explore the factors associated with social participation and HRQoL, focusing in particular on self-efficacy.
METHODS
Study sample
Participants were recruited from 10 rehabilitation centres in the western and central regions of the Netherlands and, via the Association of Physically Disabled Persons and their Parents (BOSK). Historical registers of paediatric rehabilitation and current registers of adult rehabilitation were used to trace persons with CP. A letter with information on the study and an invitation to participate were sent to the persons with CP. To optimize the response, a reminder was sent 4 weeks later.
The inclusion criteria were: bilateral spastic CP in a person aged between 25 and 45 years at the time of inclusion. Exclusion criteria were: comorbidities with lasting effects on physical activity, contraindications for a progressive maximal cycle ergometer test (e.g. severe heart disease), full dependence on electric wheelchair propulsion, legal inability to participate, inadequate comprehension of the Dutch language and cognitive impairment preventing understanding the study instruction. This study is part of a larger one, and some of the inclusion criteria were required for measuring physical activity and fitness, which were part of that study (18).
Of a total of 208 eligible persons with CP, 56 participated (response rate 27%). Twenty-four percent did not respond to the initial invitation to join the study, and 10% could not be reached due to a change of address. Another 39% refused to participate, of which 61% gave a reason for non-participation: burden of the research, problems with the duration of assessment, a lack of time (54%); personal reasons that discourage them from participating, comorbidities and communication problems (28%); and no interest (18%). On average, participants were older than non-participants (mean difference 2.5 years; t-test, p < 0.01), but did not differ regarding gender or the distribution of impaired limbs (18).
All participants received verbal and written information about the study and gave their written consent to participate. The study was approved by the medical ethics committee of Erasmus MC and all of the participating rehabilitation centres.
Measurements
Data were collected in face-to-face interviews and/or with standard questionnaires administered in the presence of a trained researcher and by physical examination or functional tests. Because of face-to-face measurements there were only a few missing values (see Tables).
The following characteristics were determined: age, gender, level of education, neuromotor abnormality, gross motor functioning and functional level (Table I). Level of education was used as an indicator of cognitive functioning. We distinguished 3 levels of education: (1: low) no education, elementary school and pre-vocational practical education; (2: medium) pre-vocational theoretical education and upper secondary vocational education; (3: high) secondary non-vocational education, higher education and university. A physical examination was performed to assess the neuromotor abnormality. The classification system described in the Reference and Training Manual of the Surveillance of CP in Europe (SCPE) was used to classify persons with CP (19). Gross motor functioning was classified according to the Gross Motor Function Classification System (GMFCS), which is a 5-level classification system graded by the age-related severity of gross motor limitations (20). Distinctions between levels of motor functioning are based on functional limitations and the need for assistive devices (20). The GMFCS was originally developed and validated for children, but it has been shown to be reliable and valid for describing gross motor functioning in adults with CP (21).
The functional level was used to describe the study sample. This was assessed with a semi-structured interview based on the Functional Independence Measure (FIMTM), which includes 18 items that assess functioning in basic physical and cognitive abilities. Each item is scored on a scale of 7-levels from 1 (total assistance required) to 7 (complete independence). The items are grouped into a motor dimension (maximum score 91), a cognitive dimension (maximum score 35) and a total score (maximum score 126) (22). The FIMTM has been used in other studies of CP, and has excellent inter-rater and test-retest reliability intercorrelation coefficient (ICC) (0.95) (22, 23).
Activities and participation
The short version of the Assessment of Life Habits (LIFE-H 3.0) was used to evaluate functioning in daily activities and social participation. The LIFE-H 3.0 assesses performance in the accomplishment of daily activities and social roles, and the overall satisfaction with performance (24). The LIFE-H is composed of 69 life habits divided into 12 categories. The categories nutrition, fitness, personal care, communication, housing and mobility refer to daily activities; the categories responsibilities, interpersonal relationships, community life, education, employment and recreation address social roles. The performance score is based on 2 concepts: the level of difficulty when performing a life habit, and the type of assistance required to perform the habit. Both elements are combined in a scale ranging from “not accomplished or achieved” (0), indicating total handicap to “accomplished without difficulty” (9), indicating optimal activity or participation. Specific life habits that were not part of a respondent’s lifestyle because of personal choice were marked as “not applicable”. Mean scores were calculated for each category, for the daily activities and social participation sub-domains and total score. We regarded a mean score < 8.0 on the LIFE-H as representing difficulties (25).
The LIFE-H comprises a second scale that evaluates the individual’s level of satisfaction with the accomplishment of life habits. Satisfaction is rated on a 5-point Likert scale; varying from very dissatisfied (1) to very satisfied (5).
The LIFE-H has been shown to be reliable for different groups of adult patients; also the Dutch language version of LIFE-H (26). The reliability and validity of the satisfaction scale have not yet been studied.
In addition to the LIFE-H, we assessed several indicators of participation. These were related to employment status, civil status, living status and whether or not the respondents had children (Table II).
Health-related quality of life
HRQoL was assessed using the Short Form-36 Health Survey (SF-36). The SF-36 is designed to measure 8 health domains on the basis of the participant’s perceived burden of his or her illness: physical functioning, role limitations due to physical health problems, bodily pain, general health, vitality, social functioning, role limitations due to emotional problems and mental health. A composite score for the SF-36 domains was calculated from the raw scale scores using a Z score transformation (score range 0–100) (27). In addition, scores were summarized by 2 scale scores: a physical component summary scale (PCS) and a mental component summary scale (MCS), which were expected to have a mean of 50 (SD 10) in the general population of the USA (27). These scales are used as a measure of participants’ overall HRQoL. Higher scores indicate a better HRQoL. Psychometric evaluation and reference values were available for the Dutch population (28, 29).
Self-efficacy
We assessed the participants’ self-efficacy by using the Dutch language version of the General Self-Efficacy Scale-12 (GSES-12) (30, 31). The scale consists of 12 items that are scored on a 5-point Likert scale. The scale is divided in 3 subscales: (1 = Initiative) willingness to initiate behaviour; (2 = Effort) willingness to expend effort in completing the behaviour; and (3 = Persistence) defined as persistence when facing adversity. The total scale and subscales showed satisfactory levels of internal consistency (Cronbachs’ alpha 0.63–0.69) (30) and test-retest reliability (r = 0.67) (32).
Statistical analysis
Analyses were performed using SPSS 12.0.1 for Windows. Results were described with descriptive statistics.
Indicators of participation were compared with the Dutch population, using data available from the Central Bureau of Statistics (for years 2005–2007) (33), with a binomial test.
One-sample t-tests were used: (i) to compare scores of the SF-36 with Dutch reference groups: a group aged 16–40 years for domain scores (28), and a group aged 20–49 years for PCS and MCS scores (29); and (ii) to compare scores of the GSES-12 with a Dutch reference group, mean (SD) age 46.9 (18.1) years (34). For all analyses, p-values ≤ 0.05 were considered to be significant.
To study associated factors of participation and HRQoL, univariate and multivariate logistic regression analyses were performed. Univariate analyses addressed relationships between demographic and clinical characteristics (age, gender, gross motor functioning, level of education and general self-efficacy) and indicators of participation, participation and HRQoL. For 4 dependent variables we explored multivariate models: “daily activities” and “social participation” of the LIFE-H and physical and mental HRQoL (PCS and MCS). Accommodating to the number of independent variables we included level of education, gross motor functioning and self-efficacy (General scale and Effort subscale) as independent variables. Because the dependent variables were not normally distributed the scores were dichotomized. For the sub-domains “daily activities” and “social participation” of the LIFE-H, individuals were classified as either having difficulties (0) or no difficulties (1). For the PCS and MCS of the SF-36, a mean score < 50.0 indicated a lower level of HRQoL (0) and a mean score ≥ 50.0 demonstrated a higher level of HRQoL (1). Of the independent variables, the GMFCS level was categorized into 3 groups: I, II, III/IV; none of the participants had a GMFCS level V. Because clinically relevant cut-off points for good and poor GSES-12 total and subscale scores are unknown, these scores were dichotomized based on the median of the study sample, identifying persons with relatively low (0) and high scores (1) (35). Odds ratios (OR), including 95% confidence intervals (95% CI), and explained variances (R2, Nagelkerke R square) of the regression models are presented.
RESULTS
Characteristics of the study sample
Table I presents the personal characteristics and functional level of the 56 adults with bilateral CP who participated in this study. The mean age was 36.4 years (SD 5.8) and 62% were male. Seventy-three percent of participants had a high level of GMFCS (level I or II). Seventy-three percent had a medium or high level of education. Participants had a high degree of independence in performing functional activities according to the FIMTM, with a mean total score of 117 (SD 9.4) out of a maximum of 126.
Daily activities and participation
The indicators of participation are shown in Table II. Sixty-eight percent of the adults with CP were in paid employment, including 54% who were in competitive employment and 14% in sheltered employment. In comparison, 77% of the overall Dutch population, aged 25–45 years, had paid employment (p = 0.08) (33). Of the adults with CP, 27% were married or living with a partner. This percentage is low compared with a cohort of age-matched Dutch people (70%) (p < 0.001). A difference was also found with regards to having children: 11% of the adults with CP had children compared with approximately 50% of Dutch households in the 25–45 years age group (p < 0.001) (33).
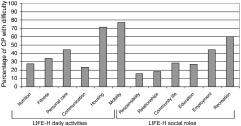
The mean scores of daily activities and social participation as measured with the LIFE-H are shown in Table III. According to the high mean scores in most categories, the participants function relatively well. However, according to the variance around the mean scores, a substantial number of subjects are restricted in their activities and social participation. In Fig. 1, the percentage of participants with difficulty in each LIFE-H category is presented. With regards to daily activities, most adults with CP encountered difficulties in mobility (77% of the participants) and housing (71%) despite the use of assistive devices, adaptations or humane assistance. Assistive devices used for mobility were a wheelchair (54%), a tricycle (39%), a scoot mobile (21%), a moped (7%) or a handbike (2%). Approximately half of the participants used a car, of which 11% were adapted.
Fig. 1. Percentage of adults with cerebral palsy (CP) with difficulty in each (Assessments of Life Habits (LIFE-H) category.
Regarding housing, 36% of the participants had a house with adaptations, 7% lived in a house with outside assistance on call, and 4% lived in an institution. Informal caregiver assistance was used by 16% and professional household assistance by 32%. With regards to personal care, 45% of the adults with CP had difficulties and at least 4% used professional assistance.
Regarding social participation, 60% of the participants had difficulty in recreational activities and 44% with employment. Difficulty in daily activities and social participation did not differ between men and women with CP. Only the category “mobility” showed a significantly lower mean score for women with CP than men, 6.2 (1.6) vs 7.1 (1.1) (p = 0.015).
Participants were mostly satisfied with their performance of daily activities and social participation on the LIFE-H (Table III). They were the most dissatisfied with their interpersonal relationships, with a mean score of 3.4 (0.5) of a maximum of 5.
Health-related quality of life
The HRQoL of the study sample is shown in Table III and compared with Dutch reference values (28, 29). Adults with CP perceived a significantly lower HRQoL for most domains, except for role limitations due to emotional problems and mental health. Regarding the PCS, participants perceived a relatively low HRQoL. On the MCS women with CP had a better score (53.7 (SD 11.5)) than women in the reference group (46.7 (p = 0.01)). No difference was found between men in the 2 groups. Between men and women with CP, no significant differences were found.
Self-efficacy and its associations with daily activities, participation and HRQoL
General self-efficacy did not differ between adults with CP and a Dutch reference group, with a total score of 47.0 (SD 6.3) vs 46.3 (SD 7.7) (p = 0.44) (see Table IV). Adults with CP scored significantly better on the persistence subscale than did the reference group (21.3 (SD 2.8) vs 19.8 (SD 3.3), (p < 0.001)).
For the indicators of participation presented in Table II no correlations were found by univariate regression analyses with age, gender, gross motor functioning, level of education and general self-efficacy, except for employment, which was associated with age (OR = 0.8; p = 0.001, R2 = 30%). However, in multivariate models these determinants were not significant. In multivariate analyses, a higher level of gross motor functioning appeared to be positively associated with both daily activities (OR = 4.6; p ≤ 0.01) and social participation (OR = 10.5; p ≤ 0.01). In addition, general self-efficacy contributed to social participation (OR = 6.2; p ≤ 0.05). The multivariate models explained 40% of the total variance of functioning in daily activities and 49% in social participation (Table V).
For the physical and mental HRQoLs, we found that corrected for demographic and clinical characteristics the self-efficacy Effort subscale explained 32% and 16% of the variance in outcome, respectively (Table VI). Participants with better gross motor functioning were 6 times more likely to perceive a higher physical HRQoL (p ≤ 0.01). Participants with a higher score on the Effort subscale of GSES-12 were 7.6 times more likely to perceive a higher physical HRQoL (p ≤ 0.05) and 3.5 times more likely to perceive a higher mental HRQoL (p ≤ 0.05). Age, gender, level of education and general self-efficacy were not associated with mental and physical HRQoL.
DISCUSSION
Participation, health-related quality of life and associated factors
The present study investigated participation and HRQoL in adults with bilateral spastic CP without severe cognitive impairment. We found that, regarding employment, civil status, and having children, adults with CP are in a disadvantaged position compared with the Dutch reference population. Being involved in participation, varies between this study and that reported in other recent studies carried out in Scandinavian countries and the USA, which also focused on adults with CP without severe learning disabilities (1, 7, 17). Although these study samples differed regarding neuromotor abnormality and distribution of limb impairment, they provide the best available reference descriptions of participation in adults with CP. For example, 54% of the adults in our study were found to be competitively employed compared with 33% in the study by Jahnsen et al. (7). In addition, 14% of our subjects were engaged in sheltered employment compared with 18% in the study by Murphy et al. (17). Previous studies have shown that adults with unilateral CP are more often competitively employed than those with bilateral CP (1, 6, 11). Sixteen percent of subjects in the present study reported receiving a disability pension compared with 46% in Jahnsen et al. (7). Difference in age between the study group of Jahnsen (7) and our sample might be of relevance in these figures on employment and disability pension, which is underlined by the association between age and employment in our sample.
The percentage of adults with CP who are married or living with a partner varies from 14% (1) to 27% (this study). Several aspects might possibly contribute to this low percentage of being married or living with a partner: a negative perception of the body (36), limited participation together with able-bodied persons (e.g. special education, sheltered employment), and more restricted to activities at home. Wiegerink et al. (37), showed that Dutch young adults with CP had less experience with dating, romantic relationships and sexuality compared with Dutch age mates. They also demonstrated the importance of participating in peer group activities for having a partner or sexual relationships (38). Rates of living independently vary from 65% (7) to 90% (this study), and rates of living with parents range from 7% (this study) to approximately 33% (17). The percentage of participants who have children ranges from 4% (17) to 11% (this study), with an outlying exception of 22% in the study by Jahnsen et al. (7). Studies that included adults with CP who had learning disabilities reported lower percentages for living independently and having children (39).
A significant number of adults with CP in our study reported having difficulties with daily activities and social participation, especially in mobility, housing, recreation and employment. Similar results were found in other studies (1, 5, 17, 39). In contrast, adolescents and young adults with CP aged from 16–20 years (25) experienced fewer difficulties in daily activities and social participation than our sample, which might be due to a large percentage of unilaterally involved persons, their younger age and the increased likelihood that they still live with their parents.
The results of our study add to the evidence that self-efficacy may contribute to better social participation. This is in accordance with the study by Bent et al. (16) of young adults with a disability, including CP. They found no differences in self-efficacy rates between disabled and non-disabled young adults. Also, in our study, scores for general self-efficacy are comparable to the reference group, except for the higher scores on persisting in the face of adversity. It is possible that persons with CP have learned to persevere to reach their goals, because of their lifelong disability with barriers.
In addition to participation, this study focused on self-perceived HRQoL, addressing health-related aspects and their perceived impact on functioning. Adults with bilateral CP perceived a low HRQoL for physical functions but not for mental functions. This is in line with other studies that used the SF-36 (7, 8, 13). Women with CP had a high mental HRQoL compared with the reference population. Participants with better gross motor functioning were more likely to have a higher physical HRQoL. Livingston et al. (40) reported that the gross motor functioning of children and adolescents with CP was positively correlated with physical functions and physical well-being, but did not consistently correlate with psychosocial well-being. Participants who work hard to achieve their goal (resulting in a higher score on the self-efficacy Effort subscale) were more likely to have a higher physical and mental HRQoL.
Our model for mental HRQoL explained only 16% of the variance in outcome, which is low. This is not surprising, because mental HRQoL could be influenced by different factors that were not included in this study, such as personality, coping styles and social support. The association between self-efficacy and HRQoL is in accordance with the theory of Bandura (14). He assumed that perceived functioning may be controlled more by beliefs of capability than by the degree of physical impairment, because the latter is not consistent with a patient’s perceived quality of life.
Study limitations
A limitation of this study was the low response rate. Only a few adults with CP were currently following a rehabilitation programme (5%).Therefore we had to use a broad approach to include adults with bilateral CP by also searching the historical registers of rehabilitation centres and actively approaching the patients’ association to recruit participants. Non-response was due mainly to a lack of up-to-date contact information for potential participants. Furthermore, the burden of the research, including extensive measurements of physical activity and fitness for other parts of the larger study (18), especially in combination with their physical disability, the patient’s lack of time available to participate, or lack of interest in the study, e.g. because of a history of extensive medical treatments, were reasons for non-response. Our sample was comparable for gender and level of education to the subgroup of adults with bilateral CP without severe cognitive impairment included in the study of Van der Dussen et al. (39). In the latter study the sample was checked to be a nearly complete incidence cohort for the region of The Hague, which is part of the recruitment area of the present study (39). Therefore we assumed the results to be representative for the subpopulation of adults with bilateral CP and normal intelligence. In our opinion, studying subpopulations is a prerequisite for the adequate investigation of functioning and associated factors, thus handling the heterogeneity that is a characteristic of CP. Comparison with other studies in this field is limited because of different selection criteria (e.g. age, subtypes of CP), use of different measurement instruments, and cultural and economic differences (e.g. different levels of unemployment in different regions). The lack of an age-matched control group was resolved by using Dutch reference data.
Implications for treatment
In conclusion, a significant number of adults with bilateral spastic CP without severe cognitive impairment encounter difficulties in daily activities and social participation. Adults with CP perceived a relatively low HRQoL for physical functions, but not for mental functions. Optimizing participation in this age group is desirable, especially for mobility, housing, recreation and employment. As self-efficacy was associated with social participation and the Effort subscale with physical and mental HRQoL, psychosocial interventions to improve self-efficacy may enhance both the objective and self-perceived levels of functioning in adults with CP.
ACKNOWLEDGEMENTS
This research was supported by grants from the Johanna Child Fund (JKF) and the Child Fund Adriaanstichting (KFA). We thank all the participants. We acknowledge Helen Luiting for her contribution to the data collection. The following members of the Transition Research Group South West Netherlands contributed to this study: Department of Rehabilitation Medicine, Erasmus MC, University Medical Centre, Rotterdam (W. G. M. Janssen, MD); Rijndam Rehabilitation Centre, Rotterdam (M. P. Bergen, MD PhD, R. F. Pangalila, MD); Sophia Rehabilitation, The Hague (W. Nieuwstraten, MD) and Delft (M. Terburg, MD); Rijnlands Rehabilitation Centre, Leiden (H. vd Heijden-Maessen, MD); Department of Rehabilitation Medicine, Leiden University Medical Centre (J. H. Arendzen, MD PhD); Rehabilitation Centre “de Waarden”, Dordrecht (H. J. R. Buijs, MD); and the Foundation of Rehabilitation Medicine Zeeland, Goes (B. Ras, MSc, T. Voogt, MSc). In addition, we thank the Department of Rehabilitation of Maasstad Hospital, Rotterdam (P. J. Janssens, MD), VU Medical Centre, Amsterdam (A. J. Dallmeijer, PhD), the Rehabilitation Centre de Trappenberg, Huizen (A. Beelen, PhD) and the Association of Physically Disabled Persons and their Parents, BOSK, who cooperated in this study.
REFERENCES