OBJECTIVE: To compare the efficacy of three 12-month training programmes on headache and upper extremity pain in patients with chronic neck pain.
METHODS: A total of 180 female office workers, with chronic, non-specific neck pain were randomly assigned to 3 groups. The strength group performed isometric, dynamic and stretching exercises. The endurance group performed dynamic muscle and stretching exercises. The control group performed stretching exercises. Pain was assessed with a visual analogue scale. Each group was divided into 3 subgroups according to headache intensity.
RESULTS: At the 12-month follow-up headache had decreased by 69% in the strength group, 58% in the endurance group and 37% in the control group compared with baseline. Neck pain diminished most in the strength group with the most severe headache (p < 0.001). In the dose analysis, one metabolic equivalent per hour of training per week accounted for a 0.6-mm decrease in headache on the visual analogue scale. Upper extremity pain decreased by 58% in the strength group, 70% in the endurance group and 21% in the control group.
CONCLUSION: All of the training methods decreased headache. However, stretching, which is often recommended for patients, was less effective alone than when combined with muscle endurance and strength training. Care must be taken in recommending the type of training to be undertaken by patients with severe cervicogenic headache.
Key words: cervical headache; cephalalgia; neck pain; disability; strength training; stretching; aerobic exercising.
J Rehabil Med 2010; 42: 344–349
Correspondence address: Jari Ylinen, Central Hospital of Central Finland, Department of Physical and Rehabilitation Medicine, Keskussairaalantie 19, FI–40620 Jyväskylä, Finland. E-mail: jari.ylinen@ksshp.fi
Submitted June 11, 2009; accepted December 15, 2009
INTRODUCTION
Cervical headaches are estimated to affect approximately 2.5% of the adult population and account for 15–20% of all chronic and recurrent headaches (1). Headache and neck pain are the most common reasons for visits to a physician at the primary level of healthcare among working age women in Finland (2). The aetiology of headaches remains largely unknown. Trauma is found in only a minority of cases. Degenerative changes in the cervical vertebrae and discs are common even in asymptomatic people. These degenerative changes also increase with advanced age and have not shown a clear correlation with chronic pain (3, 4).
Head pain, which is referred to the head from bony structures or soft tissues of the neck, is commonly termed cervicogenic headache. The classification of cervicogenic and other types of headache is controversial as it relies mainly on clinical symptoms, which vary greatly between individuals and may also vary over time. It has been questioned whether cervicogenic headache is an independent entity or a tension type of headache with a cervical trigger or migraine (5, 6).
The co-occurrence of headache has been found to be 4 times higher in individuals with musculoskeletal symptoms than in those without (7). In particular, individuals with neck pain have been found to experience headaches more frequently than those with symptoms in other areas.
Neck and upper limb pain commonly cluster. The odds of experiencing pain in different parts of the arm have been shown to be 4 times higher in subjects with neck pain than in those with no neck pain (8). However, we did not find any study on the effectiveness of a randomized neck exercise intervention that reported on upper limb pain.
Conservative management of neck disorders often includes passive therapies, which have not been shown to be effective (9). Several randomized controlled studies have shown specific neck muscle exercises to be effective treatment in cases of chronic neck pain (9–12). However, only Jull et al. (13) have reported neck exercises to be effective in treatment of cervicogenic headache.
We have shown previously that isometric strength and dynamic endurance training of neck muscles may relieve or even completely eliminate pain and restore function in patients with chronic neck pain (12). However, little is known about the effectiveness of different exercises on the symptoms associated with neck pain. The primary aim of the present study was to determine whether exercise therapy also relieves headache and arm pain associated with neck pain. The second aim was to analyse whether the presence of headache indicates a more severe condition, with consequent negative effects on the outcome of exercise therapy in patients with chronic neck pain. The third aim was to analyse the dose-response relationship of the specific strength and endurance training regimens for the cervical muscles to reduce cervicogenic headache.
METHODS
Study design and recruitment of patients
The study design and data with regards to neck pain has been published previously (12). This study was an examiner-blinded, randomized, controlled trial. Physicians working in occupational healthcare services referred patients with long-standing neck pain to the Punkaharju Rehabilitation Center, Punkaharju, Finland. A questionnaire was posted to applicants to confirm their status. The following inclusion criteria were used: female gender, age 25–53 years, office-worker, permanently employed, motivated to continue at work, motivated for rehabilitation, and constant or frequently occurring neck pain over at least 6 months.
Exclusion criteria were: specific disorders of the cervical spine, such as disc prolapse, spinal stenosis, post-operative conditions, history of severe trauma, instability, spasmodic torticollis, as well as frequent migraine (more often than twice per month), peripheral nerve entrapment, fibromyalgia, shoulder diseases, inflammatory rheumatic diseases, severe psychiatric illness and other diseases preventing physical loading, and pregnancy. These states were assessed by medical history and a clinical examination prior to entering the study.
A total of 180 female office-workers were selected and all provided their written consent before entering the study. When 30 referrals had been received, each subgroup was ranked by the Neck and Shoulder Pain and Disability Index and divided into 10 blocks of 3 subjects (14). One subject from each block was then randomized into a strength training group (SG), one into an endurance training group (EG) and one into a control group (CG) by a computer programme (15).
Outcome assessment
Measurements were taken at baseline and after the 12-month intervention period. Perceived headache, neck and upper limb pain during the previous week were assessed by visual analogue scale (VAS) and disability by Vernon’s Neck Disability Index (16, 17). For each scale the theoretical range is 0–100. In order to evaluate the effect of headache on the severity of neck pain all the subjects were divided into 3 groups according to intensity of headache as measured by VAS: group I (0–24) had no or minor headache, group II (25–54) moderate headache and group III (55–100) severe headache. The cut-points were selected on the basis of research evidence obtained from the VAS, adjusted to take into account the distribution of data (18). Patients were assessed for maximal isometric neck strength in the neutral position (19) and range of motion (ROM) in flexion, extension and rotation (20). For the dose analysis, maximal oxygen uptake was measured with a submaximal bicycle ergometer test by an exercise physiologist (21). Physical activity, defined as any bodily movement produced by skeletal muscle contractions that substantially increases energy expenditure (22, 23), was estimated from data obtained by a 4-week (28 days) all-time recall questionnaire. Information on the specific training programmes and other activities was also collected via a training diary throughout the 12-month intervention. All activities were converted into metabolic equivalents (METs) by specific software (MetPro 2.03.7, Sci Reha, Jyväskylä, Finland). Both the questionnaires and the diaries were administered by the same physical therapist during the participants’ institutional control visits. The head researcher, biostatistician and tester were all independent of the rehabilitation institution.
Description of interventions
Each training group of 10 subjects started with a 12-day institutional rehabilitation programme, during which they were instructed in a home-exercise programme. The SG and EG training regimens consisted of five 45-min sessions per week. Every other session was performed at only half intensity to avoid excessive loading. The neck flexor muscles were exercised in the EG by lifting the head up from the supine position in 3 series of 20 repetitions and in the SG by pushing a Theraband® in the sitting position in 1 series of 15 repetitions forwards, obliquely towards the right and left, and backwards (24). Both groups carried out dynamic exercises for the shoulders and upper extremities by performing dumbbell shrugs, presses, curls, bent-over rows, flyes and pullovers. The EG performed 3 sets of 20 repetitions for each exercise with a pair of dumbbells each weighing 2 kg. Thus, repetitions and load were kept constant throughout the training period. The SG exercised with an individually adjusted single dumbbell and performed only 1 set of 15 repetitions for each exercise at the highest possible load. Both training groups thereafter performed exercises in the same way for the trunk and leg muscles against their body-weight by doing a single series of squats, sit-ups and back extension exercises. Each training session was finished by stretching exercises for the neck, shoulder and upper limb muscles. Both training groups also underwent a multimodal rehabilitation programme, including aspects commonly associated with the traditional neck school. They also received 4 sessions of physical therapy, consisting mainly of massage and mobilization, to alleviate neck pain and to enable those with severe neck pain to perform the physical exercises effectively. The CG was advised to perform aerobic exercise 3 times a week for half an hour. They received written information about the same stretching exercises as carried out by the training groups, which they were to practise at home for approximately 20 min, and were trained in the correct way to perform these exercises. They received no treatments. All 3 groups were instructed to exercise regularly 3 times a week at home. Control visits for motivating participants to continue exercise training were organized after 2 and 6 months from the baseline assessment. The training regime of the EG and SG was checked at these follow-ups.
Data analysis
The clinical outcome variables were used for intention-to-treat analysis. The results are expressed as means and standard deviations (SD), and median and interquartile ranges (IQR). Statistical comparison between the groups was carried out using the t-test, Cochran-Armitage trend test, Mann-Whitney test, analysis of variance (ANOVA) with the Tukey HSD (Honestly Significantly Different) test and Kruskal-Wallis test. Hommel’s adjustments were used to correct significance levels for multiple and post hoc testing. Hodges-Lehmann estimate of median difference with a 95% confidence interval (95% CI) was used to determine changes in the clinical outcome variables. The normality of variables was evaluated using the Shapiro-Wilk statistic. To determine the predictors of change in cervicogenic headache (VAS) first, a correlation analysis was conducted. The variables selected for correlation with change in headache were energy expenditure during the specific neck training, energy expenditure during work, commuting, leisure, and miscellaneous activity, headache at baseline, study group (SG vs EG), and age. Secondly, on the basis of the variables suggested by the correlation analysis, a forced entry model was conducted to determine the contribution of the different variables to reported change in cervicogenic headache. Accordingly, headache at baseline, SG, age, energy expenditure during work, change in energy expenditure during leisure-time physical activity, and energy expenditure during the specific training programme were entered into the forced model. The α level was set at 0.05 for all tests.
RESULTS
One subject in the EG was diagnosed with polymyalgia rheumatica after randomization and was thus excluded from the study. One subject withdrew from the EG and 1 from the CG. These 2 subjects were included in the intention-to-treat analysis. The training groups and the control group did not differ in demographic data and nor did the subgroups formed when the subjects were classified according to headache intensity (Table I). However, a similar difference in pain intensity and in the disability index was observed between the subgroups. In the severe neck pain group (III) pain had lasted longer than in either of the other 2 groups. Also, pain in the upper limb was more severe in group III, while no difference was found between the other 2 groups. There was no significant difference between groups in how much they achieved, measured as maximum oxygen uptake, neck muscle strength and ROM.
| Table I. Mean baseline (and standard deviation (SD)) characteristics of the subjects in group I with no or minor neck pain (VAS 0–24), group II with moderate neck pain (VAS 25–54) and group III with severe neck pain (VAS 55–100) |
| | Group I (n = 57) | Group II (n = 59) | Group III (n = 63) | p-value* |
| Demographics, mean (SD) | | | | |
| Age, years | 47 (5) | 45 (6) | 45 (6) | 0.22 |
| Height, cm | 164 (5) | 166 (5) | 163 (8) | 0.44 |
| Weight, kg | 70 (12) | 69 (9) | 66 (11) | 0.047 |
| Body mass index | 25.8 (3.5) | 25.0 (3.1) | 24.6 (3.9) | 0.074 |
| Clinical data | | | | |
| Duration of neck pain, years, mean (SD) | 6.9 (5.9) | 8.4 (5.9) | 9.3 (5.9) | 0.032 |
| Neck pain, VAS, mean (SD) | 49 (20) | 51 (17) | 70 (18) | < 0.001 |
| Upper limb pain, VAS, mean (SD) | 31 (26) | 32 (24) | 43 (28) | 0.008 |
| Vernon index, mean (SD) | 19 (8) | 21 (8) | 27 (9) | < 0.001 |
| Smoking, n (%) | 11 (19) | 8 (14) | 13 (21) | 0.83 |
| Achievement, mean (SD) | | | | |
| VO2peak, ml/kg/min | 31 (4) | 33 (6) | 31 (5) | 0.65 |
| Isometric neck strength | | | | |
| Flexion | 59 (17) | 57 (18) | 55 (20) | 0.28 |
| Extension | 136 (35) | 132 (38) | 130 (40) | 0.43 |
| Neck ROM, degrees | | | | |
| Flexion to extension | 125 (16) | 126 (12) | 122 (13) | 0.16 |
| Rotation | 156 (18) | 163 (13) | 160 (16) | 0.22 |
| *p-value for linearity. N: Newton; ROM: range of motion; VAS: visual analogue scale; VO2peak: maximum oxygen uptake; SD: standard deviation. |
At baseline, the intensity of headache and pain in the neck and upper extremities was at the same level in all 3 groups (Table II). The decrease in headache intensity measured by VAS, of 69% in the SG, 58% in the EG and 37% in the CG, was significant compared with baseline values. However, a significant inter-group difference emerged only between the SG and the CG. The decrease in upper extremity pain, of 58% in the SG, 70% in the EG and 21% in the CG, was also significant compared with baseline values. Each training group showed a significant difference compared with the CG. The relative decrease in neck pain paralleled that of headache in the SG (69%) and was almost similar magnitude in the EG (61%) and the CG (28%).
| Table II. Pain ratings of subjects at baseline and changes (with confidence intervals (CI)) at follow-up measured by visual analogue scale (VAS) |
| Pain area | Baseline | Change to months 12 | p-value between groups (multiple comparison†) |
| Controls | Endurance | Strength | Controls | Endurance | Strength |
| Median (IQR) | Median (IQR) | Median (IQR) | Median (95% CI*) | Median (95% CI*) | Median (95% CI*) |
| Head | 41 (19, 68) | 43 (13, 61) | 42 (21, 64) | –15 (–23 to –8) | –25 (–33 to –16) | –29 (–38 to –21) | 0.028 (S/C) |
| Neck | 58 (42, 74) | 57 (43, 74) | 58 (43, 72) | –16 (–22 to –9) | –35 (–42 to –28) | –40 (–48 to –32) | < 0.001 (S/C, E/C) |
| Upper extermities | 38 (13, 55) | 30 (7, 61) | 36 (7, 57) | –8 (–14 to –1) | –21 (–30 to –12) | –21 (–28 to –13) | 0.018 (S/C, E/C) |
| *Hodges-Lehmann estimates of median difference. †Mann-Whitney test and p-value adjusted using Hommel’s method. C: control group; CI: confidence interval; E: endurance group; IQR: interquartile range; S: strength group. |
When the subgroups were analysed separately, a significant difference in change in neck pain was found in the SG; those with severe headache showed the greatest reduction in neck pain at the 12-month follow-up (Fig. 1). However, the intensity of headache did not make any statistically significant difference to the change in neck pain in the EG or the CG.
Fig. 1. Change in neck pain in subgroups of patients with minor (I, n=57), moderate (II n=59) or severe (III n=63) headache. The strength group performed isometric neck and dynamic upper extremity exercises. The endurance group performed dynamic neck and upper extremity exercises and all groups including the control group performed stretching exercises.
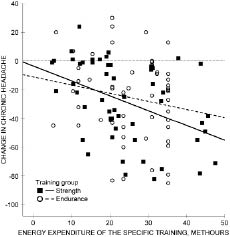
Dose analysis of the specific training applied to reduce headache showed that energy expenditure during the training correlated negatively with the pain scores, accounting for 12% of the total variation predicted by the model. The total variation predicted by the model was 54%. In the specific training programme, 1 METh (metabolic equivalents per hour) accounted for a 0.6 mm (95% CI 0.3–0.9 mm) decrease in headache experienced. Headache intensity at baseline accounted for 46% of the total variation predicted by the model; that is, the participants with the highest pain scores at baseline benefited most from the training programme. The intervention group (SG vs EG) was not a predictor of change in headache; both training modes relieved the participants’ headache significantly. Approximately 20 trainees, whose volume of training was under 9 METh per week, did not report a reduction in headache, while approximately 100 trainees did. Also, all the subjects whose training intensity was 10 METh per week or more reduced, or at least maintained, their baseline headache intensity. All but 1 of the aforementioned trainees were in the SG (Table III, Fig. 2).
Fig. 2. Scatter diagram of change in cervicogenic headache measured by visual analogue scale (mm) and in energy expenditure of the specific training program at 12-month follow-up. Fitted regression lines are also shown.
| Table III. Determinants of change in chronic headache. |
| Change in chronic headache, VAS | β | SE | p |
| Variable (constant) | 8.600 | 16.264 | 0.598 |
| Headache at baseline (VAS) | –0.630 | 0.060 | < 0.001 |
| Strength group | –1.113 | 3.568 | 0.756 |
| Age, years | –0.020 | 0.306 | 0.949 |
| METh of work | 0.026 | 0.020 | 0.195 |
| Change in METh of LTPA | 0.003 | 0.028 | 0.902 |
| METh of STP | –0.621 | 0.146 | < 0.001 |
| R2 | 0.540 | | |
| SEE | 19.416 | | |
| The variables for the forced regression procedures were headache at baseline ( visual analog scale, VAS), the strength group (comparison with the endurance group), age, energy expenditure of work (METh, metabolic equivalents per hour) and change in the METh of leisure-time physical activity (LTPA), and METh of the specific training program (STP), R2 (regression square) and SEE (standard error of the estimate). |
Discussion
The same reduction was reported in both headache and neck pain as a result of the combined strength training and stretching at the 12-month follow-up. The combined muscle endurance training and stretching resulted in a comparable decrease in headache and neck pain. Upper extremity pain also showed a similar reduction in the 2 training groups. Thus, the study showed that both long-term isometric strength and dynamic endurance training of the neck muscles is an effective treatment not only for chronic neck pain but also for other painful symptoms associated with it. Moreover, the analysis showed that strength training was more effective in relieving neck pain in the subgroup with severe headache. However, both strength and endurance training were also effective in reducing severe headache, as the participants with the highest headache scores at baseline benefited most from the training programme. Although both training modes relieved headache in 100 participants, 20 trainees whose training intensity was 9 METh per week did report any reduction in their headache intensity. Furthermore, all but one of the subjects whose training intensity was 10 METh per week or more reported VAS reduction in headache of more than 35 mm. All the latter trainees were in the SG, exercising 3 times a week. Thus, the results of the training dose analysis for headache were in line with those reported previously for neck pain (25). In the dose-analysis, 1 METh of training per week accounted for a VAS reduction of 0.6 mm in headache. That is, the intensity of specific training was between 5 and 9 METh per week, which, according to the dose analysis, was equal to a 15–22 mm reduction in headache in VAS. Moreover, the intensity of headache does not appear to have a negative effect on the results of training therapy, but rather the contrary. Intensity of headache did not make any statistically discernible difference to the change in neck pain in the EG or CG, which may be due to differences in intervention between the groups. However, normal biological variation cannot be excluded as a reason, as the subgroups were small. Thus further research on the effectiveness of intensive neck exercises for headache is needed.
We found only one randomized controlled study showing exercise therapy to be effective in cases of headache. In the study by Jull et al. (13) patients with cervical headache exercised twice daily for 6 weeks. The exercise programme consisted of isometric craniocervical flexion exercises in the supine position, scapular retraction and holding, isometric rotator and stretching exercises. Patients were trained to sit with a natural lumbar lordosis while retracting the scapulas and elongating the cervical spine regularly throughout the day. At the 12-month follow-up, the neck pain index (Northwick Park Questionnaire) was reduced by 52% in the exercise group and by 21% in the control group. A reduction of 50% or more in headache frequency was achieved by 76% of the exercise group compared with 29% of the control group. The intensity of headache measured by the VAS decreased by 52% in the exercise group and by 25% in the control group. In that study the primary outcomes were related to cervical headache, whereas in the present study the main interest was originally in neck pain and the headache analysis was performed subsequently. The weakness of the present study is that the headaches were not subtyped. However, these studies showed that both moderate- and high-intensity neck muscle exercises may be effective in the treatment of headache associated with cervical pain. Further research is required to evaluate whether specific types of headaches would be ameliorated by exercise more than others.
Barton & Hayes (26) found 50% lower maximal neck flexor muscle strength in patients with unilateral neck pain and headache compared with healthy controls. Other studies have also found neck flexor muscle strength to be significantly inferior in patients with cervical headache compared with controls (27, 28). However, it is probably not the flexor muscles alone that are affected. Ylinen et al. (29) found weakness not only in the flexor but also in the extensor and rotator muscles in patients with chronic neck pain compared with healthy matched controls. Females with chronic neck pain have been found to have smaller cervical multifidus muscles than healthy females (30). Suboccipital muscle atrophy has been found to be associated with chronic tension-type headache (31). However, it is not known whether decreased strength, metabolism and muscle atrophy are the aetiology or result of chronic neck pain. From the perspective of physical function, it appears that passive stretching alone may not always be an effective treatment for chronic neck pain and the symptoms associated with it, while muscle exercise that is intensive enough to improve muscle metabolism and strength, has been shown to be better (32).
Chronic pain is commonly associated with compression hyperalgesia of tissues in the local area (33). A lower pressure pain threshold has been found in cervicogenic headache patients compared with healthy controls and patients with other types of headache (34). Specific exercises involving intensive neck muscle contraction that exceeds the muscular effort used in ordinary daily living have been shown to induce local hypoalgesia both immediately post-exercise (35) and in the long-term (36). An exercise frequency of 3 times a week was also found to have an important impact on the results in our previous study, and thus should be considered when planning training programmes (25).
The initial intervention does not necessarily need to be institutional, as in the present study, as specific neck exercises conducted in the workplace or outpatient clinic have also been shown to alleviate chronic neck pain (37, 38). However, a common problem with home exercises supported by a low frequency of supervised exercise therapy is poor long-term compliance (38, 39). It is also important to bear in mind that while supervised exercise therapy for a couple of months may have an excellent short-term effect, this effect may be lost in the long-term (32). Thus, the emphasis should be on maintaining exercise compliance for not less than one year, as this may prevent the reoccurrence of pain even if the exercise ceases thereafter, as shown in the 3-year follow-up of the present study (40). Exercise compliance can be maintained by issuing reminders about the necessity of exercise. However, psychological support, such as when a consultant expresses interest in a patient’s health, at regular intervals may be even more important.
In conclusion, strength and endurance exercises, when accompanied by stretching exercises, were shown to be an effective treatment for headache and arm pain associated with neck pain. The study showed, in addition, that headache does not have a negative effect on the results of exercise therapy. Thus, headache does not seem to be a hindrance to strength training, which can thus also be recommended for patients experiencing severe headache associated with neck pain.
ACKNOWLEDGEMENTS
This research project was financed by the Social Insurance Institution, Finland. The authors thank Leena Nyrhinen and Tuula Lavonen for the rehabilitation arrangements and Juha Jalovaara for administering the tests.
References