BACKGROUND: Extracorporeal shock wave therapy has been reported to be effective in reducing muscle hypertonia in adults.
Aim: To evaluate the effect of shock wave treatment of spastic muscles in children with cerebral palsy.
METHODS: Twelve children with spastic equinus foot (6 boys, 6 girls; mean age 8 years (standard deviation (SD) 2.31)) were monitored. Clinical (Ashworth Scale, passive range of motion) and instrumental (pedobarography) examination were performed. This is an open study with one placebo treatment session, followed 6 weeks later by one active shock wave treatment session. Gastrocnemius muscles and soleus muscles were treated.
RESULTS: After placebo stimulation no clinical or instrumental effect was seen. After a single active shock wave stimulation a significant decrease in the Ashworth Scale (from 3 to 2), an increase in the range of motion (from 20° to 50°), and an increase in the whole plantar surface area of the treated limb (from 40.3 to 80.2 cm2) were observed in all patients. This effect lasted for 4 weeks in all patients.
CONCLUSIONS: A single active shock wave stimulation produced a significant long-lasting reduction in hypertonia in the plantar flexors in children with cerebral palsy.
Key words: cerebral palsy; spasticity; equinus foot; extracorporeal shock wave therapy.
J Rehabil Med 2010; 42: 339–343
Correspondence address: Paolo Manganotti, Dipartimento di Scienze Neurologiche e della Visione, Sezione di Neurologia Riabilitativa, Univerisity of Verona, Policlinico GB Rossi, Piazzale Scuro, 10, IT-37134 Verona, Italy. E-mail: paolo.manganotti@univr.it
Submitted January 24, 2009; accepted December 3, 2009
INTRODUCTION
Cerebral palsy (CP) is a non-progressive permanent neurological disorder caused by a defect or lesion in the immature brain. It affects motor and postural development and causes sensory disorders and learning disability. Spastic equinus foot is the most common leg deformity in children with CP who are able to ambulate (1). Many studies have demonstrated the effectiveness of botulinum toxin A (BTX-A) as a neuromuscular blockade in the treatment of equinus foot deformities in patients with diplegia and hemiplegia (2–6). Several open-label studies have supported the effectiveness of BTX-A treatment for pes equinus in CP and have shown a significant change in local parameters, such as goniometry, grading of spasticity and complex electrophysiological and biomechanical measures of gait analysis (7–13). However, in a small number of patients, the development of fibrosis and changes in rheological properties of the muscles can reduce the efficacy of treatment. In addition the dosage of BTX-A may not be sufficient to treat extensive and severe hypertonia in the upper and lower limbs in CP. Rehabilitation and different non-invasive treatments, particularly of the connective components, should also be considered. Shock waves are defined as a sequence of single sonic pulses characterized by high peak pressure (100 MPa), fast pressure rise (< 10 ns) and short duration (10 µs). Different studies and clinical experiments have demonstrated the efficacy of shock waves in the treatment of bone and tendon diseases, including pseudoarthrosis (14–16), tendinitis calcarea of the shoulder (17, 18), epicondylitis (19), plantar fasciitis (20), and several tendon diseases, especially in athletes (20, 21). In a previous study we described a long-lasting reduction in hypertonia after shock wave therapy in patients with stroke in comparison with placebo (22), and we suggested a possible use of shock wave treatment for patients with muscular hypertonia due to lesions of the central nervous system.
The aim of this study was to investigate, in a placebo-controlled open study, the effects of a single shock wave stimulation in plantar flexor muscles for a hypothetical treatment of spastic equinus foot in a group of children with CP.
MATERIAL AND METHODS
Participants
Twelve children (6 boys, 6 girls) with CP were evaluated. All children exhibited signs of unilateral spastic equinus. The mean age at the time of treatment was 8 years (standard deviation (SD) 2.31), age range 6–11 years. Outpatients were recruited from different multidisciplinary clinics for treatment of children with CP, using the following inclusion criteria: ability to ambulate (assisted or unassisted), spastic hemiparesis, spastic equinus, no previous treatment with BTX-A in 7 children, no recent treatment with BTX-A in 5 children (the last treatment in all these patients was at least 9 months), and no previous surgery of the foot, ankle, and/or leg. No physiotherapy treatment was performed after shock wave therapy.
The study was approved by the ethics committee of the Department of Neurological Sciences. Informed consent was obtained from the children’s parents before commencing the study.
Evaluation protocol
At each visit comprehensive clinical (range of motion (ROM), Modified Ashworth Scale (MAS)) and instrumental (pedobarography) examination were performed.
Clinical examination. Clinical examination included a single passive range of motion (pROM) evaluation of the ankle of the affected side by an electronic goniometer, and grade of spasticity (MAS) of the plantar flexor muscles. Children were examined by the same physician, who was not blinded. One visit was performed on each occasion by the same physician. The examination was performed with the patient lying on the bed. Video-poligraphy was performed, using on accelerometer (13, 23).
Pedobarometric assessment. The pedobarometric equipment comprised a force plate (FAS system 1.0 ACP Light, Buratto Advanced Technology, Treviso, Italy), with an active surface (47.5 × 43.0 cm) equipped with 2544 optical sensors distributed along the perimetrical border. The pedobarometric static test was performed with patients in the standing position, with arms hanging down, looking at a fixed point, for a period of 14 s. Quantitative analysis of pedobarometric evaluation included the entire plantar surface area (expressed in cm2), the peak pressure values at the forefoot and hind foot (expressed in kPa) (13, 23). No gait analysis was performed. No gross motor function scale was measured.
Study procedure
This was an open study in which each child served as their own control. The protocol consisted of one placebo treatment session in which no shock waves were applied, followed 6 weeks later by one active shock wave treatment session. This was done to ensure homogeneity in both active and placebo groups so that the true effect of shock waves could be compared in each patient. To avoid any possible crossover effect, the study included a 2-week interval between the monitoring of “placebo treatment” and active shock wave therapy.
In each subject, the clinical measurements were performed before and immediately after placebo. Two weeks later identical clinical measures were performed before and immediately after treatment, and 1, 4 and 12 weeks after the active shock wave treatment.
Shock wave instrumentation and treatment
An electromagnetic coil lithotriptor (Modulith SLK®, Storz Medical AG, Tagerwillen, Switzerland) provided with in-line ultrasound, radiographic and computerized aiming (Lithotrack® system, Storz Medical AG) was used. The pressure pulses were focused in the hypertonic muscles of the lower limb: 1500 shots were used to treat each gastrocnemius muscles and soleus muscles mainly in the middle of the belly using an ultrasound pointer-guide. The energy applied was 0.030 mJ/ mm2. The therapy is painless and does not require any kind of anaesthesia or the use of analgesic drugs. A placebo treatment without shock wave energy was applied with the identical instrumentation, with the pointer over the muscle. The same high-intensity sound was utilized in all patients.
Statistical analysis
A descriptive statistical study of the quantitative parameters of mean and SD was performed. Clinical and electrophysiological and instrumental values for each patient were submitted to analyses of variance (ANOVAs) with repeated measures. Post-hoc comparisons were performed with paired t-tests adjusted with the Bonferroni method. The alpha level chosen for all analyses was 0.05.
RESULTS
Placebo stimulation
No significant changes in Ashworth Scale in the plantar flexor muscles (gastrocnemius muscles and soleus), pROM and different parameters of pedobarometric evaluation (surface area, peak pressure value) were noted after placebo stimulation (Table I).
| Table I. Clinical and electrophysiological findings after extra-corporeal shock wave therapy (ESWT) |
| Variables | Baseline Mean (SD) | Immediately after placebo Mean (SD) | Immediately after ESWT Mean (SD) | After 1 week Mean (SD) | After 4 weeks Mean (SD) | After 12 weeks Mean (SD) | p-value Mean (SD) |
| Ashworth plantar flexors | 3.3 (0.49) | 3.1 (0.38) | 1.8 (0.38)* | 1.9 (0.51)* | 2.25 (0.45)* | 2.8 (0.57) | < 0.001 |
| pROM(°) | 20 (7) | 20 (6) | 50 (6)* | 50 (7)* | 40 (6)* | 30 (8) | < 0.001 |
| Plantar surface area (cm2) | 40.31 (5) | 43.15 (6) | 80.23 (7)* | 70.12 (5)* | 68.09 (8)* | 48.23 (6) | < 0.001 |
| peak pressure value (kpa) | 20.5 (4) | 22.1 (6) | 99.57 (9)* | 95.06 (6)* | 70.11 (8)* | 30.4 (9) | < 0.001 |
| *p < 0.001 with Bonferroni correction. pROM: passive range of motion. |
Active stimulation
The mean baseline evaluation Ashworth Scale results for the treated plantar flexor was 3.3 (SD 0.49). Immediately after the active treatment, the Ashworth Scales for the plantar flexor decreased to 1.8 (SD 0.38) (p < 0.001).
Persistent effects were observed in all children (Table I). As regards the Ashworth Scale results, the time effect was statistically significant (F (4, 11) = 80.603, p < 0.001). Post-hoc comparisons showed a significant difference in muscle tone of all plantar flexors between baseline and after one week (p < 0.001), and between baseline and after 4 weeks (p < 0.02).
There were no statistically significant group differences between baseline and muscle tone of the plantar flexors after 12 weeks, even though in 5 children the effects persisted at this time. No difference effects of shock wave treatment were noted between children with different degree of hypertonia, as measured by the Ashworth Scale.
pROM
As regards the pROM of the treated limb of all patients, the time effect was statistically significant (F (4, 11) = 80.632, p < 0.001).
Post-hoc comparisons showed a significant difference in pROM between baseline and immediately after treatment (20° vs 50° respectively; p < 0.01) between baseline and the first week after treatment (20° vs 50° respectively; p < 0.01), between baseline and 4 weeks after treatment (20° vs 40° respectively; p < 0.05). There were no statistically group differences in passive motion of the ankle between baseline and 12 weeks after treatment (Table I).
Pedobarometric evaluation
As regards the pedobarometric measures, the time effect was statistically significant (F (4, 11) = 78.127, p < 0.001). In the post-hoc comparisons the significant findings were:
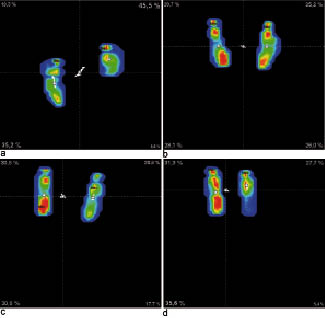
• An increase in the whole plantar surface area (cm2) on the treated limb between baseline and immediately after treatment (40.3 vs 80.2) (p < 0.01), between baseline and the first week after treatment (40.3 vs 70.1; p < 0.05), between baseline and 4 weeks after treatment (40.3 vs 68.1; p < 0.05) (Table I, Fig. 1). No statistically group differences were found between baseline and 12 weeks after treatment.
Fig. 1. Pedobarometric findings for one child (raw data). (a) Before treatment, (b) immediately after treatment, (c) 1 week, and (d) 4 weeks after treatment.
• A significant increase in the peak pressure value (kPa) on the hindfoot of the treated side between baseline and immediately after treatment (20.6 vs 99.6 p < 0.01); between baseline and the first week after treatment (20.6 vs 95.1; p < 0.01), between baseline and 4 weeks after treatment (20.6 vs 70.1; p < 0.05) (Table I, Fig. 1). No statistically significant group differences were found between baseline and 12 weeks after treatment.
DISCUSSION
The main finding of this study was that a single active treatment of shock wave therapy of the spastic muscles of the lower limbs in children with CP produced a significant reduction in muscle tone. No effect was noted after placebo stimulation. The effect of active stimulation was long-lasting after the therapy. No side-effects were observed in any patient. The main limitation of the study is that the protocol was not blinded; however, the clinical findings were consistent across the patients and comparison with placebo was performed in all of the children.
Clinical data (Ashworth Scale and pROM evaluation) support the effectiveness of active treatment with shock wave therapy of spasticity in the plantar flexor muscles in the lower limb in CP. These data are in agreement with our previous study of spastic upper limbs in adult patients with stroke (22), which documents that non-invasive shock wave therapy produced a relative long-lasting decrease in spastic hypertonia in hand muscles.
Instrumental findings showed that shock wave treatment decrease in hypertonia in foot flexor muscles on the treated limb can change the postural attitude and body stability of children with CP. Reducing the hypertonia of the plantar flexor muscles, we observed an increase in the whole plantar surface area on the affected side. Similarly, children showed a significant increase in peak pressure values at the hind foot on the affected side. This effect is similar to that produced by BTX-A injected into the plantar flexor muscles, as measured with the same methods in our previous study (13, 23). The effect of extra-corporeal shock wave therapy on children is relatively long-lasting, after only one session, the effects last for some weeks.
The mechanism of shock wave therapy on spastic muscles is unknown. Few studies have investigated the mechanisms of the shock waves, which can induce non-enzymatic (24) and enzymatic nitric oxide (NO) synthesis (25–27). NO is involved in neuromuscular junction formation in the peripheral nervous system (28) and in important physiological functions of the CNS, including neurotransmission, memory and synaptic plasticity (29). NO synthesis has been suggested as an important mechanism to explain the effectiveness of shock waves in the anti-inflammatory treatment of different tendon diseases (25–27). However, the reduction in hypertonia in patients after stroke after shock wave therapy is not produced by denervation or lesion of the peripheral nerve, as shown by neurophysiological findings in a previous study (22).
A direct effect of shock waves on fibrosis and on the rheological properties of the chronic hypertonic muscles in CP should be considered together with the documented therapeutic effect on bone and tendon diseases (14–20).
In addition, we might consider possible tixotrophy effects of shock waves on tissues and vessels of the treated muscles (25, 26). The effect of mechanical stimuli of shock waves on the muscle fibres next to the tendon cannot be excluded (30). Continuous or intermittent tendon pressure can decrease the spinal excitability without long-lasting clinical. Nevertheless, in these 12 children group the clinical effects lasted for weeks, excluding a major effect of mechanical vibratory stimulation, which is transitory and short lasting (e.g. some hours).
In conclusion, shock wave therapy appears to be safe, non-invasive, not painful and without complications. These preliminary findings suggest that shock wave therapy may be useful in decreasing flexor tone in children with spasticity of the lower limbs. This therapy could open a new field of research into the non-invasive treatment of spasticity in children. Further studies, with repetitive treatment and with a larger group of patients with CP, are therefore necessary.
ACKNOWLEDGMENTS
The authors thank Dr C. Guerra for support and clinical suggestions and Ernst Marlinghaus for technical suggestions.
Conflict of interest: The authors declaire no conflicts of interest.
REFERENCES