OBJECTIVE: To clarify the relationship between malnutrition and dysphagia following stroke.
DESIGN: Systematic review.
METHODS: All published trials that had examined both the swallowing ability and nutritional status of subjects following stroke were identified. Pooled analyses were performed to establish whether the odds of being malnourished were increased given the presence of dysphagia.
RESULTS: Eight studies were identified. The presence of malnutrition and dysphagia ranged from 8.2% to 49.0% and 24.3% to 52.6%, respectively. Five of the included trials were conducted within the first 7 days following stroke, while 3 were conducted during the rehabilitation phase. The overall odds of being malnourished were higher among subjects who were dysphagic compared with subjects with intact swallowing (odds ratio: 2.425; 95% confidence interval: 1.264–4.649, p < 0.008). In subgroup analysis, the odds of malnutrition were significantly increased during the rehabilitation stage (odds ratio: 2.445; 95% confidence interval: 1.009–5.925, p < 0.048), but not during the first 7 days of hospital admission (odds ratio: 2.401; 95% confidence interval: 0.918–6.277, p < 0.074).
CONCLUSION: In a systematic review including the results from 8 studies, the odds of being malnourished were increased given the presence of dysphagia following stroke.
Key words: protein-energy malnutrition, nutritional assessment, stroke, deglutition disorders.
J Rehabil Med 2009; 41: 707–713
Correspondence address: Norine Foley, Aging, Rehabilitation & Geriatric Care Program Lawson Health Research Institute, Parkwood Hospital, Rm B-3019b, 801 Commissioner’s Rd, E. London, ON, N6C 5J1 Canada. E-mail: norine.foley@sjhc.london.on.ca
Submitted April 06, 2009; accepted June 09, 2009
INTRODUCTION
High prevalences of both malnutrition (1–3) and dysphagia (4–6) have been reported following stroke. Although it is generally well-established that these conditions frequently co-exist and are associated with poor outcomes following stroke (7), the nature of the relationship between them remains poorly understood. Following stroke, malnutrition may develop as a consequence of dysphagia if nutritional intake is substantially reduced in relation to requirements over the course of days or weeks. In this regard, stroke may be seen as a precipitating event and malnutrition as the outcome; however, it is difficult to suggest a mechanism that explains the co-existence of dysphagia and malnutrition acutely, following stroke.
Although explored in several studies as a secondary objective, only one trial has been conducted with the primary objective of examining the relationship between malnutrition and dysphagia during the acute post-stroke period (8). In this trial no significant relationship was found, although a positive correlation between dysphagia and stroke severity was demonstrated. This finding suggests that previous accounts of an association may have been confounded by the presence of other factors. The relationship between dysphagia and malnutrition also has been explored in the subacute phase or rehabilitation phase (several weeks after stroke onset) with conflicting results (1, 9, 10). The purpose of this review was therefore to survey the published literature with the aim of clarifying the relationship between nutritional status and dysphagia in both the acute and rehabilitation stages following stroke.
METHODS
Relevant studies were identified through a literature search encompassing the years 1985 to October 2008. The following databases were searched: the Cumulative Index to Nursing and Allied Health Literature (CINAHL), MEDLINE, EMBASE and ISI Web of Science. Search terms varied slightly across databases, but included: “cerebrovascular accident” or “stroke”, and the terms “nutrition” or “diet” or “malnutrition” or “nutrition assessment” and “dysphagia” or “deglutition disorders” as MeSH terms, key words or subject headings. The search was limited to: “Human”, “All adults; 19+ years”. Hand searching of the bibliographies of the included studies was conducted to identify potential articles not recovered using the search terms. Articles from a recent systematic review examining nutritional status following stroke were also used if dysphagia had been reported (11).
Studies were included if: (i) well-nourished subjects were identified and differentiated from those who were malnourished on at least one occasion during the hospitalization period following a first or recurrent stroke, and (ii) subjects with intact swallowing were differentiated from those who had swallowing impairment. We accepted the authors’ definitions and assessments of both malnutrition and dysphagia. Studies were excluded if the study sample included a proportion of patients who had not sustained a stroke or if 100% of subjects were either dysphagic or had intact swallowing. This final criterion was included to enable an examination of associations between dysphagia and malnutrition within each trial. Abstracts, conference proceedings and letters to the editor were excluded because of lack of reporting detail.
The following data were collected from each included study: (i) patient characteristics; (ii) the percentage of subjects with swallowing impairment; (iii) the percentage of patients identified as malnourished; and (iv) the timing and method used for nutritional and swallowing assessments. We confined the reporting of abstracted results to those that facilitated an examination of the relationship between dysphagia and malnutrition. Associations between the dichotomized variables of nutritional state (well-nourished vs malnourished) and swallowing ability (impaired vs intact swallowing) were examined using the χ2 statistic when data were available in the original reports. Pooled analyses were also conducted using the software Comprehensive Meta-analysis (version 2, Biostat Inc., Englewood, New Jersey, USA, 2007). The odds ratio (OR) and 95% confidence interval (CI) of malnutrition given the presence of dysphagia are reported. A random effects model was chosen to account for both within- and between-study variability. The effect of timing of stroke onset (acute vs rehabilitation) was examined as a covariate using subgroup analysis.
RESULTS
Literature reviewed
The results of the literature search are presented in Table I. The initial search strategy returned 534 results. On the basis of the title or abstract 522 studies were excluded. The remaining 12 articles, which suggested that both nutritional state and swallowing status had been established on at least one occasion following stroke, were examined. Of these, 8 were excluded for the following reasons: well-nourished subjects had not been differentiated from malnourished subjects (12–14), subjects with diagnoses other than stroke were included (15), swallowing or nutritional status of subjects was not recorded (2, 16), or publication duplication (reporting on the same cohort of subjects) (17). Finally, the Food or Ordinary Diet (FOOD) trial was excluded since all subjects were either dysphagic or fed enterally, or had intact swallowing and received oral sip supplementation (18). However, the preliminary findings from this trial, which did examine the association between nutritional status and swallowing ability, were retrieved through manual searching (19). Three trials identified from a previous review examining the nutritional status of subjects post-stroke also reported on the prevalence of dysphagia and were included (9, 20, 21). A total of 8 studies remained for review (1, 8–10, 19–22).
| Table I. Literature search outcome |
| | MEDLINE | EMBASE | ISI Web of Science | CINAHL | Total |
| Hits on database | 174 | 163 | 108 | 89 | 534 |
| Exclusions: | | | | | |
| Duplication between database | – | 55 | 54 | 43 | 152 |
| Non-English | 19 | 27 | 3 | 1 | 50 |
| Review | 30 | 25 | 9 | 11 | 75 |
| Commentary/Letter to editor/Case report | 38 | 19 | 3 | 24 | 84 |
| All subjects dysphagic | 23 | 4 | 4 | 5 | 36 |
| No nutrition assessment conducted | 33 | 17 | 9 | 3 | 62 |
| Subjects with diagnoses other than stroke recruited | 11 | 8 | 20 | 2 | 41 |
| Non-patient | 8 | 3 | 2 | 0 | 13 |
| Other | 3 | 4 | 2 | 0 | 9 |
| Total exclusions | 165 | 162 | 106 | 89 | 522 |
| Trials remaining following review of title/abstract | 9 | 1 | 2 | 0 | 12 |
Study and patient characteristics
The average age of patients ranged from 57 (9) to 79 (21) years. In a single study, inclusion was restricted to subjects with ischemic stroke (8), while subjects in the remaining trials had had either ischemic or hemorrhagic stroke, except in one case where no details of stroke etiology, type or location were provided (10), In all but 2 trials, which did not report details, subjects with previous stroke were included (10, 22). The eligibility criteria of one trial excluded subjects with pre-morbid swallowing impairment due to stroke or other causes (8). Although not explicitly stated, dysphagia was assumed to be a consequence of stroke in all other trials. The majority of trials conducted during the acute hospital admission period included subjects who experienced a broad range of stroke severity, from mild to severe. Subjects included in 3 trials conducted during the rehabilitation admission or in an infirmary appeared to have experienced moderately disabling (1, 9) and more severe strokes (10), respectively.
Nutritional assessments
The nutritional assessment techniques used in the studies are described in Table II. None of the studies used the same assessment method. The percentage of patients identified as malnourished at study entry, based on the authors’ criteria, ranged from 8.2% (10) to 49% (1). A traditional approach to nutritional assessment, which included a combination of anthropometric and biochemical measurements, was used in 3 trials (1, 10, 20), while either a low body mass index (BMI) or a history of weight loss was sufficient to detect malnutrition in one trial (9). The FOOD Trial Collaborators permitted clinicians at each of the 125 participating centres to classify a patient’s nutritional status based on their own standard of care. In this trial an informal assessment, which estimates a subject’s weight following brief observation, was used as the sole marker of nutritional state in the absence of a more comprehensive assessment. This method was used to categorize 60% of the subjects as underweight, normal weight or overweight (19). Clinical judgement using either a modified version of Subjective Global Assessment (SGA), or a variant, Patient-Generated SGA (PG-SGA), was used in 2 trials (21, 22). SGA was designed originally for use in the prediction of risk for complications following general surgery, although its use has become more widespread in recent years. This assessment technique involves obtaining a nutrition-oriented history, focusing on declines in usual intake or weight over the preceding 6 months, identifying the presence of gastrointestinal symptoms and nutrition-related functional impairment, plus a physical examination that focuses on muscle wasting and subcutaneous fat loss. The final trial (8) used the Mini Nutritional Assessment (MNA), a method that includes anthropometric measurements, global assessment, a dietary questionnaire and subjective assessment. This form of nutritional assessment was developed as a screening and assessment tool to identify geriatric patients at risk of malnutrition. Two of the methods described above, MNA and an informal assessment, have been validated previously (23–25).
Swallowing assessments
The methods used to establish the presence of dysphagia are presented in Table II. The prevalence of dysphagia at entry into the study ranged from 24.3% (19) to 52.6% (8). In 3 studies dysphagia was identified retrospectively through chart review (1, 10, 22). In the remaining studies swallowing ability was assessed using a water-swallowing test (20) or was inferred given a subject’s inability to swallow (19). Oral mechanism observations/assessments of eating performed during a meal or test meal were employed to identify swallowing difficulties in 2 trials (9, 21). In one trial, the Mann Assessment of Swallowing Ability (MASA) was used (8). The MASA is a brief, 26-item, bedside examination designed to assess swallowing ability. The tool includes components that evaluate oromotor/sensory components of swallowing, baseline cranial nerve function and functional assessment of swallowing. Scores of 178 to a maximum of 200 points indicate no swallowing abnormality, while scores below this indicate mild < 168–177), moderate (< 139–167) and severe (< 138) impairment. Only one assessment method, the MASA tool, has been validated previously. When compared with the reference standard of videofluoroscopy, the sensitivity and specificity of the examination were 71% and 72%, respectively, using a MASA cut-off score of < 180 (26).
| Table II. Results (arranged chronologically) |
| Study/subject inclusions | Timing/methods used for screening or assessment of dysphagia/prevalence of dysphagia | Timing/methods used for screening or assessment of nutritional status/prevalence of malnutrition | Association(s) between dysphagia and malnutrition |
| Finestone et al. 1995 (1) n = 49 (32 M/17 F) subjects admitted consecutively to a stroke rehabilitation unit Mean age: 61 years | Assessments were conducted during subjects’ stay on the acute service using clinical or a videofluoroscopic modified barium swallow Subjects were admitted to rehabilitation a mean of 22 days post-stroke Clinical: evidence of choking, coughing, wet-sounding voice after food consumption, decreased oral motor function or difficulty swallowing Dysphagia: 47% on admission to rehabilitation unit | Assessment conducted within 4 days of admission to rehabilitation Serum albumin (< 35 g/l), transferrin (< 2.0 g/l), total lymphocyte count (< 1800 mm3), body weight (< 90% of reference weight, or < 95% of usual weight, or body mass index< 20), sum of 4 skinfolds (< 5th percentile of reference population), mid-arm muscle circumference (< 5th percentile of reference population). Criteria: ≥ 2/6 nutrition variables below reference limits Malnutrition: 49% on admission to rehab unit | On admission to the rehabilitation unit, a greater proportion of subjects who were malnourished were dysphagic compared with those who were well-nourished (15/24 vs 8/25, p = 0.032) |
| Davalos et al. 1996 (20) n = 104 (60 M/44 F) (n = 91 at 1-week) admitted to hospital with an acute stroke within 24 h of symptom onset. < 80 years without subarachnoid hemorrhage Mean age: 66 years | First assessment within 24 h of admission Alert subjects: unable to swallow 10 ml water. All unconscious subjects were classified as dysphagic Dysphagia: 30% | Initial assessment conducted within 24 h of admission. Serum albumin (< 35 g/l) or tricep skinfold or mid-arm muscle circumference < 10th percentile of reference population. Malnutrition: 16.3% at hospital admission (n = 104), 26.4% after 1 week (n = 91) | At admission there was no association between nutritional state and dysphagia Subjects with dysphagia at admission were more likely to be malnourished at 1 week post-stroke compared with subjects who were well-nourished (16/24 vs 15/67, p < 0.001) |
| Westergren et al. 2001 (21) n = 162 (74 M/88 F) subjects admitted consecutively to a stroke rehabilitation unit Mean age: 79 years | Timing of assessment not stated, but presumed to be at admission, a median of 6 days following stroke. Structured observation/assessments of eating were performed following admission to the stroke rehabilitation unit. Subjects identified with swallowing difficulties were considered to be dysphagic Dysphagia: 25% | Initial assessment conducted at admission to rehabilitation Author’s modified version of Subjective Global Assessment (SGA) A = well nourished B = well nourished but at risk of becoming malnourished C = suspected of being malnourished D = severely malnourished Criteria: SGA classes B or C or D = malnourished 32% at admission to rehabilitation | Swallowing difficulty was found to be a predictor of nutritional status (odds ratio: 4.6, 95% confidence interval: 1.6–13.2, p < 0.006). |
| FOOD 2003 (19) n = 3012 (1520 M/1492 F) subjects admitted to a participating hospital within 7 days of acute stroke. Any subject presenting with a recurrent or first-ever stroke was eligible to participate Mean age: 73.3 years | Single assessment conducted following admission to hospital Subjects who were not able to swallow were considered to be dysphagic. Dysphagia: 24.3% | Single assessment conducted following admission to hospital Clinical judgement was used to determine if a patient was undernourished, normal or overweight. (A more comprehensive assessment may also have been carried out) Malnutrition: 9.3% | No association between nutritional state and dysphagia. |
| Martineau et al. 2005 (22) n = 73 (44M/29 F) admitted to an acute stroke unit with a length of stay > 48 h who received a nutritional assessment Mean age: 72 years | Presence of dysphagia was obtained retrospectively from chart review. Appears swallowing status was assessed shortly after acute admission. Dysphagia: 40% | Single assessment within 48 h of admission Patient Generated SGA (PG-SGA) A = well nourished B = moderately (or suspected of being malnourished C = severely malnourished Criteria: B or C = malnourished Malnutrition: 19.2% | A greater proportion of subjects who were malnourished were dysphagic compared with those who were well-nourished (10/14 vs 19/59, p = 0.007) |
| Table II. Results (arranged chronologically) |
| Study/subject inclusions | Timing/methods used for screening or assessment of dysphagia/prevalence of dysphagia | Timing/methods used for screening or assessment of nutritional status/prevalence of malnutrition | Association(s) between dysphagia and malnutrition |
| Crary et al. 2006 (8) n = 76 (36 M/40 F) admitted to stroke unit without pre-stroke dysphagia or conditions that would impact swallowing ability Mean age: 66 years | Single assessment completed a mean of 2.2 days following admission for acute stroke A score of < 178 on the Mann Assessment of Swallowing Ability indicated dysphagia Dysphagia: 52.6% | Single assessment completed a mean of 2.2 days following admission for acute stroke Mini Nutritional Assessment (maximum score = 30) Criteria: score < 23.5 Malnutrition: 26.3% | No association between malnutrition and dysphagia. Correlation co-efficient –0.029 p = not significant |
| Poels et al. 2006 (9) n = 69 (47 M/21 F) (60 at 4 weeks) Subjects without aphasia > 18 years admitted to rehabilitation unit. Mean age: 57 years | Assessment conducted according to Westergren et al. 2001 (21) Mean interval between stroke and screening was 34 days following stroke, following admission to stroke rehabilitation Dysphagia: 43% | Initial assessment conducted 34 days following stroke at admission to rehabilitation service Unintentional weight loss of more than 5% in 1 month or 10% in 6 months or body mass index < 18 for subjects < 65 years or < 22 for subjects ≥ 65years indicated malnutrition Malnutrition: 35% at admission to rehabilitation | No association between malnutrition and dysphagia 4/20 subjects with swallowing difficulties/malnourished vs 4/40 subjects with difficulties swallowing/well-nourished (p = 0.233) |
| Chai et al. 2008 (10) n = 61 (33 M/28 F) admitted to infirmary with significant disability following stroke Mean age: 76 years | Interval between stroke onset and assessment not reported, but appears to have been shortly after arrival to infirmary. Presence of dysphagia was determined through retrospective chart review. Dysphagia was established prior to admission or at the time of assessment by speech-language pathologis if: patient observed to be choking during a meal, patient complained of swallowing difficulty or repeated chest infection. Dysphagia: 34.4% | Time of assessment not reported, but appears to have been shortly after arrival to infirmary. Nutritional status retrieved through chart review. body mass index < 18.5 and serum albumin < 35 g/l Malnutrition: 8.2% | A greater proportion of subjects who were malnourished were dysphagic compared with those who were well-nourished (4/5 vs 17/56, p = 0.044) |
Associations between swallowing ability and nutritional state
Six studies reported sufficient data to enable calculation of associations (1, 9, 10, 19, 20, 22). Although 2 trials reported the percentages of subjects who were malnourished and who were dysphagic, the proportion of malnourished subjects who were also dysphagic was not reported (8, 21). The authors of these trials were contacted and one (Crary et al., 8) provided the requested data. Among these 7 studies, 3 reported that a greater proportion of subjects with dysphagia were malnourished compared with subjects who were well-nourished (1, 10, 22). Three studies reported no association (8, 9, 19). In the final trial, in which the association was examined on 2 occasions, the results conflicted (20).
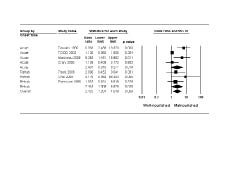
Using data from 7 studies, the overall odds of being malnourished were higher among subjects who were dysphagic compared with subjects with intact swallowing (OR: 2.425; 95% CI: 1.264–4.649, p < 0.008). In subgroup analysis, the odds of malnutrition were significantly increased during the rehabilitation stage (OR: 2.445; 95% CI: 1.009–5.925, p < 0.048), but not during the first 7 days of hospital admission (acute period) (OR: 2.401; 95% CI: 0.918–6.277, p < 0.074) (Fig. 1).
Fig. 1. Pooled analysis of the association between dysphagia and malnutrition following stroke. CI: confidence interval.
DISCUSSION
Of the 8 trials included in this study, the relationship between dysphagia and malnutrition was examined on 9 occasions. The results were ambiguous. Significant associations were reported, on 5 occasions. Using pooled analyses, there was an increase in the odds of malnutrition given the presence of dysphagia, although the effect was statistically significant only when trials that had been conducted several weeks following stroke onset were included. Several factors, such as timing and method of swallowing and nutritional assessments that were used and the modifying effects of other variables may help us to better understand the nature of this relationship.
Dysphagia may contribute to the development of malnutrition following stroke. For those able to eat orally, fear of eating and/or choking, unwillingness to eat and the decreased palatability of texture-modified diets may lead directly to inadequate intake; however, other factors that often accompany dysphagia may also impact indirectly on an individual’s desire or ability to eat. Depending on the location of stroke, fatigue, motor impairment, visuospatial perceptual, depression, and cognitive deficits may be contributory. In 3 of the studies included in the present review, patients were admitted to a rehabilitation facility or infirmary following a delay of at least 3 weeks; theoretically a sufficient length of time for a patient to change from a well-nourished state to a malnourished one. Although an association between malnutrition and dysphagia was reported in 2 of these trials (1, 10), the contributory role dysphagia might have played in the development of malnutrition remains unclear for several reasons. It is unknown whether a proportion of patients was already malnourished at the time of stroke onset, or if there was further deterioration during the acute hospitalization period attributable to other causes. The adequacy of nutritional intake and the degree or severity of dysphagia was not reported in any of the studies.
There are limited and conflicting reports of the adequacy of energy and protein intakes of patients consuming texture-modified dysphagia diets during hospitalization (27, 28). Of the 2 studies found on the subject, only one was stroke-specific (28). The results of this trial indicated that the previously well-nourished patients received an average of 80–90% of their protein and energy requirements regardless of diet type (regular vs texture-modified) over the immediate 3-week period following stroke. It also appears that stroke, unlike conditions such as traumatic brain injury, does not increase caloric demands significantly (29, 30). Hypermetabolism, if present, would represent an additional challenge to meeting nutritional requirements. There is also evidence that other impairments may be greater contributors to the development of malnutrition. Following severe stroke, Axelsson et al. (31) reported a worsening of nutritional indices in patients with dysphagia, while also noting that right-arm motor deficits and dependency in self-care were better predictors of undernutrition 3 weeks post-stroke than eating problems. While it has been demonstrated previously that subjects with neurogenic dysphagia have exhibited “dysphagia-induced starvation”, as evidenced by significant weight loss (32), the use of non-oral feeding strategies, such as enteric feeding tubes, has become more commonplace in recent years as a means for patients unsafe with oral intake to achieve their nutritional requirements. Current clinical practice guidelines commonly recommend the use of such strategies (33).
In 5 of the included studies both swallowing and nutritional assessments were conducted concurrently within 7 days following stroke. In these trials, since dysphagia did not precede malnutrition, it could not have been a contributor to its development, and the nature of a positive association identified in 3 of these trials is more difficult to explain. While Veldee & Perth (34) have proposed a mechanism through which malnutrition could lead to the development of dysphagia through the atrophy of deglutitive muscles, stroke was assumed to be the primary cause of dysphagia in this study. We suggest that in the positive studies the relationship was not causal, and stroke severity may have acted as a confounding variable. While stroke size and location are the greatest determinants of swallowing function, it is also true that the presence of dysphagia is itself an indicator of greater stroke severity (35, 36). Increasing stroke severity may also influence the identification of malnutrition, due to the limitations of many of the biochemical measurements commonly used for nutritional assessment. The hepatic production of many proteins, including albumin, pre-albumin and transferring, are down-regulated during periods of acute illness, resulting in depressed serum values (37, 38). These declines, indicative of a worsening nutritional state, may occur independently of true nutritional status. An association between malnutrition and dysphagia was reported in all of the 3 trials that used a form of nutrition assessment that included hepatically-synthesized proteins (1, 10, 20).
The contributing effect of stroke severity was assessed in only 2 of the included trials (8, 20). In one of the included trials, associations between malnutrition at one week and both dysphagia and stroke severity at admission were reported (20). Even though the inflammatory process can enhance nutritional depletion, there was evidence that one of the components used for nutritional assessment, serum albumin, was depressed due to non-nutritional factors. Despite receiving their full energy and protein requirements either enterally or orally, the number of subjects with hypoalbuminemia (< 35 g/l) increased over the 1-week period. Furthermore, in this trial an association between malnutrition and stroke severity, assessed using the Canadian Stroke Scale and the Barthel Index (BI), was reported. In addition to higher mortality at one week, death and poor outcome (dead or BI ≤ 50 at one month) were observed more frequently in patients identified as malnourished. Together, these findings suggest that patients with more severe strokes were identified as malnourished. Crary et al. (8) also reported that dysphagia was associated with stroke severity, as assessed using the National Institutes of Health Stroke Scale, but not malnutrition in a study that was designed specifically to assess the dysphagia/malnutrition relationship. This was the only trial that used previously validated assessment tools to assess both nutritional status and swallowing ability. Another possible explanation for the lack of association may have been the means by which these authors elected to identify cases of malnutrition, since subjects identified as being “at risk” (MNA score 17–23.5) were also included in the malnourished category.
Since the pre-stroke nutritional status of patients in any of the studies reviewed was unknown, it remains unclear whether malnutrition was pre-existing at the time of the initial assessment, or if it developed as a consequence of stroke. However, the authors of 5 of the included studies used nutritional assessment methods that captured remote nutritional status, using static measures, such as weight or weight loss, and did not include biochemical measurements (8, 9, 19, 21, 22). In these trials it could be assumed that nutritional state assessed shortly after stroke onset was the equivalent of pre-stroke nutritional state. The validity of the assessment methods may also have been influential. Among the 8 trials included, 2 used previously validated nutritional assessment tools (8, 19) and only one used a valid assessment of swallowing status (8). In both of these trials no associations between malnutrition and dysphagia were reported.
The results of this review should be interpreted with caution, since the small number of studies included in this review, as well as the small sample sizes included in these trials, may have resulted in unstable pooled estimates. The CI surrounding the point estimate of one of the studies conducted in the rehabilitation stage (10) was very large and probably contributed to the substantial statistical heterogeneity reported here. Due to the small number of studies available for pooling, we chose not to remove this study in a sensitivity analysis. Nutritional assessment techniques, including MNA, SGA or PG-SGA, were used in several of the studies. Since these assessment techniques require responses from patients, those with significant communication or cognitive impairments may have been excluded, skewing the sample towards those with less disabling strokes and potentially leading to an underestimation of the odds of malnutrition. A lack of reporting detail provided in the many of the included reports prevented us from exploring fully the effect of nutritional intake, co-morbidities and stroke severity on the relationship between dysphagia and malnutrition.
In conclusion, this review suggests that the odds of being malnourished were increased in the presence of dysphagia. When timing of stroke onset and assessment were considered in subgroup analysis, there was no increase in the odds of malnutrition in the acute phase of stroke. In the individual trials that did report an association, we suggest that the effect of stroke severity may have confounded the relationship between malnutrition and dysphagia, since a biological mechanism to explain their co-existence remains elusive. In the rehabilitation phase of stroke the odds of being malnourished were increased significantly, although it was impossible to ascertain whether clinical care practices, or lack thereof, contributed its development. Among the portion of dysphagic patients who were identified as malnourished, the most likely explanation was a prolonged period of inadequate dietary intake during inpatient hospitalization, highlighting the importance of closely monitoring the sufficiency of nutritional intake following stroke.
ACKNOWLEDGEMENT
This project was supported by funds from the Canadian Stroke Network.
REFERENCES