OBJECTIVE: To determine whether functional electrical stimulation-supported ergometric training of patients with multiple sclerosis has a prosthetic or therapeutic effect on biomechanical (power, smoothness of cycling) and functional outcomes (walking capability, strength of muscle, spasticity). DESIGN: Twelve subjects with multiple sclerosis participated in an electrical stimulation-supported ergometric training (3 sessions/week for 2 weeks). Measurements were made in a cross-over design to study prosthetic (with and without stimulation) and therapeutic effects (before and after training). METHODS: Power and smoothness were calculated by cadence and torque recordings of cycling and spasticity; strength and walking capability were measured by the Modified Ashworth Scale, Manual Muscle Test, and 10-Metre Walk Test. RESULTS: The power and smoothness of pedalling significantly improved prosthetically with electrical stimulation (p = 0.02), but did not show significant improvement over the 2 weeks of training. Significant short-term reductions in spasticity (before vs after training session; p < 0.05) were found. Isometric strength did not increase significantly during the 2-week training period and there was no improvement in walking ability.
CONCLUSION: Patients with multiple sclerosis are able to improve their cycling power and smoothness by pedalling with stimulation. We suggest that severely affected patients benefit more from functional electric stimulation-cycling therapy than do slightly affected patients.
Key words: multiple sclerosis, electric stimulation therapy, exercise therapy, cycle ergometer, muscle strength, muscle spasticity.
J Rehabil Med 2009; 41: 674–680
Correspondence address: Johann Szecsi, Centre for Sensorimotor Research, Department of Neurology, Ludwig-Maximillians University, Marchioninistrasse 23, DE-81377 Munich, Germany. E-mail: jszecsi@nefo.med.uni-muenchen.de
Submitted July 28, 2008; accepted April 28, 2009
INTRODUCTION
Two of the main symptoms of multiple sclerosis (MS) are impaired gait and postural imbalance, both of which have a negative impact on activities of daily living (1–3). Since cycling is practised in a sitting position, it is a safe and functionally effective exercise for these patients. Earlier research has shown that ergometric training of patients with MS improves their aerobic capacity (4, 5), functional capacity (5), isometric strength and psycho-mental factors (e.g. anxiety), and reduces fatigue (4).
Functional electric stimulation (FES)-propelled cycling has so far been applied successfully to persons with complete spinal cord injury (SCI) (6) to strengthen muscles (7), to stimulate the cardiovascular system (8, 9) and to improve cycling mobility (10, 11). Because the use of a FES approach in stroke rehabilitation is thought to facilitate the achievement of better functional output within a shorter period of time (12, 13), FES was recently combined with cycling for post-stroke patients (14), who participated in a treatment protocol programme that supported the active movement of paralysed muscles.
With the exception of an application in foot-drop systems (15), the effects of FES have so far been little investigated in patients with MS (16). Using stimulation of the quadriceps and hamstrings musculature, Livesley (17) did not find any evidence of improvements in subjectively experienced spasticity, range of motion, and strength in patients with MS. In a case study based on preliminary work (18), we reported a significant reduction in spasticity measured by the pendulum test in a patient with MS before and after FES-supported ergometric training during a single session.
To the best of our knowledge, neither the therapeutic effect of FES coupled with cycling in patients with MS is known, nor have the biomechanical parameters or functional outcome that could be improved by such therapy been investigated. However, a comparison of the FES-cycling of patients with partial motor and sensory pareses, for example patients with MS, with the FES-cycling of complete paraplegics revealed a few particularities. If sensation is partially or fully preserved, FES can be experienced as uncomfortable or even painful (19, 20). The resulting sensory or pain threshold defines the stimulation intensity that can be applied in each patient. Although low-intensity sensory stimulation is sometimes used in practice (21), most researchers believe that electrical stimulation that elicits muscle contraction is needed to increase voluntary strength (14, 16). Thus, the stimulation intensity has to be adjusted for each individual.
Furthermore, since patients with MS often still have considerable strength, they can, in most cases, engage in volitional cycling even without supportive FES. These patients often exhibit asymmetrical movement patterns due to unilateral muscle weakness, coordination deficits, or spasticity. Such symptoms manifest as non-smooth pedalling and low-power output during cycling. Finally, the performance of patients with MS can be strongly influenced by subjectively experienced fatigue and temperature changes that are particularly induced by the physical activity itself (22).
The principal aim of our study was to assess the effects of electrical stimulation on mechanical power output and the uniformity of pedalling (14, 23) during a 2-week FES-supported ergometric training of patients with MS with pareses of the lower limbs. Both prosthetic effects occurring during FES-supported cycling, as well as therapeutic, long-term effects (before and after the 2-week training period) were considered. Furthermore, the impact of the intervention on walking capability, spasticity, and volitional strength was investigated.
MATERIALS AND METHODS
Subjects
Twelve subjects (11 men/1 woman) were recruited to the study from the Clinics for Multiple Sclerosis in Kempfenhausen, Germany (inpatients) and the Department of Neurology of the University of Munich (outpatients).
Subjects were selected according to the following criteria: (i) they had chronic progressive MS; (ii) they had limited standing or walking capability due to weakness of the leg musculature (manual muscle test (MMT) (24) ≤ 3–4/5 knee extensor strength); and (iii) they were taking no anti-spastic medication, or had no scheduled change in medication.
Table I summarizes the clinical data and functional assessments of the study participants.
| Table I. Study participants with initial clinical and functional assessments |
| Patient number | Age, years /gender | Diagnosis (EDSS) | Duration of disease, years | Type of paresis | Anti-spastic medication, dosage, applied before training period, weeks | 10-MWT, sec/FAC | MAS | Strength (knee joint) |
| Extensor | Flexor |
| 1 | 51/M | MS (unknown) | 6 | Asymmetrical | – | 15 | 0.5 | 4 | 2.5 |
| 2 | 62/M | MS (4.0) | 10 | Asymmetrical | – | 9 | 1 | 3.5 | 3 |
| 3 | 53/M | MS (7.0) | 17 | Symmetrical | – | FAC 1 | 0.5 | 2.5 | 2 |
| 4 | 49/M | MS (5.0) | 9 | Asymmetrical | MP, 5 × 1000 mg, 3 weeks | 10 | 0 | 2 | 1 |
| 5 | 54/M | MS (6.5) | 30 | Symmetrical | – | 142 | 3 | 3 | 1 |
| 6 | 59/M | MS (6.5) | 18 | Symmetrical | – | 11 | 0 | 3 | 4 |
| 7 | 52/M | MS (7.5) | 8 | Symmetrical | – | FAC 0 | 2 | 3 | 0.75 |
| 8 | 37/F | MS (6.5) | 8 | Symmetrical | – | 20 | 2 | 3.5 | 3 |
| 9* | 54/M | MS (6.5) | 15 | Symmetrical | – | 55 | 2.5 | 3.5 | 1.5 |
| 10* | 47/M | MS (7.0) | 12 | Symmetrical | – | FAC 0 | 3.5 | – | 1 |
| 11* | 52/M | MS (8.0) | 30 | Symmetrical | MP, 5 × 500 mg, 2 weeks | FAC 0 | 3 | 2 | 0 |
| 12* | 41/M | MS (6.5) | 20 | Symmetrical | – | 73 | 0.75 | 3.5 | 1.5 |
| *Drop-out; – constant/no anti-spastic medication. 10-MWT: 10-m walk test; FAC: functional ambulation category; MAS: modified Ashworth scale (for statistical calculations we considered MAS grade 1+ as 1.5. For symmetrical pareses the mean value of both sides was considered); MS: multiple sclerosis; M: male; F: female; EDSS: Expanded Disability Status Scale for Multiple Sclerosis; MP: methylprednisolone. |
The participants showed moderate to severe functional limitations (Expanded Disability Status Scale (EDSS) = 4–8). Their mobility was greatly impaired according to the 10-Metre Walk Test (10-MWT (25)) or Functional Ambulation Category (FAC (26), when the 10-MWT was not applicable). The subjects were able to comprehend simple commands. The study was approved by the ethics committee of the University of Munich, and the subjects gave their informed consent prior to participation.
Training set-up
The subjects were scheduled to undergo 6 FES-supported cycling training sessions on a stationary ergometer for 2 weeks (every second working day, Fig. 1).
Fig. 1. Subject 3 with multiple sclerosis performing functional electric stimulation-supported cycling.
The protocol of a single training session is shown in Table II. In addition to ergometric training, inpatient subjects numbers 2–12 received conventional physiotherapy 5 times a week, and outpatient subject number 1 attended conventional outpatient physiotherapy sessions twice a week. All subjects had received conventional outpatient physiotherapy 2–5 times a week before they joined the study. No improvements in EDSS or 10-MWT scores had been documented in the medical records for at least 4 months before any of the subjects entered the study. Stimulation
| Table II. Training protocol |
| Time, min | Activity |
| 1–3 | Warm-up |
| 1–2 | Pre-stimulation phase |
| 2 | Stimulation phase |
| 1–2 | Early and late post-stimulation phase |
| Break 1–3 | |
| 1–2 | Pre-stimulation phase |
| 2 | Stimulation phase |
| 1–2 | Early and late post-stimulation phase |
| Break 1–3 | |
| 1–2 | Pre-stimulation phase |
| 2 | Stimulation phase |
| 1–2 | Early and late post-stimulation phase |
| 12–18 min total training (excl varm-up). 6 min functional electric stimulation-supported pedalling. |
The patient’s quadriceps and hamstring muscle groups on both sides were electrically stimulated during ergometric cycling. Although important for walking, the glutei muscle group was not stimulated for practical reasons. Pairs of auto-adhesive gel electrodes (Flextrode, Krauth + Timmermann Ltd, Hamburg, Germany) (size: 4.5 × 9.5 cm2) were placed on the skin over the proximal and distal quarter of each muscle bulk. A constant current, 8-channel stimulator (Motionstim, Krauth + Timmermann Ltd, Hamburg, Germany) provided the stimulation current (rectangular, biphasic, charged balanced pulses; frequency 20 Hz; maximum pulse amplitude 127 mA; constant pulse width 300 µs). These parameters are similar to those used in FES-cycling of subjects with complete paraplegia (27, 28), and no alternative electrical stimulation has yet proven superior for FES-cycling of subjects with incomplete paraplegia and preserved sensation (29).
During ergometric cycling the stimulator was controlled by serial communication from a personal computer. It directed the muscle stimulator to induce muscle contractions at the appropriate crank angles (10) so as to support voluntary pedalling. During stimulation- supported cycling, a maximum of individually tolerated stimulation intensity was set using a throttle, which was manually operated by the patient.
Ergometry
An ergometer with a motor-powered brake and drive (Theravital, Medica-Medizintechnik Ltd, Hochdorf, Germany) was used. Braking torque (accuracy 0.1 Nm) and crank angle were measured with an 8-bit incremental encoder (accuracy 1.4°), synchronized to turn with the crankshaft. Angular and torque data were recorded on a laptop at a sample rate of 20 Hz. Subjects performed cycling from their wheelchairs or used a chair coupled to the ergometer. The ankle joint was immobilized at 90°, and leg movement was restricted by shank and foot orthoses to the sagittal plane.
Before the first training session, and depending on the individual’s strength, the highest cycling resistance was selected that would allow the subject to tolerate well 12–18 min of active ergometric pedalling (with and without stimulation), but at the same time not become too exhausted.
Measurements
Biomechanical (cadence, torque, power, and smoothness of cycling) and functional outcome (walking capability, muscle strength, and spasticity) measurements were performed in a cross-over design to study prosthetic (with and without stimulation, Table I) and therapeutic effects (before and after training). Therapeutic effects were distinguished for the short and long term (before and after the daily training session or before and after the 2-week training period, respectively).
Biomechanical parameters
Crank angular position and torque were recorded during ergometer sessions; cadence, power, and smoothness of pedalling were derived. The cadence was calculated from the change of crank position over time. This was digitally filtered using a second-order Butterworth filter with a cut-off frequency of 4 Hz. Power was defined as the product of cadence and torque.
The method proposed by Chen and co-workers (23) was used to measure the smoothness of reciprocal pedalling. In their approach, the instantaneous cycling cadence is an undulating curve along the pedalling cycle rather than a straight line as would be expected in ideally smooth pedalling. The cadence was approximated by a smooth curve using a tenth-order polynomial fit.
The roughness index (RI), defined as the summation of the curvature for each instantaneous cranking speed, is given as:
360
RI = ∑ dR/ds
1
where R is the instantaneous cranking speed after polynomial curve fitting, and s is the crank position. RI will approach zero in smooth pedalling.
Functional outcome
Functional outcome was evaluated by walking capability, knee extensor and flexor strength, and spasticity, which has a functional significance for walking (30).
To evaluate walking capability, subjects had to perform the 10-MWT while using their usual walking aids (25). If they could not perform the 10-MWT (patient numbers 3,7, 10 and 11), they were evaluated according to the FAC (26).
Knee extensor and flexor strength were assessed by the MMT.
Spasticity was measured by the Modified Ashworth Scale (MAS) (31). Strength and spasticity on the more affected side were considered for asymmetrical pareses, and the mean value of both sides, for symmetrical pareses.
Data collection and reduction
Biomechanical parameters. To account for the prosthetic effects (comparison of values obtained with and without stimulation), mean power and smoothness were calculated for each subject over all training sessions with respect to the 4 comparison intervals (the last 30 sec of the pre-stimulation phase, the middle 30 sec of the stimulation phase, the middle 30 sec of the early post-stimulation phase, and the last 30 sec of the late post-stimulation phase, Table II).
Polynomial regression and interpolation of the cadence and the torque to 1° crank angle of the pedalling cycle for the 3 30-sec periods for each of the 4 comparison intervals yielded 12 cadence and torque profiles. Averaging over the 3 parts of the training session resulted in 4 values for the parameters power and smoothness for each subject. Furthermore, averages were computed for the 4 comparison intervals.
Finally, to analyse the effect of stimulation on power and smoothness, a repeated-measures one-way ANOVA with the factor comparison interval (4 levels: pre-stimulation, stimulation, early and late post-stimulation intervals) and Tukey post-hoc tests were performed.
Time course. To analyse the development of power and smoothness during the 2-week training period, averages were assigned in a first step to the 6 training sessions and for the 4 comparison intervals of the sessions. In a second step, a one-way ANOVA with factor session number was performed for the phase-related power and smoothness over the 2-week training time.
Functional outcome. Walking capability and spasticity (MAS) were evaluated before and after the first and last training sessions to study the therapeutic effects. Statistical analyses were performed for walking capability (10-MWT) and spasticity (MAS), using a two-way repeated measures ANOVA (factor A = first/last day, factor B = before/after the training session). Therefore, factors A and B stand for long-term and short-term therapeutic effects, respectively.
Data collected before the first and after the last training session were compared using a paired 1-sided t-test in order to assess muscle strength.
Statistical comparisons and regressions were considered significant if p ≤ 0.05.
RESULTS
Eight subjects completed the training and measurement protocols (patient numbers 1–8). Four subjects dropped out of the study before completion for the following reasons: (i) inpatient clinic left ahead of schedule (patient number 9); (ii) anti-spastic medication changed (patient number 10); (iii) failure to comply (patient number 12); and (iv) technical problems during transfer due to a high degree of disability (EDSS 8, patient number 11).
Biomechanical parameters (n = 8)
Power
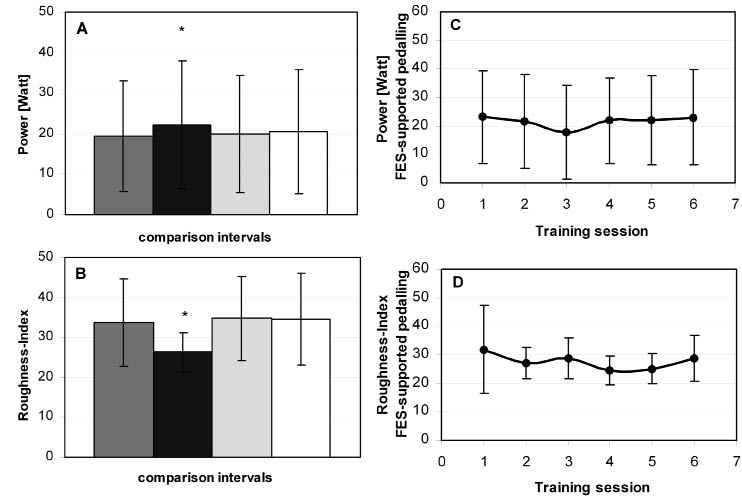
Prosthetic effects. Fig. 2A shows power generated during the 4 comparison intervals. Generated power increased significantly with stimulation compared with voluntary cycling in the pre-stimulation interval (mean increase +2.75 W, p = 0.02, 95% confidence interval (CI) 0.43–5.07). No carry-over of the prosthetic effect was found in the late (p > 0.5, mean increase +1.19 W, 95% CI –1.12 to 3.52) or early (p > 0.5, mean increase +0.47 W, 95% CI –1.85 to 2.79) post-stimulation intervals, compared with that seen in the pre-stimulation period. No significant difference could be detected between early and late post-stimulation intervals (p > 0.5).
Fig. 2. (A) Course of power and (B) smoothness, in one training session related to the comparison intervals (dark grey: before; black: during; light grey: early post-stimulation; white: late post-stimulation). Power and smoothness significantly improved during stimulation-supported pedalling. *p < 0.05. (C) Time course of power and (D) smoothness during the 2-week training period, considered only in the stimulated intervals. No significant changes occurred. Data are presented as group means and standard deviations. FES: functional electric stimulation.
Time course (Fig. 2C). The number of training sessions had no significant effect on the power generated with stimulation during the 2-week training period (p = 0.28). This was also true for the training intervals before and after stimulation (p = 0.5).
Smoothness of pedalling
Prosthetic effects. Fig. 2B depicts the smoothness of cycling in the 4 comparison intervals. Significantly better smoothness (p = 0.02, mean decrease in RI –7.35, 95% CI –13.47 to –1.23 ) was achieved in the stimulation interval than in the voluntary cycling interval beforehand. After cessation of stimulation the smoothness worsened significantly in comparison with that during the stimulated interval (p = 0.01, mean increase in RI +8.37, 95% CI 2.25–14.49). No significant change in smoothness was found when comparing intervals before and after stimulation (p > 0.5). Again, no significant (p > 0.2) difference in smoothness could be detected between early and late stimulation intervals.
Time course (Fig. 2D). The number of training sessions had no significant effect on the pedalling smoothness with stimulation during the 2-week training period (p = 0.38). This was also true for the training intervals before and after stimulation (p > 0.5).
Functional outcome
Walking capability (n = 8). No significant changes in walking capability could be found in either the short- (p > 0.77) or long-term (p > 0.67).
Muscle strength (n = 8). Both knee extensor and flexor strengths did not change significantly over the 2-week training period (mean increase extensor strength +0.37 Nm, p = 0.22, 95% CI –1.01 to 0.26; mean increase flexor strength +0.39 Nm, p =0.56, 95% CI –1.83 to 1.05).
Spasticity (MAS, n = 8). The 2-way ANOVA analysis of MAS revealed a significant reduction in muscle spasticity in the short term (pre/post training session, p = 0.05), but no significant reduction in the long term (first/last training days, p = 0.92). To determine the effect of the significant factor, pre- and post-MAS values were pooled from the first and the last training days. The MAS decreased from a mean value of 1.19 (95% CI 0.74–1.63) to 0.56 (95% CI 0.11–1.00), yielding a mean difference of 0.62 (95% CI 0.00–1.24).
DISCUSSION
Biomechanical parameters
The power-generating capability of muscle and the coordination control of the central nervous system (CNS) are prerequisites for locomotion, e.g. walking or cycling (32). Since previous research had suggested that smoothness of pedalling characterizes the ability to precisely recruit muscle activity (23), it was adopted as a measure of coordination control in this study. The main finding of the present study was that subjects with MS could achieve significantly more cycling power and smoothness with FES than without (prosthetic effect, Fig. 2A, B). This is in contrast to the situation of subjects with hemiplegia or other patient groups with incomplete sensory and motor pareses; they showed no prosthetic effect (14).
Power. The increase in power with FES, when the pre-stimulation phase is compared with the stimulation phase, amounts to 2.74/19.39 W = 14% (Fig. 2A). Moreover, power in the post-stimulation phase tended to remain increased compared with that in the pre-stimulation phase (Fig. 2A). Therefore, the question arises as to whether modifications in the training protocol could eventually lead to a longer-lasting power increase, even after cessation of the stimulation (see below).
The time course of power during the 2-week training period shows a slight (non-significant) fall on the third training session day (Fig. 2C). The cause of this phenomenon is not known. On analogy with the power drop observed in the FES-cycling of paraplegics (25), the occurrence of metabolically induced short-term fatigue might be caused by the muscle training.
Smoothness. As smoothness of cycling improved significantly with FES, the coordination deficits of cycling kinematics could be corrected (prosthetic effect).
Influence of stimulation intensity on the improvement of biomechanical parameters
Grouping the participants of the study according to the maximum tolerated current intensity showed that power increased (> 20%) and smoothness improved (≤ 10%) depending on stimulation intensity. This observation agrees with the presumed limitation of therapeutic effects due to too low stimulation intensities (16, 25), as discussed above (see Introduction). The subjects with low pain tolerance (numbers 4 and 8), as shown by low stimulation intensities (< 40 mA assumed to be the motor threshold), could not, as expected, increase their power or improve their smoothness. In contrast, the subjects with high pain tolerance (numbers 1, 2 and 7, > 55 mA) improved both their power and smoothness, probably independently of the severity or asymmetry of the impairment. Subjects with moderate pain tolerance (numbers 3, 5 and 6, 40–55 mA) achieved either power or smoothness improvements, presumably depending on the severity and asymmetry of their pareses and spasticity. On the basis of our hypotheses, we recommend using the FES-cycling method to develop endurance or promote coordination training:
• in subjects with high pain tolerance; or
• in subjects with medium pain tolerance, depending on the severity and asymmetry of the motor impairments.
• It is probably inappropriate for subjects with low pain tolerance to use this method.
Functional outcome
An increasing body of literature indicates that FES has positive effects on walking capability, muscle strength, and spasticity in stroke patients (16, 33, 34). There is no evidence as yet that FES has therapeutic effects in subjects with MS (16).
Impairments in patients with MS that are due to demyelination and axonal degeneration in the CNS are probably irreversible (35), whereas those that are consequences of reduced physical activity are reversible. A substantial part of these impairments seems to be the result of inactivity (36, 37); one can expect these impairments and functional output improvements to revert once FES-enhanced exercise is applied (38).
Our data show that walking capability did not change in the short- or long-term. The lack of therapeutic effect can perhaps be explained by the insufficiency of muscle strength and coordination improvement (as reflected by no improvement in smoothness) achieved over the 2-week training period (see below).
In agreement with a recent case report (18), the spastic muscle tone of our subjects decreased immediately after FES. In addition, no long-term reduction in muscle tone was measured over the 2 weeks of training.
Efficacy of FES-cycling from the viewpoint of patients. Regularly collected feedback from the participants revealed that they subjectively experienced positive outcomes. A comparison of these subjectively experienced results with initially measured EDSS, walking capability, spasticity, and muscle strength (Table I) showed again that the effect of FES-cycling depends on the severity of the disease and the predominant symptoms. In particular, those patients with a high degree of disability who were wheelchair users were able to improve their transfer (from wheelchair to seat) and their ability to stand up or to climb stairs (patient numbers 3 and 7). Subjects with considerable spasticity in activities of daily living (ADL) reported that FES-cycling allowed them to accomplish ADL more independently (patient numbers 5 and 7). Subjects who primarily had symptoms of gait disorders and compensated with a cane, walking frame, or peroneal orthosis reported experiencing gait improvements, such as qualitative improvement of leg lifting (patient numbers 1, 2, and 4). Lastly, a patient with considerable sensation deficits experienced a prickling and vitalizing sensation in the feet after FES-cycling (patient number 5).
Limitations and future work
The training protocol used in this study was compared with other conventional aerobic training programmes using the ergometer or cross-trainer (4, 5) for patients with MS. Those programmes were more intensive and of longer duration (e.g. 3 times/week, 15 weeks (4) or 30 min/day for 4 weeks) than our training protocol. Due to the disability of our patients (EDSS = 4–8, moderate to severe), the training sessions could not last longer than 3 times/week, each time for 6 min. The frequency and number of sessions (3 times/week and 6 sessions/training period, respectively) were determined by organizational constraints in the inpatient clinics. However, an increase only in the number of training sessions per week would probably not have improved the biomechanical outcome. This was shown by an additional subject with MS who met the inclusion criteria, and whose biomechanical outcome was the same after a more intensive training (5 sessions/week) than that received by the study participants (3 sessions/week).
It is debatable whether chronic functional effects should be expected at all in the brief training period of 2 weeks. The training period adopted was somewhat shorter than the lower limit of usual strength-increasing protocols with FES in stroke patients, including interventions lasting 3–8 weeks, with 3–10 interventions per week (16). Nevertheless, it was reported that even one session of cycling could achieve plastic changes in the CNS (increasing biceps brachii motor-evoked potential (39)) or spasticity amelioration (40). From a physiological viewpoint, the chronic stimulation of mammalian muscle in experiments has revealed that even if metabolic plasticity of muscles is manifested by fibre type transformation, it occurs only after 5 weeks, whereas higher levels of oxidative enzymes occur in fibres earlier, after 2 weeks (41).
Further research is therefore required to determine whether a more intensive (e.g. 5 training sessions/week) and longer training period (e.g. 4–8 weeks) would eventually have short-term or long-term carry-over effects on biomechanical and functional outcome.
Limitations of our study were the lack of a control group and no randomization. These factors could have influenced the therapeutic effects and therefore the functional outcome measurements. The relatively small number of study participants and the high percentage of dropouts (33%) could also have biased the results. Nevertheless, the effects revealed by this study can help to estimate the required number of participants for future (randomized and controlled) studies. Moreover, the number of dropouts can be minimized by considering only those subjects who would be likely to benefit from FES-cycling therapy (see above).
Although the MMT provides only a rough estimate of the muscle strength, the test was performed by an experienced physiotherapist, who was blinded to the cycling power measurements, which could eventually interfere with muscle strength determination. Finally, the training setup also included conventional physiotherapy in addition to FES-cycling. As all the study participants had chronic progressive MS and had shown no improvement in EDSS or 10-MWT scores in the pre-study months, we attribute the changes encountered in the study to the FES-cycling therapy.
In conclusion, the main effect of FES-assisted cycling in subjects with MS who received 3 sessions, each 6 min long (total = 18 min) per week for a training period of 2 weeks is the prosthetic improvement of power and smoothness. We suggest that severely affected patients benefit more from FES-cycling therapy than do slightly affected patients. Further research is needed to clarify whether a therapeutic gain can be achieved, in the sense of improved power, smoothness, walking capability, and spasticity after stimulation ceases.
ACKNOWLEDGEMENTS
The authors would like to thank Judy Benson for copyediting the manuscript.
This study was supported by a grant from the Else Kröner-Fresenius Foundation. Research grant: Else Kröner-Fresenius Foundation, Bad-Homburg, Germany.
REFERENCES