OBJECTIVE: To investigate the prevalence and course of passive shoulder range of motion in people with a spinal cord injury and the relationships between shoulder range of motion limitations and personal and lesion characteristics.
DESIGN: Multicentre longitudinal study.
SUBJECTS: A total of 199 subjects with spinal cord injury admitted to specialized rehabilitation centres.
METHODS: Assessments of shoulder range of motion at the start of active rehabilitation, 3 months later, at discharge and one year after discharge.
RESULTS: Up to 70% (95% confidence interval (CI): 57–81) of the subjects with tetraplegia and 29% (95% CI: 20–38) of those with paraplegia experienced a limited range of motion of the shoulder during, or in the first year after, inpatient rehabilitation. Shoulder flexion was affected most. Up to 26% (95% CI: 20–37) of subjects had a shoulder range of motion limitation on both sides. Increased age, tetraplegia, spasticity of elbow extensors and longer duration between injury and start of active rehabilitation increased the risk. Presence of shoulder pain is associated with limited shoulder range of motion.
CONCLUSION: Limited shoulder range of motion is common following spinal cord injury. Tetraplegia, increased age, spasticity of elbow extensors, longer duration between injury and start of active rehabilitation and shoulder pain are associated with an increased risk for shoulder range of motion problems and require extra attention.
Key words: spinal cord injuries, longitudinal survey, shoulder, range of motion, rehabilitation.
J Rehabil Med 2009; 41: 438–444
Correspondence address: I. E. Eriks-Hoogland, Swiss Paraplegic Research, CH-6207 Nottwil, Switzerland. E-mail: inge.eriks@paranet.ch
Submitted May 16, 2008; accepted January 21, 2009
INTRODUCTION
An unlimited range of motion (ROM) of the shoulder is necessary for various activities of daily living (ADL), e.g. reaching and perineal care. Shoulder ROM limitations may therefore lead to dependence on assistance with these activities (1, 2).
People with spinal cord injury (SCI) are highly dependent on the function of their upper limbs for mobility and ADL and are more at risk for problems associated with over-use of the shoulder than those without SCI (3). During rehabilitation, decreased shoulder ROM may limit participation in rehabilitation activities and thereby delay rehabilitation or lead to sub-optimal outcomes.
Most studies on shoulder problems in SCI have addressed shoulder pain (4–12). Few studies have focused on shoulder ROM (13–14) or the relationship between shoulder ROM and shoulder pain (7). A study of 89 men with SCI living in the community showed that 22% reported problems with shoulder ROM, and correlations were found with level and completeness of the lesion, age, shoulder pain and functional independence scores (13). Another study, of 41 patients with tetraplegia (7), showed that, during rehabilitation, patients with shoulder pain lost ROM in flexion, abduction, and external rotation at 90° abduction. The last finding was significant only for abduction on the left side. A loss of shoulder ROM was significantly related to previous shoulder injury on admission (7). A cross-sectional study of 352 subjects who had had tetraplegia for longer than 20 years showed that 12% had upper-extremity joint problems, encompassing shoulder and non-shoulder problems. Women and those with longer time since injury reported more upper extremity problems than men and those with short time since injury (14).
These studies, however, had several limitations, which hamper our understanding of the prevalence and course of shoulder ROM in people with SCI. The studies were mostly performed in chronic SCI, had a cross-sectional design or were relatively small. In addition, shoulder ROM and shoulder problems were not clearly defined.
In order to increase our understanding of the limitations in shoulder ROM in people with SCI during and after rehabilitation, as well as the relationships between shoulder ROM and personal and lesion characteristics, spasticity of elbow flexors and extensors, shoulder pain and time since injury at start of active rehabilitation, we assessed shoulder ROM (flexion, external rotation, and abduction) in a prospective cohort study with the following research questions: (i) What is the prevalence of shoulder ROM limitations in subjects with SCI at standardized time-points during inpatient rehabilitation and the first year after discharge? (ii) What is the course of shoulder ROM limitations in people with SCI during inpatient rehabilitation and the first year after discharge? (iii) What are the relationships between limitations in shoulder ROM and personal characteristics (age and gender), lesion characteristics (level, completeness of the lesion), time since injury, spasticity of elbow flexors and extensors and shoulder pain?
METHODS
Subjects
The present study was part of the Dutch research programme, “Physical strain, work capacity and mechanisms of restoration of mobility in the rehabilitation of persons with SCI”. After having received acute care in an academic or a large general hospital, subjects admitted to the SCI unit of one of 8 participating rehabilitation centres between May 2000 and September 2003 were included in the study if they met the following eligibility criteria: (i) acute SCI, classified as A, B, C or D on the American Spinal Injury Association (ASIA) impairment scale (15); (ii) age between 18 and 65 years; (iii) wheelchair dependent (using a wheelchair for daily mobility); (iv) sufficient comprehension of the Dutch language to understand the purpose of the study; and (v) not having a progressive or psychiatric condition that could interfere with constructive participation (16).
Procedure
Measurements were conducted following a standardized protocol by a trained research assistant at the start of active inpatient rehabilitation (t1) (defined as the moment when the subject was able to sit in a wheelchair ≥ 3 h), 3 months later (t2), at discharge of inpatient rehabilitation (t3) and one year after discharge (t4). If the subject was discharged within one month after t2, the assessment at t2 was considered the “discharge” measurement, and was included in the analyses as t3.
All subjects gave their written informed consent prior to the study. The study was approved by the medical ethics committee of the Stichting Revalidatie Limburg and the Institute for Rehabilitation Research and by all local medical ethics committees.
Measurements
Range of motion (ROM). Following a standardized protocol, passive ROM of both shoulders was measured in the sitting position for flexion, external rotation and abduction, using goniometry. Normal ROM was defined as: 180° for shoulder flexion, 60° for external rotation and 90° for glenohumeral abduction (17).
A decrease in ROM of 10° or more was considered to be an impaired ROM. This cut-off point was chosen by experts working in the field of SCI.
Personal and lesion characteristics. Age and gender of all subjects were recorded at t1. Level and completeness of the lesion were recorded at each measurement according to the ASIA impairment scale classification (15). Tetraplegia was defined as a lesion at or above the T1 segment. A lesion was defined as motor complete when subjects met the criteria of the ASIA Impairment Scale A or B.
Time since injury. For all subjects, time since injury (TSI) was determined as the time between the occurrence of SCI and t1 (in days) and was called TSIt1.
Spasticity. The presence of spasticity of the elbow flexors and extensors of both arms was determined in subjects with tetraplegia. Spasticity was defined as a velocity-dependent increase in muscle tone combined with exaggerated reflexes, through a direct standardized examination (1: catch; 2: clonus < 5 beats; 3: clonus ≥ 5 beats) (18).
Musculoskeletal pain. Subjects were asked in a standardized questionnaire if they experienced pain in the shoulder joint or muscles around the shoulder (for details see Van Drongelen et al. (5)). At t1, subjects were asked about shoulder pain since the time of injury . At t2, t3 and t4, subjects were asked if they had experienced pain since the previous measurement (no pain = 0, presence of pain = 1).
Statistical analysis
Firstly, shoulder ROM was measured and the prevalence of impaired shoulder ROM was calculated at each measurement. Changes in prevalence of impaired shoulder ROM between t1 and t3 were calculated in the total group and in subjects with paraplegia and tetraplegia separately. These calculations were also performed for the changes in prevalence between t3 and t4. Furthermore, the prevalence of limited shoulder ROM in one or both shoulders was calculated during and after rehabilitation.
Secondly, to determine whether the occurrence of impaired shoulder ROM changed significantly over time, the multilevel modelling programme MlwiN (MLwiN version 1.1; Centre for Multilevel Modelling, Institute of Education, London, UK) was used (19, 20). In the longitudinal data-set of this study, the hierarchy in the data is the repeated measurement “test occasion (t1–t4)” (level 1), which is grouped within the individual subjects (level 2), who are grouped in the rehabilitation centres (level 3). Limitations in shoulder ROM (no limitation = 0 and limitation = 1) for left and right side and each of the 3 movement direction separately, were the dependent variables in a multilevel binomial regression analysis. Time was modelled with 3 categorical dummy variables, with t3 as the reference to t1, t2 and t4. The regression coefficient for a time dummy describes the change in shoulder ROM limitations over that time period. In addition, to investigate the change in shoulder ROM limitations during the first 3 months of active rehabilitation (t1t2), the regression analysis was also performed with t1 as reference. The regression coefficients were converted to odds ratios (OR). An OR of 1 indicated that there was no association with this particular variable, whereas an OR > 1 indicated an increased risk of having limited shoulder ROM, and an OR < 1 indicated a decreased risk of having limited shoulder ROM in the presence of this risk factor. The robustness of our model was tested by analysing the course over time in those subjects with complete measurement data at t3 and t4.
Thirdly, to investigate the association of shoulder ROM limitations with personal characteristics (age, gender (men = 0; women = 1)), lesion characteristics (paraplegia = 1; tetraplegia = 0, incomplete = 0; complete = 1), TSIt1 (days), shoulder pain (yes = 1; no = 0) and spasticity of the elbow flexors and extensors (yes = 1; no = 0), were added to the model as independent variables. All variables were added individually to the basic model with the time dummies only. Independent variables with p-values < 0.1 were included in a subsequent multivariate model where a backward selection procedure was followed, excluding non-significant determinants (p > 0.05), in order to create the final multivariate model. The regression coefficients for all factors were converted to OR, as explained above. All models were made for shoulder flexion, external rotation and abduction and for the right and left shoulder separately.
RESULTS
Descriptive
At t1 199 subjects were included in the study. The mean age of subjects was 40.8 years (standard deviation (SD) 14.1 years). Of all the included subjects, 74% were male, 59% had paraplegia and 45% had a motor complete SCI. Overall, 48 subjects were lost to follow-up, for several reasons (16). At t1 the median TSI was 87 days with a minimum of 20 days and a maximum of 448 days.
Prevalence of limited ROM and residual ROM
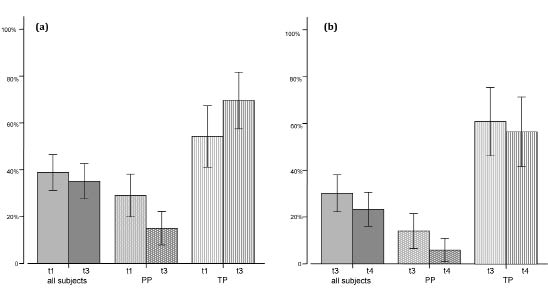
A limitation in shoulder ROM was present in up to 39% (95% CI: 31–46) of all subjects at the start of active rehabilitation (t1) and 23% (95% CI: 16–30) one year after rehabilitation (t4). Subjects with tetraplegia had much higher prevalences of limitation in shoulder ROM, and subjects with paraplegia had lower prevalences, as shown in Fig. 1.
Fig. 1. Percentage (and 95% confidence interval) of subjects with a shoulder range of motion (ROM) limitation in the overall group, in subjects with paraplegia (PP) and in subjects with tetraplegia (TP). (a) Percentages of subjects with complete measurement data-sets at start of active rehabilitation (t1) and at discharge (t3). (b) Percentages of subjects with complete data-sets at discharge (t3) and at one year after rehabilitation (t4).
Table I shows the percentages of subjects with limited shoulder flexion, external rotation and abduction at t1, t3 and t4 and the residual ROM. This shows that shoulder flexion is affected most.
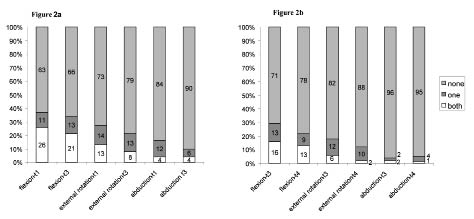
Fig. 2 shows the percentages of subjects without shoulder ROM limitation, and with shoulder ROM limitation in one or both shoulders at t1, t3 and t4.
Fig. 2. Percentage of subjects without limitations in shoulder range of motion (ROM), limitations in one shoulder and limitations in both shoulders. (a) Percentages of subjects with complete measurement data-sets at start active rehabilitation (t1) and at discharge (t3). (b) Percentages of subjects with complete data-sets at discharge (t3) and at one year after rehabilitation (t4).
|
Table I. Percentage of subjects with complete measurement data-sets at start of active rehabilitation (t1), at discharge (t3) and one year after discharge (t4) with limited shoulder range of motion (ROM) (% limitation) in flexion, external rotation or abduction. Normal ROM defined as 180° (flexion), 60° (external rotation), 90° (abduction). Of subjects with a limited ROM, mean residual ROM (in degrees) is given with standard deviation (SD) and range
|
|
|
Start of active rehabilitation to discharge
n = 160
|
Discharge to one year after discharge
n = 133
|
|
t1
|
t3
|
t3
|
t4
|
|
% limitation
|
Mean (SD)
|
Range
|
% limitation
|
Mean (SD)
|
Range
|
% limitation
|
Mean (SD)
|
Range
|
% limitation
|
Mean (SD)
|
Range
|
|
Flexion, °
|
|
Right
|
29
|
119 (34)
|
10–165
|
26
|
130 (36)
|
20–170
|
23
|
127 (42)
|
10–170
|
18
|
139 (30)
|
80–170
|
|
Left
|
33
|
118 (32)
|
30–170
|
28
|
134 (36)
|
20–170
|
22
|
135 (40)
|
20–170
|
16
|
144 (26)
|
80–170
|
|
External rotation, °
|
|
Right
|
18
|
25 (16)
|
0–50
|
14
|
28 (18)
|
0–50
|
12
|
31 (16)
|
0–50
|
5
|
37 (28)
|
0–50
|
|
Left
|
23
|
31 (19)
|
0–50
|
15
|
32 (18)
|
0–50
|
12
|
37 (13)
|
10–50
|
8
|
36 (14)
|
15–50
|
|
Abduction, °
|
|
Right
|
8
|
73 (18)
|
40–80
|
7
|
76 (8)
|
60–80
|
5
|
72 (16)
|
45–80
|
5
|
74 (5)
|
70–80
|
|
Left
|
12
|
74 (13)
|
45–80
|
6
|
72 (8)
|
65–80
|
2
|
78 (10)
|
70–80
|
1
|
80 (0)
|
80
|
Course of limitations in shoulder ROM over time
Table II shows the ORs of all shoulder ROM limitations at t1, t2, t4 compared with t3. No differences in risk of ROM limitations were found between t1 and t2 (left: flexion, OR = 1.0, p = 0.1; external rotation, OR = 0.9, p = 0.8; abduction, OR = 0.9, p = 0.8; right: flexion, OR = 1.1, p = 0.8; external rotation, OR = 1.8, p = 0.1; abduction, OR = 1.0, p = 0.9). Multilevel random coefficient analyses revealed that in our study population at the start of active rehabilitation (t1) the chance of having impaired shoulder external rotation or abduction for the left shoulder is 2.2 times higher than at discharge (p < 0.05). Three months after the start of active rehabilitation, we found a 2.6-times higher chance of having impaired shoulder external rotation for the right shoulder compared with time at discharge. One year after discharge a significantly decreased chance of having impaired shoulder flexion was found compared with discharge. For the right shoulder an OR of 0.5 was found, meaning a 2 times lower chance of limited ROM (Table II).
The results of testing the robustness of our model by including only participants with complete measurement data in t3 and t4 showed no different outcomes compared with the models in Table II.
|
Table II. Course of limitations in shoulder range of motion (ROM) as calculated with random coefficient analysis. Shown are the odds ratios (OR) and their 95% confidence intervals (95% CI) of having shoulder ROM limitations at t1, t2, t4 compared with t3
|
|
|
Flexion
|
External rotation
|
Abduction
|
|
β
|
OR
|
95% CI
|
β
|
OR
|
95% CI
|
β
|
OR
|
95% CI
|
|
Right
|
|
Cons
|
–1.8
|
|
|
–2.989
|
|
|
–2.886
|
|
|
|
∆t1t3
|
0.396
|
1.4
|
0.77–2.03
|
0.597
|
1.8
|
1.03–2.57
|
0.42
|
1.4
|
0.69–2.31
|
|
∆t2t3
|
0.574
|
1.8
|
1.14–2.46
|
0.962
|
2.6*
|
1.83–4.54
|
0.513
|
1.8
|
0.77–2.43
|
|
∆t4t3
|
–0.684
|
0.5
|
–0.26–1.26
|
–0.96
|
0.4
|
–2.31–0.69
|
–0.398
|
0.5
|
–0.32–1.72
|
|
Left
|
|
Cons
|
–1.517
|
|
|
–3.181
|
|
|
–2.844
|
|
|
|
∆t1t3
|
0.498
|
1.6
|
0.99–2.21
|
0.805
|
2.2
|
1.38–3.52
|
0.768
|
1.6
|
1.44–2.96
|
|
∆t2t3
|
0.449
|
1.6
|
0.96–2.24
|
0.683
|
2.0
|
1.16–2.95
|
0.667
|
1.6
|
0.90 –2.50
|
|
∆t4t3
|
–0.99
|
0.4
|
–0.37–1.17
|
–0.74
|
0.5
|
–1.74–0.51
|
–1.487
|
0.4
|
–1.33 –1.73
|
|
*Example: at t2 the risk of having limited right shoulder external rotation compared with t3 is 2.6 times higher.
t1: start of active rehabilitation; t2: 3 months after start of active rehabilitation; t3: at discharge; t4: one year after discharge; β: regression coefficient for each independent variable.
|
Relationship with personal and lesion characteristics, TSI, spasticity of elbow flexors, spasticity of elbow extensors and shoulder pain
Table III shows the relationship between limitations in shoulder ROM and age, gender, level of injury, completeness, TSI at t1, spasticity of elbow flexors, spasticity of elbow extensors and shoulder pain. When different results were found for the right and the left shoulder these are described in the text. In Table III the OR for age was calculated with an increase of one year and for TSI at t1 for every day. For clinical understanding, we described the OR for age with every increase of 10 years of age and TSI with every month (30 days).
|
Table III. Odds ratios (OR) and their 95% confidence intervals (95% CI) for the association with personal and lesion characteristics, TSIt1, spasticity of elbow flexors, spasticity of elbow extensors and pain after random coefficient analysis
|
|
|
Flexion
|
External rotation
|
Abduction
|
|
β
|
95% CI
|
OR
|
β
|
95% CI
|
OR
|
β
|
95% CI
|
OR
|
|
Right
|
|
Cons
|
–7.102
|
|
|
–3.769
|
|
|
–7.122
|
|
|
|
∆t1t3
|
0.352
|
0.66–2.14
|
1.4
|
0.725
|
1.41–2.79
|
2.1
|
0.550
|
0.78–2.62
|
1.7
|
|
∆t2t3
|
0.312
|
0.63–2.17
|
1.4
|
0.702
|
1.31–2.69
|
2.0
|
0.351
|
0.48–2.32
|
1.4
|
|
∆t4t3
|
–0.527
|
0.82–2.58
|
1.7
|
–0.428
|
0.58–2.42
|
1.5
|
–0.114
|
–0.05–2.25
|
1.1
|
|
Age
|
0.059
|
1.77–1.83
|
1.8*
|
ns
|
|
ns
|
0.052
|
1.77–1.83
|
1.8*
|
|
Gender
|
ns
|
|
ns
|
ns
|
|
ns
|
ns
|
|
ns
|
|
Level
|
2.319
|
9.36–11.04
|
10.2
|
1.504
|
3.90–5.10
|
4.5
|
1.847
|
5.40–7.20
|
6.3
|
|
Compl.
|
ns
|
|
ns
|
ns
|
|
ns
|
ns
|
|
ns
|
|
TSIt1
|
0.010
|
1.29–1.31
|
1.3†
|
ns
|
|
ns
|
ns
|
|
ns
|
|
Spasticity flexors
|
1.562
|
3.49–6.11
|
4.8
|
ns
|
|
ns
|
ns
|
|
ns
|
|
Spasticity extensors
|
ns
|
|
ns
|
0.925
|
1.63–3.37
|
2.5
|
1.334
|
2.70–4.90
|
3.8
|
|
Pain
|
1.829
|
5.54–6.68
|
6.2
|
1.311
|
3.16–4.24
|
3.7
|
1.512
|
3.74–5.26
|
4.5
|
|
Left
|
|
Cons
|
–7.152
|
|
|
–7.152
|
|
|
–6.686
|
|
|
|
∆t1t3
|
0.315
|
0.63–2.17
|
1.4
|
0.559
|
1.02–2.38
|
1.7
|
0.558
|
0.82–2.58
|
1.7
|
|
∆t2t3
|
0.087
|
0.29–1.91
|
1.1
|
0.329
|
0.71–2.09
|
1.4
|
0.506
|
0.82 –2.58
|
1.7
|
|
∆t4t3
|
–1.130
|
2.02–3.98
|
3.0
|
–0.264
|
0.46–2.14
|
1.3
|
–2.015
|
5.37–9.36
|
7.5
|
|
Age
|
0.050
|
1.57–1.63
|
1.6*
|
ns
|
|
ns
|
0.044
|
1.57–1.63
|
1.6*
|
|
Gender
|
ns
|
|
ns
|
ns
|
|
ns
|
ns
|
|
ns
|
|
Level
|
2.477
|
10.99–12.81
|
11.9‡
|
1.246
|
2.87–4.13
|
3.5
|
0.854
|
1.53–3.07
|
2.3
|
|
Compl.
|
ns
|
|
ns
|
ns
|
|
ns
|
ns
|
|
ns
|
|
TSIt1
|
0.013
|
1.49–1.51
|
1.5†
|
ns
|
|
ns
|
ns
|
|
ns
|
|
Spasticity flexors
|
ns
|
|
ns
|
ns
|
|
ns
|
ns
|
|
ns
|
|
Spasticity extensors
|
1.206
|
2.08–4.52
|
3.3
|
1.074
|
2.04–3.76
|
2.9
|
1.388
|
3.07–4.93
|
4.0
|
|
Pain
|
2.479
|
11.02–12.68
|
11.9
|
1.354
|
3.24–4.36
|
3.8
|
1.886
|
3.81–7.39
|
6.6
|
|
*OR for age for a period of 10 years.
†OR for TSI for period of one month.
‡Example: having tetraplegia was associated with a 11.9 times higher risk of having shoulder flexion limitations.
β: regression coefficient for each independent variable; t1: start of active rehabilitation; t2: 3 months after start of active rehabilitation; t3: at discharge; t4: one year after discharge; ∆t1t3: t1 compared with t3; ∆t2t3: t2 compared with t3; ∆t4t3: t4 compared with t3; Compl.: completeness of the lesion; TSIt1: time since injury at t1; ns: not significant.
|
Shoulder flexion
Subjects with tetraplegia, of older age, with longer duration until start of active rehabilitation (TSIt1) and shoulder pain are at risk for having limited shoulder flexion. With every 10-year increase in age the chance of having limited shoulder flexion is 1.8 times higher for the right shoulder and 1.6 times for the left shoulder. This means that a 50-year-old subject has a 1.8 (and 1.6, respectively) times higher chance of developing limited shoulder flexion compared with a 40-year-old subject. TSI at t1 was found to be a risk factor for limited shoulder flexion for both shoulders. Every month delay of active rehabilitation increases the chance of having shoulder flexion problems, by 1.3 for the right and 1.5 for the left shoulder. For the left shoulder only, spasticity of the elbow extensors increases the chance of having limitations of shoulder flexion. For the right shoulder only, spasticity of the elbow flexors increases the chance of limited shoulder flexion.
Shoulder external rotation
Having tetraplegia, spasticity of the elbow extensors and presence of shoulder pain was associated with a higher chance of having limited shoulder external rotation. For example, subjects with pain in the left shoulder had a 3.8 times higher chance of having limited shoulder external rotation.
Shoulder abduction
Older age, tetraplegia, spasticity of the elbow extensors and the presence of shoulder pain were associated with shoulder abduction limitations for both shoulders. With every increase in age of 10 years the chance of having limited shoulder abduction increases to 1.8 for the right and 1.6 times for the left shoulder.
DISCUSSION
Prevalence of limited ROM and residual ROM
Limitations in shoulder ROM were present in a significant proportion of subjects with SCI in our study. For those subjects with tetraplegia, in particular, high prevalences were found during and after inpatient rehabilitation. Comparison of our results with the studies of Salisbury et al. (7) and Ballinger et al. (13) should be made with caution due to the inclusion criteria for the study sample (e.g. only wheelchair-dependent subjects). A study by Sinott et al. (21) in persons with long-term paraplegia showed that 82% of the 22 persons with a T2 to T7 lesion and 40% of the 20 persons with a T8 to T12 lesion were diagnosed with rotator cuff disorders. Ballinger et al. (13) found ROM problems in 22% of a group of 89 men with long-term traumatic SCI (45% paraplegia, TSI: average 10 years, range 1–48 years).
Our study showed that shoulder flexion, in particular, was affected at t1 in up to 26% (95% CI: 20–37) of subjects in both shoulders. Sinnott et al. (21) found limited ROM in both shoulders in 43% of the persons with long-term paraplegia. It is possible that a limitation of ROM of both shoulders places an even greater burden on the patient with respect to his/her possibilities of actively taking part in the rehabilitation programme and achieving functional independence.
The mean residual ROM for each movement does not show much variation over time (Table I). The range, however, is broad and shows that the severity of shoulder ROM limitations varies strongly between individuals. The clinical relevance of ROM is that unlimited ROM is conditional to be able to perform functional activities such as transfers and reaching. Magermans et al. (1) described the requirements for upper extremity motion during activities of daily living in able-bodied persons. Their study showed, for example, that for reaching a mean glenohumeral elevation of 121.4 degrees is needed. This indicates that a substantial part of our subjects have such severe shoulder ROM limitations that they are restricted in this activity.
Course of limitations of shoulder ROM over time
Shoulder external rotation was shown to be most at risk during inpatient rehabilitation and shoulder flexion after inpatient rehabilitation. Special attention is necessary in the acute phase and during inpatient rehabilitation to prevent limited shoulder external rotation. In the acute phase optimal shoulder positioning and early mobilization are therefore still important since, in our study and the study of Waring & Maynard (22), prolonged immobilization is found to contribute to limited shoulder ROM. The start of active rehabilitation means a higher demand on the shoulder, which is thought to be a risk for overuse. A relationship has been described in the literature between specific joint forces and moments and measures of shoulder pathology in subjects with paraplegia (23, 24). The study by Van Drongelen (25) underlines the theory that muscle imbalance is a major risk factor for developing shoulder problems in SCI, such as pain and limitations in ROM.
After rehabilitation the focus of attention should shift towards prevention of shoulder flexion ROM limitations. Overuse of the shoulder could lead to damage of the structures of the shoulder and may therefore lead to limited shoulder ROM (26).
Relationship between shoulder ROM limitations and personal and lesion characteristics, TSIt1, spasticity of elbow flexors and extensors and pain
Having a tetraplegia was shown to be the most important risk factor for shoulder ROM limitations during and one year after rehabilitation. At and above the level of C5, shoulder muscles are impaired, creating an imbalance of shoulder musculature and thus making the shoulder vulnerable to overuse. In the literature this imbalance is often postulated to be the cause of shoulder pain and ROM problems in wheelchair-dependent persons (6, 22, 23). Another important factor for shoulder functioning and functional end-level is the role of postural control (27). This is often seen in the choice of wheelchair design (without trunk stabilization) and striving for independent transfers and manual wheelchairs, even in persons with tetraplegia. We should ask ourselves whether these choices are justified in the long-term.
Older age was found to be a risk factor for limited shoulder ROM. It has been shown that degenerative changes of the shoulder joint occur as early as 40 years of age (28) and that ageing with an SCI leads to an increase in physical assistance as most people, for example, need more help to make a transfer (29). Although problems with shoulder ROM could be regarded as a complication of SCI (30), age-related problems may contribute to shoulder problems and may even be amplified in SCI.
Prolonged immobilization was shown to be a risk factor for shoulder ROM limitations in the present study. The importance of early mobilization and proper shoulder positioning has been described previously.
In this study shoulder pain was also shown to be associated strongly with limited shoulder ROM. In our study we clearly distinguished between musculoskeletal pain and other sensations of pain. However, one should be careful to address all reported pain to physical damage. The impact of pain is influenced not only by physical factors but also by psychosocial factors (31). It was beyond the scope of our study to investigate the aetiology and pathology of shoulder ROM; therefore we cannot answer the question as to what causes limitations of shoulder ROM. Studies of radiographic changes in the shoulders of subjects with SCI (19, 32–34) show that physical changes are often present, but no consistent findings have yet been published.
This study showed that spasticity of the elbow flexors increased the risk for developing limited shoulder flexion for the right shoulder only. In daily practice spasticity of the m. biceps brachii is found to cause the most problems in shoulder ROM and is often treated with oral medication or local medication like botulin toxin injections. Spasticity of the elbow extensors was found to be related to an increased risk for all measured shoulder ROMs for both shoulders. Spasticity of the m. triceps brachii, even when present, is less often a reason for treatment. No literature was found to explain these results.
In contrast to the literature (14), in our study female gender was not shown to be a risk factor for limitation of shoulder ROM.
Limitations, clinical implications and future research
When interpreting the data of the current study, one should bear in mind that we measured only wheelchair-dependent subjects, and therefore cannot generalize our results to those persons with SCI who are not wheelchair dependent. In clinical practice wheelchair-dependent subjects seem to be most affected by shoulder problems, which justifies this choice.
The drop-out at t4 could have caused bias. Using random coefficient analyses, however, gave us the possibility to include all present subjects at each measurement time and provided us with realistic data on the occurrence of shoulder ROM limitations during each interval. Insight into the course of problems with shoulder ROM was guaranteed by the longitudinal design of the study. This contributes to the understanding of this problem.
Limitations of shoulder ROM are common following SCI during and after inpatient rehabilitation. People with tetraplegia are especially at risk of developing shoulder ROM limitations. Furthermore, increased age, spasticity of elbow extensors, prolonged immobilization and shoulder pain are determinants of an increased risk for shoulder ROM problems and require extra attention during rehabilitation and after discharge.
Future research would ideally involve a more comprehensive approach. A longitudinal study that addresses shoulder ROM and relates it to pain, structural changes and ageing will provide more insight into the cause and development of limitations of shoulder ROM. We should bear in mind that not only physical changes can cause shoulder problems in people with SCI. To understand the complex relationship between shoulder ROM, shoulder pain and spasticity one should also take into account physiological causes, such as the presence of depression. To really understand the magnitude of shoulder problems in people with SCI, one should determine what level of shoulder ROM is needed in wheelchair-dependent persons and, ideally, such a study should also measure restrictions in activities and participation.
ACKNOWLEDGEMENTS
This study was supported by the Netherlands Organization for Health Research and Development (ZonMW), under grants 14350003 and 14350010, and is part of the research programme “Physical strain, work capacity and mechanisms of restoration of mobility in the rehabilitation of individuals with SCI”.
The work of the research assistants (Annelieke Niezen, Hennie Rijken, Ferry Woldring, Karin Postma, Jos Bloemen, Linda Valent, Sacha van Langeveld and Marijke Schuitemaker) and the rehabilitation physicians is gratefully acknowledged. We also thank the 8 rehabilitation centres: Rehabilitation Center Amsterdam, De Hoogstraat (Utrecht); Het Roessingh (Enschede); Rijndam Revalidatiecentrum (Rotterdam); Hoensbroeck Revalidatiecentrum (Hoensbroek); Sint Maartenskliniek (Nijmegen); Beatrixoord (Haren); and Heliomare (Wijk aan Zee); and all of the subjects for their participation. Special thanks are extended to Govert Snoek and Roger Hilfiker for their input.
REFERENCES