OBJECTIVES: To compare self-reported mental health in trauma survivors with and without brain injury; to describe factors associated with lower mental health; and to compare needs in terms of mental health services and perceived access limitations to such services.
DESIGN: Cross-sectional community survey.
Patients: A total of 405 trauma survivors (239 with traumatic brain injury and 166 without) interviewed 2–4 years post-injury.
METHODS: Short Form-12 mental health scales and a survey measuring perceived needs for mental health services, and access limitations.
RESULTS: Injury survivors with and without traumatic brain injury are similarly affected on subjective reports of global mental health, vitality, role changes, and social functioning except for cognitive complaints. Variables associated with lower mental health in trauma survivors include younger age, being a woman, shorter time since injury, higher pain, lower social support, and presence of cognitive problems. Although individuals with traumatic brain injury report slightly more mental health problems and more need for mental health services, proportionally to their needs, more individuals without traumatic brain injury report access limitations to mental health services.
CONCLUSION: Mental health problems affect important proportions of trauma survivors, either with or without traumatic brain injury. More effort should be made to facilitate access to mental health services for all trauma survivors.
Key words: multiple trauma, brain injuries, mental health services, health services accessibility.
J Rehabil Med 2009; 41: 179–186
Correspondence address: Marie-Christine Ouellet, Axe de recherche en traumatologie-Médecine d’urgence-Soins Intensifs, Centre de recherche du CHAUQ, Hôpital de l’Enfant-Jésus du CHA, Pavillon Notre-Dame, Local H-044, 1401, 18e Rue, Québec G1J 1Z4, Canada. E-mail: marie-christine.ouellet@mail.mcgill.ca
Submitted March 28, 2008; accepted September 29, 2008
INTRODUCTION
Survivors of traumatic injuries are likely to experience multiple stressors (e.g. medical interventions, adjustment to limitations, pain, inability to return to work, redefinition of roles) that can potentially precipitate mental health problems. Furthermore, individuals who sustain traumatic injuries include an overrepresentation of individuals with pre-injury substance abuse, lower education, unstable work history, psychiatric histories and risk-taking behaviors (1, 2), factors which may put them more at risk for developing mental health problems after trauma. The bulk of research on mental health issues following orthopedic injuries or multiple trauma has focused on post-traumatic stress disorder, which is only one specific mental health problem that may occur following an injury. There are few studies of more general mental health problems following physical trauma (e.g. depression or anxiety) and data reporting on psychological outcome beyond one year is rare. Moreover, this literature is characterized by a wide variability in terms of definition of mental health problems, their measurement, and inclusion or exclusion criteria. For example, individuals with mild head injury may or may not be included in different studies. Nonetheless, this research indicates that psychological complications following trauma without neurological involvement are common and seemingly persistent. O’Donnell and colleagues (3) studied 363 consecutive admissions to a level I trauma center 3 and 12 months post-injury, excluding patients with moderate or severe traumatic brain injury (TBI). They found that more than 20% of their sample met the diagnostic criteria for a psychiatric disorder at 1-year post-injury. In a study of severe lower-limb injury patients, McCarthy et al. (4) found that 42–48% of their sample screened positive for a possible psychological disorder between 3 and 24 months post-injury. Reports of anxiety and depression symptoms in the few weeks following trauma have varied as widely as 8–78% (5–7). Anxiety and depression affect proportions of individuals varying from 7% to 17% at 3–6 months post-injury (3, 6–8) 6–19% at 1-year (3, 8), and from 11% to 30% beyond 2 years (9, 10). Thus, needs in the mental health domain seem significant following trauma, yet it remains unclear if traumatic injury survivors have access to appropriate services relating to mental health.
Much scientific attention has already been devoted to mental health issues following trauma that involves TBI. Recently, McCarthy and colleagues (11) reported that one-third of adults with TBI reported poor psychosocial health at one year post-injury. The prevalence of depressive and anxiety problems in patients with TBI has been found to be as high as 57% and 70%, respectively (12, 13). High rates of emotional difficulties and depression have been documented up to 5 years post-TBI (1, 12, 14–16). Studies comparing traumatic injury survivors with and without brain injury are rare however. Four studies have used orthopedic or multiple trauma patients without any head injury as controls to evaluate mental health outcomes in patients with TBI 1–5 years post-injury (15, 17–19). Interestingly, all of these groups found high rates of emotional difficulties (e.g. high rates of anxiety and depressive symptoms) in both their TBI and trauma control groups with no statistically significant differences. Furthermore, the severity of these symptoms was not related to time since injury and no improvement was seen on longitudinal measures, suggesting a chronic course for these psychological complications.
Injury survivors with and without brain injury share similar stressors, but also face different challenges. For example, both groups must come to grips with acquired limitations, changes in roles, and issues related to return to work. Cognitive problems are more specific to TBI, however, and issues related to pain might be more important in the multiple or orthopedic trauma survivors. These different challenges may contribute to the development of similar mental health issues, such as anxiety, depression or problems in interpersonal relationships. No study has yet tried to identify how different and similar factors may influence mental health in these 2 sub-groups of the trauma population.
Despite clear data showing that mental health issues are important to address whether the trauma involved the brain or not, very few authors have described the needs of traumatic injury survivors in terms of services aimed at enhancing mental health or psychological well-being. Even fewer authors have documented the accessibility or barriers to such types of services. Corrigan et al. (20) indicated that the 2 most frequently expressed needs following TBI are needs to improve memory and problem-solving skills and to manage stress and emotional upsets. Heinemann et al. (21) found that approximately 40% of TBI survivors expressed a need for managing stress and emotional upsets and improving their mood. The most prevalent unmet need reported in their sample was related to improving memory or problem-solving skills. Recently, Pickelsimer et al. (22) found that the second most frequently cited need following TBI, after the need for “receiving information about services”, was “improving mood, managing stress, or emotional upsets”. They also found that at least 17% of persons reporting such a need were unable to receive adequate services because they were either unaware that help may be available or did not know where to look for appropriate help. Thus mental health issues are top needs following TBI. To our knowledge, no study has yet described the needs for mental health services in traumatic injury survivors without TBI. Yet it is clear that this group also has important needs that should be addressed.
In the context of a larger epidemiological survey seeking to obtain a global portrait of long-term health and functional status after severe traumatic injuries, the present study aimed: (i) to compare self-reported mental health status in traumatic injury survivors with (TBI) and without brain injury (non-TBI); (ii) to describe factors associated with perceived lower mental health; and (iii) to compare traumatic injury survivors with and without brain injury in terms of perceived needs for services relating to mental health and their perceived access to such services. We hypothesized that both groups would be similar in terms of reported mental health status except for higher cognitive problems in the survivors with TBI. We expected several socio-demographic and clinical factors to be associated with lower mental health, such as gender, the severity of the injury, and the presence of pain, cognitive problems, or co-morbid health problems. We expected higher needs for mental health services in the TBI group.
METHODS
Participants
The sample was composed of 405 trauma patients (239 with and 166 without brain injury) admitted to 10 level I and level II trauma centers in the province of Québec, Canada, between January 2000 and December 2001. Participants were identified via the Quebec Trauma Registry data provided by all trauma centers. The inclusion criteria in the Quebec Trauma Registry are standard across centers and consist in the presence of any of these 4 conditions: (i) admission for more than 2 days after a traumatic injury; (ii) admission to the intensive care unit; (iii) emergency room or in-hospital death; or (iv) transfer from another hospital. The registry contains complete prospectively collected information on patients’ injuries, hospital history from emergency room to discharge and destination at discharge.
Individuals between 18 and 65 years who were traumatic injury survivors who required post-acute rehabilitation after discharge from the hospital were included in this study, which was part of a larger scale study aiming at evaluating functional outcome following trauma in urban and rural regions (23).
Among 642 eligible participants contacted by telephone, 435 (67.8 %) responded to the survey, 97 (15.1%) denied participation, 79 (12.3%) could not be contacted, and 31 (4.8%) were excluded because of legal competence. Thirty individuals were also excluded from the present analyses because another person responded to the survey in their place.
Data from the Quebec Trauma Registry allowed a comparison between responders and non-responders, given as mean with standard deviation (SD). The non-responders (excluding participants for whom a proxy responded to the survey in the larger-scale study) were not different from the responders with regards to age (41.1 (SD 15.1) vs 41.2 (SD 14.9) years, p = 0.97), Injury Severity Scores (ISS) (23.6 (SD 11.7) vs 23.4 (SD 10.9), p = 0.85) and number of body regions injured (8.6 (SD 6.2) vs 8.4 (SD 5.3), p = 0.68). Gender was significantly different between responders and non-responders; 73.4 % of non-responders were men, compared with 64.6% among the responders (p = 0.03). Participants excluded because a proxy responded to the survey were not different from the responders in terms of age and number of body regions injured, but had suffered significantly more severe injuries (mean ISS score of 30.7 (SD 11.6), p < 0.001) and were more often men (p = 0.03).
The final sample thus included 405 participants. Patients with minor injuries (e.g. minor fractures, lacerations or minor head trauma) who were not admitted to the intensive care unit (ICU) nor hospitalized for more than 2 days were not included in the trauma registry and were thus not included in this study. The sample was subdivided in 2 according to the presence (TBI) or absence (non-TBI) of a brain injury. Because even minor TBI (which may accompany orthopedic trauma) influences cognition and mental health it was important for us to use a conservative way of categorizing TBI and non-TBI trauma survivors: thus even if a patient presented no visible brain lesion but had an altered level of consciousness, this patient was categorized in the TBI group. More specifically, presence of brain injury was noted if the Quebec Trauma Registry included any of the following Abbreviated Injury Scale (AIS), 24) codes (the digit to the right is the AIS severity code ranging from 1 (minor) to 6 (maximum) with 9 as unknown) : 115099.9 (closed head injury); 113000.6 (Crush: Massive destruction of both cranium and brain); 115299.9 (traumatic brain injury); 116002.3 and 116004.5 (penetrating injuries); 120202.5 to 122806.3 (lesions to intracranial vessels); 130202.2 to 132604.2 (lesions to cranial nerves); 140202.5 to 140799.3 (lesions to cerebral internal organs); 150000.2 to 150408.4 (skull or vault fractures); 160202.2 to 160214.5 (unconsciousness); 160402.1 to 161000.2 (altered level of consciousness).
Procedure
The study was approved by the Commission d’accès à l’information du Québec (Quebec Information Access Board) and the Ethics Review Board of each of the 10 participating trauma centers. Participants’ consent was obtained verbally over the telephone.
A 45–60-min structured telephone interview was conducted with all participants. It included 73 questions organized into 6 sections: 1) socio-demographic information, 2) needs for rehabilitation services and access to such services, 3) Medical Outcomes Study – Short Form (SF-12), 4) functional status (reported elsewhere (25)), 5) co-morbid physical health problems, and 6) and social support. Prior to the data collection period, the questionnaire was tested over the telephone with 25 healthy adult volunteers. The data was obtained from October 2003 to September 2004. The telephone interviews were conducted by 4 trained research assistants who were all students in medicine. The integrity and quality of the data collection process was ensured by weekly meetings between investigators and research assistants.
Main outcome measures
Perceived mental health status. The Mental Component Summary score and individual scales related to mental health (Vitality, Social Functioning, Role-Emotional, and Mental Health) of the second version of the Medical Outcomes Study – Short Form (SF-12v2 (26)) were used to measure self-perceived psychosocial health. A Canadian French-language version of this instrument was used with French-speaking individuals (questions taken from the SF-36 Canadian French-language validated version (27)). The SF-12 contains 12 questions that address physical functioning, role limitation due to physical health problems, bodily pain, general health, vitality, social functioning, role limitations due to emotional health problems and mental health. Each scale can range from 0 (worst outcome) to 100 (best outcome) score. The scales can be aggregated in order to provide a Physical Component Summary score and a Mental Component Summary score. In this study, we examined only the Mental Component Summary score and individual scales related to mental health (Vitality, Social Functioning, Role-Emotional, and Mental Health). Results related to physical health are reported elsewhere (25). Reliability coefficients for the 4 SF-12v2 mental health and the Mental Component Summary Score scales range from 0.74 to 0.87 (26). The validity of the SF-12 is well established: this instrument has been shown to distinguish individuals suffering from diverse psychiatric conditions (26). One study using the SF-36 found that this instrument was a reliable and valid measure for use with individuals having sustained TBI (28).
MacKenzie et al. (29) have proposed and validated the addition of a cognitive scale (COG) to supplement the SF-36 version in studies of outcome after multiple trauma involving head injury. This scale taps into perceived difficulties with: (i) reasoning and solving problems; (ii) memory for recent events; (iii) sustaining attention; and (iv) concentration and thinking. With French-speaking individuals, we used a French translation of the 4 items. Unfortunately, the psychometric properties of the French translation have not yet been formally evaluated.
Potential correlates of mental health
Demographic variables. Age at injury and gender were directly available in trauma registry data. The participants’ pre-injury level of education, working and marital status were gathered during the interviews using the demographic section of the Enquête Sociale et de Santé 1998 (30).
Injury Severity Score. The ISS is a measure of anatomic severity of injuries that provides an overall score for patients with multiple injuries. Each injury is assigned an AIS (24). The sum of squares of the highest AIS grade in the 3 most severely injured body regions is used to produce the ISS which ranges from 1 (minor) to 75 (most likely lethal). The ISS and Time since injury were directly computed from the trauma registry data.
Self-reported co-morbid health problems. The presence of coexisting medical conditions was measured by counts of self-reported conditions at the time of the interview. A list of 16 physical and 3 mental or cognitive problems was derived from the Enquête Sociale et de Santé 1998 questionnaire (30). The Enquête Sociale et de Santé is conducted every 5 years or so in representative samples of more than 30000 Quebec households (French- and English-speaking) and is well adapted to the Quebec general population. Participants were asked if they presented (yes/no) any of these health problems. Physical health problems included 16 conditions such as serious back, neck or spinal pain, cancer, respiratory problems, epilepsy, gastro-intestinal problems, or cardiac conditions. Mental health problems included depression, periods of important anxiety or irritability, and periods of important confusion or memory problems. These 3 mental health problems were endorsed by less than 5% of the Quebec population in health surveys conducted in 1987, 1992 and 1998 (31).
Social support. In this study, we used the Social Support Index of the Enquête Sociale et de Santé 1998 (30), which was used and validated among the general population of Quebec. The Social Support Index is constructed from 11 questions that inquire about both the quantity and satisfaction with available practical and emotional support from friends, family and the entourage. The Social Support Index raw scores are transformed on a scale ranging from 13 to 100, with higher scores reflecting higher social support.
Pain rating. Pain was assessed with the SF-12 question relating to pain. On a 5-point Likert scale ranging from “Not at all” to “Extremely”, participants answered the following question: “How much did pain interfere with your normal work (including both work outside the home and housework)?”.
Needs for rehabilitation services related to mental health
Self-perceived needs for 6 types of services related to mental health were evaluated: 1) cognitive rehabilitation, 2) therapy for communication problems (e.g. speech therapy), 3) psychotherapy, 4) family or couple therapy, 5) work or school counseling services, and 6) special education services. For each service, participants were asked whether 1) they needed or would have needed the services (yes/no) and 2) if they had encountered barriers to access the services (yes/no). A typical question was “Since your discharge from hospital did you need, or would you have needed, psychotherapy to cope with difficulties in your life resulting from your injury”? If participants answered yes, then they were asked “Did you encounter difficulties obtaining this service”? Four types of barriers were described: 1) unavailability of service, 2) geographic barriers (e.g. long distances preventing regular visits to service providers), 3) financial barriers (e.g. inability to afford the service) and 4) time barriers (e.g. waiting list). Access limitation to rehabilitation services was coded as positive if at least 1 of the 4 types of barriers was encountered. Unfortunately, the specific type of barrier was not coded for further data analysis in the original survey.
Data analysis
The 2 groups were compared on demographic and injury characteristics. Categorical variables were tested by χ2 and continuous variables with t-test analyses. The 2 groups were then compared on the SF-12 scale scores with independent group t-tests (Objective 1). Differences between groups were considered significant at the alpha level of 0.05. Percentages were computed to describe perceived needs for mental health services (Objective 3).
In order to explore the factors associated with low mental health-related quality of life (Objective 2), a direct logistic regression analysis was carried on the global sample. Low mental health was defined as a SF-12 Mental Component Score lower than 43.5, the cut-off for the 25th percentile in the US general population (26) (no normative data for the SF-12 is available for the Quebec population for the Mental Component Score). In direct logistic regression, all variables are entered in the equation simultaneously: since the analysis is exploratory, there is no specific hypothesis about the order of importance of different factors. This method provides an estimation of the contribution of each variable over and above the other variables (32). An alpha level of 0.05 was chosen to identify variables significantly associated with the outcome. Eleven variables, chosen for their potential predictive value based on the literature on psychological distress following trauma, were entered in the regression analysis: age, gender, marital status (living alone vs with a spouse), education, occupation (presently active or retired vs on disability leave), ISS, Time since injury, Pain rating, Social Support Index score, number of co-morbid physical health problems reported, and presence or absence of reported cognitive problems (confusion or memory loss). In order to explore if variables associated with lower mental health differed among TBI and non-TBI traumatic injury survivors, the logistic regressions were re-run for each group separately.
The sample sizes were adequate considering the recommended number of 8–10 participants per variable for logistic regression (32). The analyses were completed using the Statistical Package for Social Sciences (SPSS), version 11.0.
RESULTS
Table I presents the socio-demographic, injury and health variables for the TBI and non-TBI groups. The mean age at the time of injury was 41.1 years (SD = 15.1) and men composed 63.3% of the total sample. The distribution of gender, marital status and education did not differ significantly among groups. As could be expected, however, individuals in the TBI group were significantly younger, more frequently on disability leave, and less often retired than the non-TBI group. With regards to injury characteristics, individuals with TBI were more often injured in motor vehicle accidents, spent significantly more days in the ICU, had greater ISS, had higher numbers of injuries and of body regions injured, and had more acute complications while admitted to the trauma center. Non-TBI traumatic injury survivors had significantly more injuries to the lower limbs. Again, these differences were expected given the different nature of the injuries in both groups. Time since injury did not differ significantly among groups. Groups did not differ significantly on the number of co-morbid physical health problems they reported. Self-reports of Depression and Anxiety/Irritability were more frequent in the TBI group but the χ2 comparison did not reach significance. There were, however, significantly more reports of Confusion or Memory loss in the TBI group compared with the non-TBI group.
| Table I. Socio-demographic, injury and health characteristics of the traumatic brain injury (TBI) and Non-TBI groups |
| Variables | TBI (n = 239) | Non-TBI (n = 166) |
| Socio-demographic characteristics | | |
| Age, years, mean (SD) | 37.4 (14.5) | 46.4 (14.5)* |
| Sex, n (%) | | |
| Female | 84 (35.1) | 64 (39.0) |
| Male | 155 (64.9) | 100 (61.0) |
| Marital status, n (%) | | |
| Married/Living with spouse | 126 (53.2) | 92 (56.1) |
| Single/Divorced/Separated/Widowed | 111 (46.8) | 72 (43.9) |
| Education (years completed) , n (%) | | |
| 1–7 | 17 (7.2) | 19 (11.5) |
| 8–12 | 123 (51.9) | 81 (49.1) |
| 13–15 | 59 (24.9) | 36 (21.8) |
| More than 16 | 38 (16.0) | 29 (17.6) |
| Occupation at the time of interview, n (%) | | |
| Working/Studying/Home maker | 92 (38.8) | 59 (35.5) |
| Retired | 25 (10.5) | 48 (28.9)* |
| On disability leave | 120 (50.6) | 59 (35.5)* |
| Social support index, mean (SD) | 79.3 (16.9) | 77.1 (20.1) |
| Injury characteristics | | |
| Cause of injuries, n (%) | | |
| Motor vehicle crash | 201 (84.1) | 108 (65.9)* |
| Falls | 26 (10.9) | 48 (29.3)* |
| Other | 12 (5.0) | 8 (4.8) |
| Injury types, n (%) | | |
| Injury to the spine | 81 (33.9) | 67 (40.4) |
| Upper-limb injury | 94 (39.3) | 55 (33.5) |
| Lower-limb injury | 145 (60.7) | 146 (89.0)* |
| Time since injury, years, mean (SD) | 3.3 (0.7) | 3.3 (0.8) |
| Hospital stay, mean (SD) | | |
| Number of days in ICU | 10.3 (14.3) | 4.2 (8.2)* |
| Acute length of stay (days) | 30.0 (20.9) | 28.2 (18.6) |
| Injury severity, mean (SD) | | |
| Glasgow Coma Score at ER arrival | 9.9 (4.5) | 14.6 (1.4)* |
| Index of Severity Score | 27.9 (9.1) | 15.7 (8.4)* |
| Number of body regions injured | 3.4 (1.36) | 2.3 (1.20)* |
| Number of acute complications | 2.0 (2.7) | 1.4 (2.3)* |
| Total number of injuries | 10.1 (4.9) | 5.5 (3.9)* |
| Pain rating, mean (SD) | 2.4 (1.1) | 2.8 (1.20)* |
| Health characteristics | | |
| Number of co-morbid physical health problems, mean (SD) | 3.4 (2.1) | 3.3 (2.10) |
| Reporting depression, n (%) | 43 (18) | 23 (13.8) |
| Reporting significant anxiety or irritability, n (%) | 50 (21.1) | 23 (13.8) |
| Reporting confusion or memory loss, n (%) | 51 (21.6) | 11 (6.7)* |
| *p < 0.001 for independent t-tests or p < 0.05 χ2 tests compared with the TBI group. Note: Sample sizes may reflect missing data on certain variables. SD: standard deviation; ICU: intensive care unit; ER: emergency room. |
Perceived mental health status in TBI and non-TBI groups
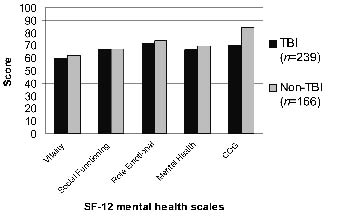
Fig. 1 presents mean scores for the SF-12 mental health scales in the TBI and non-TBI groups. Scores on the Vitality, Social Functioning, Role-Emotional and Mental Health scales were not significantly different in TBI and non-TBI participants. However, both groups scored lower than a normative sample evaluated recently on the SF-12 in a population-based study on insomnia conducted in Quebec recently also using the second version of the SF-12 (33). On the COG scale, TBI participants reported having significantly more problems at the cognitive level than traumatic injury survivors without TBI (p < 0.001).
Fig. 1. Mean 12-item short form (SF-12) mental health scores and cognitive scale (COG) in traumatic brain injury (TBI) and Non-TBI participants.
Factors associated with low mental health
Complete data was available for 397 participants (98% of all available cases) to perform the logistic regression analysis on the global sample (both groups confounded). A comparison of the full to a constant-only model indicated that the model was statistically valid (χ2 (11, n = 397) = 105.13, p < 0.001). A moderate fit was observed between obtained and predicted data (pseudo-R2 Nagelkerke = 0.38). Table II presents the regression coefficients, odd ratios and confidence intervals for each variable considered in the logistic regression analysis. Six variables were found to be significantly associated with low mental health: younger age, being a woman, a shorter time since the injury, a higher pain rating, a lower social support score, and the presence of cognitive problems.
| Table II. Variables associated with low mental health (below 25th percentile of US general population norm) for the entire sample (n = 397) |
| Variables | B | Odds ratio | p | 95% confidence interval |
| Cognitive problems | 1.76 | 5.81* | 0.00 | 2.81–12.01 |
| Social support | –0.04 | 0.96* | 0.00 | 0.95–0.98 |
| Pain rating | 0.36 | 1.43* | 0.01 | 1.07–1.90 |
| Age | –0.03 | 0.97* | 0.01 | 0.94–0.99 |
| Gender | –0.78 | 0.46* | 0.02 | 0.24–0.89 |
| Time since injury | –0.48 | 0.62* | 0.04 | 0.40–0.98 |
| Marital status | 0.47 | 1.60 | 0.15 | 0.85–3.00 |
| Injury Severity Score | 0.004 | 1.00 | 0.83 | 0.97–1.04 |
| Education | 0.10 | 1.10 | 0.61 | 0.75–1.62 |
| Occupation | –0.11 | 0.89 | 0.74 | 0.46–1.73 |
| Physical health problems | 0.02 | 1.02 | 0.82 | 0.86–1.21 |
| Constant | 2.00 | 7.34 | 0.22 | |
| *p < 0.05 |
Note that the interpretation of the odds ratios varies according to the range of units possible for each scale. For example, for each increase of one year of age, the odds of being in the low mental health category decreases by 3% (for each increase in 10 years of age, the odds decrease by 26%). For each increase of 1 unit on the pain rating (ranging from 1 to 5), the odds of being in the low mental health category increases by 43%. For each increase of 1 unit on the social support scale (ranging from 9 to 100), the odds of being in the low mental health category decreases by 4% (for each increase in 10 units, the odds decrease by 32%). And, finally, when participants report having confusion or memory loss, the odds of being in the low mental health category are multiplied by approximately 6.
In a more exploratory manner, separate logistic analyses were conducted on the TBI and non-TBI groups. Results are presented in Table III. In the TBI groups, a comparison of the full to a constant-only model indicated that the model was statistically valid (χ2 (11, n =236) = 79.23, p < 0.001). A moderate fit was observed between obtained and predicted data (pseudo-R2 Nagelkerke = 0.44). Three variables were found to be significantly associated with lower mental health (p < 0.05) in the TBI group: being a woman, a lower social support score, and the presence of cognitive problems. Age almost reached significance suggesting that younger individuals with TBI were more prone to lower mental health.
| Table III. Variables associated with low mental health for the traumatic brain injury (TBI) (n = 235) and Non-TBI (n = 162) groups separately (complete data was available for 397 participants) |
| Variables | TBI | Non-TBI |
| Odds ratio | p | 95% confidence interval | Odds ratio | p | 95% confidence interval |
| Cognitive problems | 5.74* | 0.00 | 2.41–13.67 | 2.90 | 0.22 | 0.52–16.04 |
| Social support | 0.94* | 0.00 | 0.92–0.97 | 0.98 | 0.16 | 0.95–1.01 |
| Pain rating | 1.33 | 0.15 | 0.90–1.97 | 1.90* | 0.03 | 1.08–3.34 |
| Time since injury | 0.61 | 0.09 | 0.35–1.08 | 0.45 | 0.06 | 0.20–1.03 |
| Gender | 0.42* | 0.04 | 0.18–0.98 | 0.54 | 0.29 | 0.17–1.72 |
| Age | 0.97 | 0.07 | 0.94–1.00 | 0.96 | 0.08 | 0.91–1.00 |
| Marital status | 1.37 | 0.44 | 0.62–3.02 | 1.84 | 0.31 | 0.57–5.88 |
| Injury Severity Score | 0.99 | 0.74 | 0.95–1.04 | 0.97 | 0.41 | 0.90–1.05 |
| Education | 1.32 | 0.27 | 0.81–2.15 | 0.72 | 0.38 | 0.35–1.50 |
| Occupation | 0.80 | 0.61 | 0.34–1.88 | 1.03 | 0.96 | 0.31–3.44 |
| Physical health problems | 0.99 | 0.91 | 0.79–1.23 | 1.11 | 0.55 | 0.79–1.55 |
| Constant | 76.22 | 0.06 | | 8.13 | 0.48 | |
| *p < 0.05. |
For the non-TBI group, the model was also statistically valid (χ2 (11, n = 162) = 34.36, p < 0.001). A moderate fit was observed between obtained and predicted data (pseudo-R2 Nagelkerke = 0.36). For this group, only pain was found to be significantly related to lower mental health. Age and Time Since Injury almost reached significance.
Perceived needs for mental health services
Perceived needs for mental health services and perceived access limitations to these services are presented in Table IV. Participants with TBI reported more needs for all types of mental health services in comparison with the non-TBI group, but proportionally to these needs, more individuals in the non-TBI group reported access limitations to all types of mental health services. For the TBI group, services most needed (in decreasing order of importance) were psychotherapy, cognitive rehabilitation, and counseling for work or school. For the non-TBI group, services most needed were psychotherapy and counseling for work or school.
| Table IV. Perceived needs and access limitations for mental health services in the traumatic brain injury (TBI) (n = 239) and Non-TBI (n = 166) groups |
| Type of service | TBI n (%) | Non-TBI n (%) |
| Psychotherapy Perceived need Access limitation | 153 (64.0) 50 (32.7) | 74 (44.6) 34 (46) |
| Family/Couple therapy Perceived need Access limitation | 70 (29.3) 27 (38.6) | 31 (18.7) 17 (54.8) |
| Cognitive rehabilitation Perceived need Access limitation | 148 (61.9) 38 (25.7) | 29 (17.5) 13 (44.8) |
| Communication therapy Perceived need Access limitation | 68 (28.5) 10 (14.7) | 4 (2.4) 1(25.0) |
| Special education services Perceived need Access limitation | 66 (27.6) 10 (15.2) | 12 (7.2) 3 (25.0) |
| Work/School counseling services Perceived need Access limitation | 102 (42.7) 20 (19.6) | 60 (36.1) 20 (33.3) |
DISCUSSION
The present study aimed to describe and compare the subjective mental health status of individuals having sustained trauma, with or without injury to the brain, to explore the correlates of poorer mental health, and to describe these populations’ needs and access to mental health services. Our results revealed that various dimensions of functioning (e.g. vitality, social functioning, roles) are affected by mental health issues following trauma, and that reports of mental problems are frequent whether there is presence of brain injury or not. The presence of psychological distress following TBI has already been well documented in previous studies. However, studies comparing TBI and non-TBI survivors are rare. In the present study, TBI participants presented scores slightly below their non-TBI trauma counterparts on the mental health SF-12 scale scores, but these differences were negligible, except for the COG scale (Fig. 1). Cognitive deficits, which are more specific to TBI, may bring about additional stress and challenges for traumatic injury survivors, which probably explains the supplementary (yet not significantly larger) psychological burden observed on the mental health scales in the brain injury group.
The second objective of this study was to identify factors associated with lower mental health status following trauma with or without brain injury. Six variables were found to be significantly related to lower mental health in the global sample: age, gender, time since injury, social support, pain, and cognitive problems. In a study of adults with TBI only, McCarthy et al. (11) found similar factors associated with lower psychosocial health: younger age, female sex, Medicaid coverage, no health insurance, inadequate social support, co-morbidities, cognitive complaints, and limitations in activities of daily living.
Our results concur with those of previous studies indicating that women report more psychological distress than men after road traffic accidents and injuries (8, 9, 34), and that younger age is associated with worse psychological functioning following TBI (11) or orthopedic trauma (4, 35). The impact of trauma may be more psychologically challenging for younger individuals trying to establish their professional and personal lives. A shorter time since the injury was associated with lower SF-12 Mental Component Scores, suggesting that the impacts of mental health on quality of life tend to lessen as years go by after the accident. This is an encouraging result, yet, it remains that depression and anxiety are still reported up to 5 years after the injury (10).
Available social support is positively associated with measures of health and psychological well-being following trauma (4, 11). McCarthy and colleagues (4) also found that limited social support was linked to psychological distress in a group of trauma survivors with severe lower-limb injuries. It is well established that social support, particularly perceived support, has a protective effect against the development of depression. Individuals who have poor social support should be more closely monitored by their healthcare professionals. Some authors have suggested that social support may be particularly vulnerable following brain injury (36) because of changes in personality or behavior disturbances (apathy, lack of initiative, disinhibition). Although we found no significant difference between the TBI and non-TBI groups in terms of social support (Table I), our regression analyses in separate groups do suggest that low social support seems to be more strongly linked to low mental health individuals with TBI (Table III).
Pain was also found to be linked to poor mental health following trauma. The link between pain and depression in individuals with disabilities is well established in the literature. In our sample, pain was significantly greater in non-TBI trauma patients and seemed to be more strongly related to lower mental health in this group (Table III).
The severity of injuries is not strongly associated with perceived general health and quality of life (37). It is not considered a reliable a predictor of long-term psychological outcome after a traumatic injury (1). Some studies in patients with TBI populations have even shown an inverse relationship between injury severity and psychological problems such as depression, anxiety or insomnia (1, 38). Anosognosia (i.e. lack of awareness of deficits) in more severe TBI is thought to have a protective role against the development of important distress about their condition (39). These data suggest that mental health is not merely a function of physical integrity or recovery following trauma, but that multiple factors may affect psychological outcome. In the same vein, the presence of co-morbid physical health problems was not related to lower mental health either.
The last, but very important, objective of this study was to describe needs and access to services related to mental health following trauma either with or without brain injury. Individuals in both the TBI and non-TBI groups reported in large proportions having needs for services related to mental health (Table IV). As expected, services more specifically oriented towards cognitive sequelae, such as cognitive rehabilitation, communication therapy (speech therapy), and needs for special education, were much more endorsed by traumatic injury survivors having suffered brain injury. Needs for psychotherapy, family/couple therapy, and counseling services in the context of return to school or work were important in both groups however. Thus, whether the brain is involved or not, trauma has consequences that can require attention from mental health professionals.
Important proportions of individuals reported having difficulty obtaining services related to mental health (Table III). Several factors may explain this discouraging situation. First, injured persons themselves or healthcare professionals might not be able to identify mental health problems and to point to adequate resources. Secondly, taboos or beliefs that mental health problems will resorb on their own can hinder patients’ motivation to consult or to mention these to others, thereby preventing themselves from obtaining potential support. Thirdly, healthcare might still not be well organized for dissemination of mental health interventions. In the Quebec rehabilitation care system, mental health services are generally covered by a public insurance program during inpatient rehabilitation. Once patients are discharged from rehabilitation however, geographical or financial barriers to treatment may appear. The results of the larger epidemiological survey indicate that in- and out-patient rehabilitation services targeting physical impairments are reported to be more accessible than those targeting mental health issues (25). Further research should uncover why services related to mental health are so difficult to obtain and whether the lack of services or the presence of barriers to obtain services may in fact worsen psychological difficulties for some individuals.
Particular efforts should be made to help multiple traumatic injury survivors without TBI have better access to mental health services because they systematically report poorer accessibility to mental healthcare (Table III). Rehabilitation systems for brain injury patients have more experience with mental health issues: patients are usually evaluated by a neuropsychologist and attention is paid to symptoms such as depressed mood or anxious reactions. Health professionals working with non-TBI trauma patients, however, need perhaps be sensitized to the presence and potential impacts of mental health issues in their patients. Indeed, there is now a growing literature indicating that problems with depression and anxiety (including symptoms of post-traumatic stress), for example, are very frequent up to 6 weeks post-trauma (5–7), resorb in part by 6 months (3, 6–8) but then persist in proportions varying from 6% to 30% up to 5 years post-trauma, according to different studies (3, 8–10). Screening for psychological problems is perhaps not yet systematically part of routine care protocols for trauma patients without TBI. A short series of validated questionnaires (e.g. Beck depression and anxiety inventories, Psychiatric Symptom Index, or Hospital Anxiety and Depression Scale) or a short clinical interview could help identify traumatic injury survivors in need of more thorough evaluation or treatment.
The main strength of the present study is that it was carried out among a population-based sample of severe traumatic injury survivors requiring rehabilitation. To our knowledge, it also represents the first effort to document needs and access to mental health services in a non-TBI trauma population. Several limitations of this study must be noted however. Patients who were too severely physically or cognitively impaired to consent or answer survey questions by themselves were excluded from the analyses. Furthermore, despite an excellent response rate (67%), we must take into account that non-responders may represent a group of individuals for whom mental health issues may be important. Indeed Corrigan and colleagues (40) showed that TBI survivors who are most likely to be lost to follow-up in studies are usually disadvantaged socio-economically, have higher rates of history of substance abuse, and have more frequently injuries of violent etiology, factors which are all correlated with lower mental health. There is thus a possibility that this bias may have led to an underestimation of mental health problems. Furthermore, we cannot be entirely sure that some participants classified in the non-TBI group did not suffer from undiagnosed minor (concussions) or mild brain injury, although if so, this proportion is most probably quite small because all persons with any alteration of consciousness were classified in the TBI group. Another weakness is that we could not evaluate the proportion of participants who had low mental health prior to the accident. The most important limitation of this study is that it is based on self-reported retrospective data, with the individual biases these methods imply (e.g. errors due to memory, social desirability, exaggerated reports). Participants with cognitive deficits or impairment of awareness may thus have either under- or over-estimated their difficulties or needs. Furthermore, because it was based in the context of a large-scale epidemiological survey, this study relied only on the person’s general perception of his or her mental health. A more complete and precise portrait of different psychopathologies would have been possible only with the use of diagnostic clinical interviews and clinically valid questionnaires. Nonetheless, individual perceptions of mental health convey important information as to the subjective state and level of distress felt by traumatic injury survivors. It is our opinion that paying attention to this subjective distress should be part of the outcome evaluation process following trauma. Finally, one must remember that the results are limited to the Quebec population and that rehabilitation systems may vary greatly between and within countries.
Despite these limitations, which should be taken into consideration in future studies, this study suggests that mental health issues probably remain neglected in trauma care systems. There is now ample literature supporting the diagnostic validity of short interviews or scales to at least identify individuals who are suffering from significant distress and who need further evaluation and care. Trauma care systems have made tremendous advances in lowering mortality. However, advances in medical procedures to improve physical health have not yet been followed by advances in the mental health realm. The next step is now to adapt systems to surviving victims who return to their communities with psychological sequelae of their injuries. Addressing needs related to mental health may prevent chronic difficulties, thereby lowering morbidity, enhancing quality of life and return to productivity, and lowering the social costs of trauma.
ACKNOWLEDGEMENTS
Preparation of this article was supported by the Canadian Institutes for Health Research (CIHR, grants no. MOP-62873), by the Fonds de la Recherche en Santé du Québec (FRSQ, grant no. 3255), and by a scholarship awarded to the first author by the Fondation de l’Hôpital de l’Enfant-Jésus.
REFERENCES
1. Dikmen SS, Bombardier CH, Machamer JE, Fann JR, Temkin NR. Natural history of depression in traumatic brain injury. Arch Phys Med Rehabil 2004; 85: 1457–1464.
2. Ham OK. Psychosocial factors associated with lifetime experience of serious unintentional injury in South Korea. Public Health Nurs 2008; 25: 37–45.
3. O’Donnell ML, Creamer M, Pattison P. Posttraumatic stress disorder and depression following trauma: understanding comorbidity. Am J Psychiatry 2004; 161: 1390–1396.
4. McCarthy ML, MacKenzie EJ, Edwin D, Bosse MJ, Castillo RC, Starr A. Psychological distress associated with severe lower-limb injury. J Bone Joint Surg Am 2003; 85-A: 1689–1697.
5. Wang CH, Tsay SL, Bond AE. Post-traumatic stress disorder, depression, anxiety and quality of life in patients with traffic-related injuries. J Adv Nurs 2005; 52: 22–30.
6. Shepherd JP, Qureshi R, Preston MS, Levers BG. Psychological distress after assaults and accidents. BMJ 1990; 301: 849–850.
7. Mason S, Wardrope J, Turpin G, Rowlands A. The psychological burden of injury: an 18 month prospective cohort study. Emerg Med J 2002; 19: 400–404.
8. Mayou R, Bryant B, Ehlers A. Prediction of psychological outcomes one year after a motor vehicle accident. Am J Psychiatry 2001; 158: 1231–1238.
9. Andersson AL, Bunketorp O, Allebeck P. High rates of psychosocial complications after road traffic injuries. Injury 1997; 28: 539–543.
10. Piccinelli M, Patterson M, Braithwaite I, Boot D, Wilkinson G. Anxiety and depression disorders 5 years after severe injuries: a prospective follow-up study. J Psychosom Res 1999; 46: 455–464.
11. McCarthy ML, Dikmen SS, Langlois JA, Selassie AW, Gu JK, Horner MD. Self-reported psychosocial health among adults with traumatic brain injury. Arch Phys Med Rehabil 2006; 87: 953–961.
12. Hibbard MR, Ashman TA, Spielman LA, Chun D, Charatz HJ, Melvin S. Relationship between depression and psychological functioning after traumatic brain injury. Arch Phys Med Rehabil 2004; 85: S43–S53.
13. Kreutzer JS, Rosenthal M, Hammond FM, Corrigan JD, Black K. Depression after traumatic brain injury: a comprehensive examination. Brain Inj 2003; 15: 563–576.
14. Kreutzer JS, Seel RT, Gourley E. The prevalence and symptom rates of depression after traumatic brain injury: a comprehensive examination. Brain Inj 2001; 15: 563–576.
15. Pagulayan K, Temkin N, Machamer J, Dikmen S. A longitudinal study of health-related quality of life after traumatic brain injury. Arch Phys Med Rehabil 2006; 87: 611–618.
16. Seel RT, Kreutzer JS, Rosenthal M, Hammond FM, Corrigan JD, Black K. Depression after traumatic brain injury: a National Institute on Disability and Rehabilitation Research Model Systems multicenter investigation. Arch Phys Med Rehabil 2003; 84: 177–184.
17. Curran CA, Ponsford JL, Crowe S. Coping strategies and emotional outcome following traumatic brain injury: a comparison with orthopedic patients. J Head Trauma Rehabil 2000; 15: 1256–1274.
18. Frénisy M, Bénony H, Chahraoui K, Minot D, d’Athis P, Pinoit J, et al. Brain injured patients versus multiple trauma patients: some neurobehavioral and psychopathological aspects. J Trauma 2006; 60: 1018–1026.
19. Hanks RA, Temkin N, Machamer J, Dikmen SS. Emotional and behavioral adjustment after traumatic brain injury. Arch Phys Med Rehabil 1999; 80: 991–997.
20. Corrigan J, Whiteneck G, Mellik D. Perceived needs following traumatic brain injury. J Head Trauma Rehabil 2004; 19: 205–216.
21. Heinemann A, Sokol K, Garvin L, Bode R. Measuring unmet needs and services among persons with traumatic brain injury. Arch Phys Med Rehabil 2002; 83: 1052–1059.
22. Pickelsimer EE, Selassie AW, Sample PL, Heinemann AW, Gu JK, Veldheer LC. Unmet service needs of persons with traumatic brain injury. J Head Trauma Rehabil 2007; 22: 1–13.
23. Sirois MJ, Lavoie A, Dionne CE. Predicting discharge of trauma survivors to rehabilitation: a sampling frame solution for a population-based trauma-rehabilitation survey. Am J Phys Med Rehabil 2007; 86: 563–573.
24. American Association for the Advancement of Automotive Medicine. The Abbreviated Injury Scale. Des Plaines, IL: American Association for the Advancement of Automotive Medicine; 1990.
25. Sirois M, Lavoie A, Dionne C. Metropolitan-rural differences in rehabilitation needs, rehabilitation access and physical health outcomes among trauma survivors. Am J Phys Med Rehabil, in press.
26. Ware J, Kosinski M, Turner-Bowker D, Gandek B. How to score version 2 of the SF-12 Health Survey (with a supplement documenting version 1). Lincoln, RI: QualiMetric Incorporated; 2002.
27. Ware JE Jr, Keller SD, Gandek B, Brazier JE, Sullivan M. Evaluating translations of health status questionnaires. Methods from the IQOLA project. International Quality of Life Assessment. Int J Technol Assess Health Care 1995; 11: 525–551.
28. Findler M, Cantor J, Haddad L, Gordon W, Ashman T. The reliability and validity of the SF-36 health survey questionnaire for use with individuals with traumatic brain injury. Brain Inj 2001; 15: 715–723.
29. MacKenzie E, McCarthy M, Ditunno J. Using the SF-36 for characterizing outcome after mutiple trauma involving head injury. J Trauma 2002; 52: 527–534.
30. Daveluy C, Pica L, Audet N, Courtemanche R, Lapointe F, Côté L et al., editors. Enquête sociale et de santé 1998-Cahier technique et méthodologique: documentation générale. Montréal: Institut de la statistique du Québec; 2001.
31. Levasseur M, Goulet L, editors. Les problèmes de santé. Montréal: Institut de la statistique du Québec; 2001.
32. Tabachnik BG, Fidell LS, editors. Using multivariate statistics. 3rd edn. New York: Harper Collins College Publishers; 1996.
33. Leblanc M, Beaulieu-Bonneau S, Merette C, Savard J, Ivers H, Morin CM. Psychological and health-related quality of life factors associated with insomnia in a population-based sample. J Psychosom Res 2007; 63: 157–166.
34. Holbrook T, Hoyt D, Anderson J. The importance of gender on outcome after major trauma: functional and psychological outcomes in women versus men. J Trauma 2001; 50: 270–273.
35. Richmond TS, Kauder D. Predictors of psychological distress following serious injury. J Trauma Stress 2000; 13: 681–692.
36. Rosenthal M, Christensen BK, Ross TP. Depression following traumatic brain injury. Arch Phys Med Rehabil 1998; 79: 90–103.
37. Witheneck G, Gerhart K, Cusick C. Identifying environment factors that influence the outcomes of people with traumatic brain injury. J Head Trauma Rehabil 2004; 19: 191–204.
38. Dickmen SS, Bombardier CH, Machamer JE, Fan JR, Tempkin NR. Natural history of depression in traumatic brain injury. Arch Phys Med Rehabil 2004; 85: 1457–1464.
39. Wallace CA, Bogner J. Awareness of deficits: emotional implications for persons with brain injury and their significant others. Brain Inj 2000; 14: 549–562.
40. Corrigan JD, Harrison-Felix C, Bogner J, Dijkers M, Terrill MS, Whiteneck G. Systematic bias in traumatic brain injury outcome studies because of loss to follow-up. Arch Phys Med Rehabil 2003; 84: 153–160.