OBJECTIVE: The aim of this study was to analyse the efficacy of multidisciplinary interventions on return to work for people on sick leave due to low back pain.
METHODS: A systematic review of published studies was performed, including a meta-analysis. Identified publications were assessed for relevance and study quality.
RESULTS: A meta-analysis based on 5 studies from Scandinavia verified the scientific evidence for the efficacy of multidisciplinary interventions on return to work.
CONCLUSION: Although long-term sick leave due to low back pain represents a large problem for the community and multidisciplinary interventions are often advocated, surprisingly few published studies have return to work as an outcome. There is evidence for a clinically relevant effect of multidisciplinary interventions on return to work.
Key words: sick leave, return to work, rehabilitation, low back pain, multidisciplinary interventions.
J Rehabil Med 2009; 41: 115–121
Correspondence address: Anders Norlund, SBU, PO Box 5650, SE-114 86 Stockholm, Sweden. E-mail: norlund@sbu.se
Submitted March 27, 2008; accepted September 4, 2008
INTRODUCTION
Back, neck and shoulder disorders are the main reasons for long-term sick leave (1) and thereby generate high costs for the community due to loss of productivity. Different rehabilitation measures are used to promote return to work (RTW). Studies of rehabilitation have used RTW, or days of sick leave following intervention, as an outcome, although other measures are possible (2). RTW of a person on sick leave after an intervention of rehabilitation indicates that working capacity has been re-established. In the past few decades, multidisciplinary interventions have been proposed to enhance RTW, but the results have been conflicting. A descriptive study of outcome of vocational rehabilitation managed by 6 local insurance offices in a Swedish county showed positive effects on RTW of 23–57% (3). Thus, scientific evidence for the effect of multidisciplinary interventions on RTW of people with low back pain is needed.
The Swedish Council on Technology Assessment in Health Care (SBU) published a systematic literature review in 2000 entitled Neck Pain, Back Pain (4) based on an assessment of relevance and study quality. The conclusion concerning multidisciplinary interventions was that such treatment was of value for people with chronic low back pain, but that there was no evidence for outcome defined as RTW. The review includes studies published up to May 1998. Thus, whether more recent studies can provide evidence for the efficacy of multidisciplinary interventions needs to be investigated.
The aim of the present study was to analyse the efficacy of multidisciplinary interventions on RTW for people on sick leave due to sub-acute and chronic low back pain lasting more than 4 weeks by means of a systematic literature review supplemented by a meta-analysis.
METHODS
A systematic review was based on a search of literature in PubMed, including studies published as of April 1998, i.e. following the search for literature included in the SBU report (4). Only randomized controlled trials (RCTs) or controlled clinical trials were included. The MeSH terms “Back pain AND (rehabilitation OR return to work OR sick leave OR work injury OR disability pension)” combined with the limitations “April 1998 – December 2006, RCT, English, Adults age 19–64” identified 187 studies. The definition of multidisciplinary interventions included studies involving 2 or more healthcare disciplines. Outcome was RTW measured either directly or indirectly as days of sick leave after start of rehabilitation, with the opportunity to turn sick leave into RTW. Studies were included if low back pain lasted 5–11 weeks (sub-acute) or 12 weeks or more (chronic) according to SBU (2000) (4). Studies involving people with low back pain caused by specific pathologies or conditions were excluded. Studies were excluded if the drop-out rate was more than 30%. Studies that appeared to be relevant were assessed for scientific quality by means of a standard checklist for systematic reviews at SBU. High study quality meant that all quality criteria had been met. All studies with at least limited quality were included. A manual search of studies was based on bibliographies in identified publications. Authors were contacted if the study did not provide sufficient RTW information.
Table I explains the outcome of the literature search, including the reasons for excluding relevant studies.
| Table I. Literature search and excluded relevant studies |
| Literature search |
| The MeSH-terms used were “Back pain AND (rehabilitation OR return to work OR sick leave OR work injury OR disability pension)” combined with the limitations “January 1998–December 2006, RCT, English, Adults 19–64 years”. |
| All identified studies | 187 |
| Not relevant | 171 |
| Relevant but excluded | 10 |
| Included from lists of references | 1 |
| Included in this review | 7 |
| Nine excluded studies | |
| Main author, year | Reason for exclusion |
| Aure, 2003 | Not multidisciplinary intervention |
| Friedrich, 2005 | Drop-out > 30% |
| Greitemann, 2006 | LBP one of several subgroups included |
| Heymans, 2006 | Sick leave, not RTW |
| Kool, 2005 | Sick leave, not RTW |
| Von Korff, 2005 | Sick leave, not RTW |
| Schweikert, 2006 | Drop-out: Trial > 40%, Controls > 30% |
| Soukup, 1999 | Sick leave, not RTW |
| Stenstra, 2006 | Sick leave, not RTW |
| Torstensen, 1998 | Not multidisciplinary intervention |
| RTW: return to work; LBP: low back pain. |
Quantitative analyses used meta-analytic methods based on Cochrane RevMed Version 4.2. Meta-analyses were performed by pooling weighted mean differences with both fixed and random effects models. Data on the number of people with RTW were extracted. Statistical heterogeneity was assessed by means of I2 (Cochrane’s chi-square) statistics and 95% confidence intervals (95% CI) (5). Funnel plots, i.e. plotting of treatment effect vs study size, was used to detect publication bias or systematic heterogeneity (6). In the case of an asymmetric funnel plot the appropriateness of the meta-analysis could be questioned.
RESULTS
Results of the systematic review
Seven studies were included with a total of 1450 patients, 51% of whom were women. A majority of the studies were in Scandinavia. The studies are broken down according to length of sick leave before the start of rehabilitation, i.e. 5–11 weeks or 12 weeks or longer.
Initial sick leave of 5–11 weeks
A multi-centre RCT compared behaviour-oriented physiotherapy, cognitive behavioural therapy, behavioural medicine rehabilitation and a control group (7) (Table II). Interventions lasted 4 weeks, were performed in small groups (4–8) and included a medical examination. The interventions included 6 informational sessions and workplace visits. Supervisors at the workplace were invited to the discharge sessions at which a rehabilitation plan was agreed upon. The control group had no structured involvement by such supervisors. Finally, 6 booster sessions were held over a 12-month period. The outcome was taken from national registers with regard to sick leave and disability pension, as well as from self-reporting of pain and healthcare utilization at 3-month and 6-month intervals. The study showed that multidisciplinary intervention had a significant impact on RTW in women but not men.
| Table II. Included studies on sub-acute and chronic low back pain |
| Author, year, country | Interventions Duration of LBP or Sick leave when LPB | Design, participants, drop-outs, time | Inclusion, exclusion | Outcome measures | Results | Comments | Study quality and relevance |
| Bendix et al. 2000 (11) Denmark | Functional restoration vs outpatient physical training > 3 months | RCT, 59 + 68, women 65% and 66% Drop-outs 11 + 17 1-year follow up | Inclusion: 18–59 years old, on sick leave > 120 days from LBP with or without sciatica Exclusion: osteoporosis, cancer, psychiatric condition, surgically treatable instability. | Work capability | After 12 months 36/48 vs 35/51 had work capability (not significant), but increase in each group | Results per protocol | Limited |
| Hagen et al. 2000 (8) Norway | Early onset of information of prognosis and of importance of physical therapy | RCT, 237 + 220 participants, drop-outs 13 + 5, university clinic (intervention) vs primary care (controls) | Inclusion: age 18–60, on sick leave for LBP 8–12 weeks, no pregnancy, trauma, cancer etc + no ongoing other LBP treatment | Return to work Days of sick leave Societal costs | Return to work year 1, odds ratio 1.60; year 2 difference not significant; year 3 days of sick leave 127.7 versus 169.6 | No sensitivity analysis, costs not patient specific. | Moderately high |
| van den Hout et al. 2003 (9) The Netherlands | Problem solving therapy added to graded physical therapy Controls had group education | Unblinded RCT, 45 + 39 participants, drop-outs 13 + 18 1 year | Inclusion: ages 18–65, LBP > 6 weeks, sick-leave < 20 weeks Exclusion: trauma, pregnancy, non-Dutch speaking, other ongoing rehabilitation, any litigation regarding conflicts | Return to work Days of sick leave due to LBP | No significant difference of outcome measures | Analysis per protocol, unclear randomization, skewed gender distribution | Limited |
| Indahl et al. 1998 (10) Norway | Light mobilization + mini back school vs control | Controlled trial, follow-up after 5 years 245 + 244 (89 + 94 women) | Inclusion: 18–65 years old, sicklisted for sub-chronic LBP, referred to spine clinic Exclusion: pregnant women. | Return to work | After 5 years 81% vs 66% return to work (p < 0.001) No effects on those age 60+ years | Longitudinal follow-up study | Moderately high |
| Jensen et al. 2005 (7) Sweden | PT, CBT, PT + CBT 1–6 months of LBP | RCT multicentre, 214 participants in total, 42% drop-out in controls, 3 years | Inclusion: Non-specific spinal pain sick-listed > 1 < 6 months, fluent in Swedish, 18–60 years Exclusion: Trauma, need for surgery, co-morbidity, ongoing rehabilitation, pregnancy | Days of sick leave, disability pension, pain (SF-36), costs to the community | Combination PT + CBT superior to either PT, CBT or controls. Strongest effect among women | High drop-out rate of controls, but not on register data of sick leave No sensitivity analysis despite skewed cost data | Moderately high |
| Jousset et al. 2004 (13) France | Functional restoration vs physical therapy 3 h weekly > 200 days of sick leave | RCT, 44 + 42 participants in 2 intervention groups, 6 months | Inclusion: Ages 18–50 years, chronic LBP. Exclusion: Disability pension, psychiatric disorders, recent surgery | Self-reported sick leave, return to work, self-estimation of pain and of work capacity | No significant difference for sick leave | Short follow-up, self-reported outcome | Limited |
| Skouen et al. 2002 (12) Norway | Light MDR, extensive treatment as usual | RCT, 95 + 56 participants, drop-outs 4 + 0 | Inclusion: Employees with LBP and sick leave Exclusion: Trauma, malignancy, pregnancy, neurological or cardiovascular diseases | Return to work Relative Risk | Mean number of months at work from end of intervention up to 24 months: Treatment as usual 11.1 months, Light MDR 16.9 months (p < 0.02), Extensive MDR 14.1 months | CI (95%) at 24 months almost 1.0, i.e. uncertainty as regards power of significance | Moderately high |
| LBP: low back pain; RCT: randomized controlled trial; MDR: multi-disciplinary treatment; SF-36: Short-Form 36 questionnaire; CI: confidence interval; PT: physiotherapy; CBT: cognitive behaviour therapy. |
A Norwegian RCT lasting for 3 years, a continuation of a previously published 1-year RCT, examined the effects of light mobilization on long-term sick leave of people with low back pain (8) (Table II). The setting was a university clinic for the intervention group and primary care for the control group (8). The core of the intervention was individualized information provided to each patient concerning prognosis (good) and the importance of staying active (daily walks) in order to avoid muscle dysfunction. Calculations of costs to the community were included but without a sensitivity analysis.
The intervention group had earlier RTW during the first year, after which the differences narrowed and finally disappeared. Thus, the effect of early intervention was achieved during the first year and RTW did not increase the risk of recurrence.
An RCT analysed the supplemental value of problem-solving therapy (PST), when added to behavioural graded activity, with regard to days of sick leave and work status in employees with low back pain (9) (Table II). The intervention for the control group was education. The analysis was performed per protocol. No significant difference was found between outcome expressed as RTW and days of sick leave. A multiple regression analysis showed that baseline differences related to the Roland Disability Questionnaire (measuring functional status for low back pain) alone explained variations in days of sick leave during the first 6 months of follow-up and PST during the subsequent 6–12 months.
A Norwegian controlled study at a spine clinic included 489 consecutive patients, who were alternately assigned to the intervention or control group (10) (Table II). The intervention consisted of a light mobilization programme based on education and advice (mini back school) and monitoring of conventional treatment. Follow-up was 5 years. Based on data from the insurance office, RTW was 81% in the intervention group and 65% in the control group. During the follow-up period, 72% of the intervention group and 74% of the control group had sickness absence due to low back pain. Those who did not RTW reported less self-monitoring of their health, earned lower incomes and had more children than those who returned to work.
Initial sick leave of 12 weeks or longer
A Danish RCT compared functional restoration with outpatient physical training of people with chronic low back pain (11) (Table II). Work capability, which included people working following education, early retirees for non-health-related reasons and unemployed people ready to work, was used as an outcome, thus representing a broader interpretation of RTW. The study suffered from a rather large drop-out rate, and the results were presented as per protocol only. Both groups showed an increase in work capability, but there was no significant difference between them at 1-year follow-up.
A large Norwegian RCT on musculoskeletal pain separately analysed a subgroup of patients with chronic low back pain who were on sick leave for an average of 3 months (12) (Table II). Out of 211 patients, 195 were followed for 24 months. Patients receiving light and extensive multidisciplinary treatment (6 h a day, 5 days a week for 4 weeks) were compared with a control group. There was a significant increase of RTW among men in the light multidisciplinary treatment group compared with the control group (70% vs 50%, p < 0.05) but not among those in the extensive multidisciplinary treatment group. The relative risk of RTW peaked after about 11 months in all groups, i.e. just before the period when Norwegian national health insurance reduces sickness benefits by 40%.
A French RCT with 84 participants with chronic low back pain compared the effects of functional restoration with active individual therapy (13) (Table II). Follow-up lasted for 6 months. Outcomes were measured on the basis of different self-reported estimates, such as scales of pain, well-being and work capacity, as well as sick leave. The results showed no significant difference in days of sick leave or RTW, but the intensity of pain was lower in the functional restoration group than the active individual therapy group.
Meta-analysis
The 7 studies included in the systematic review cover multidisciplinary interventions in the broad sense of the term, i.e. several disciplines of vocational therapy were involved. Because several studies show no significant effect of multidisciplinary interventions on RTW, there is no clear indication as to whether the included studies provide such evidence. A meta-analysis was performed, including 2 studies on multidisciplinary interventions from the SBU report (4) that were assessed as having higher study quality (14, 15) and RTW as an outcome.
The meta-analysis was performed in 2 steps. First, 6 out of the 8 studies with RTW as an outcome were included (except for Skouen et al. (12), which expressed RTW as months of work rather than RTW of individuals), adding the 2 studies from the SBU report (14, 15) and breaking them down according to initial length of sick leave, i.e. 5–11 weeks or 12 weeks or longer, prior to the intervention of rehabilitation. The second step included only studies with a Scandinavian setting, given the similarity of population structures, labour markets, social security systems and unemployment rates, i.e. factors that may have a major influence on RTW.
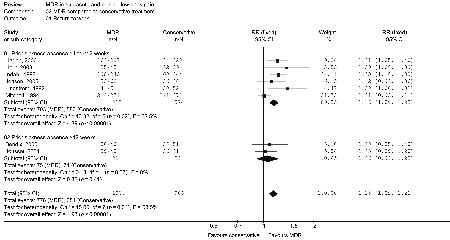
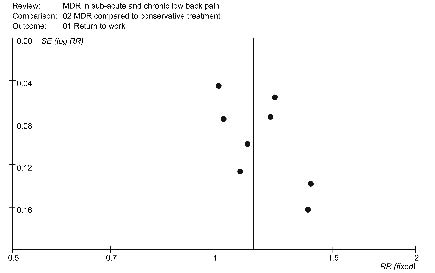
The meta-analysis in Fig. 1 of all studies included in this review shows heterogeneity between them despite a significant difference of effect on RTW (15%, i.e. relative risk (RR) 1.15). A funnel plot (Fig. 2) reveals that publication bias is likely for the included studies (an asymmetric inverted funnel shape indicates the possibility of publication bias). However, studies including individuals on sick leave for 5–11 weeks showed a somewhat larger difference of effect on RTW (16%, i.e. RR 1.16).
Fig. 1. Meta-analysis of all included multidisciplinary intervention studies, grouped according to duration of initial sick leave. Outcome of studies expressed as relative risk (RR) using fixed effect according to the size of each included study. CI: confidence interval; I2: describes the % of variation across studies due to heterogeneity; MDR: multidisciplinary rehabilitation; n: number of patients in the intervention group, and in the control group, respectively; N: all included patients in a study; P: probability; Z: statistics of effect.
Fig. 2. Funnel plot of studies included in Fig. 1. Plot of outcome of included studies expressed as relative risk (RR). MDR: multidisciplinary rehabilitation; SE: standard error.
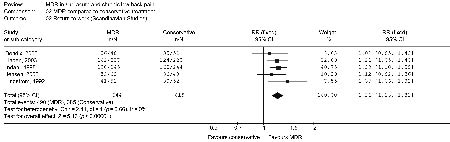
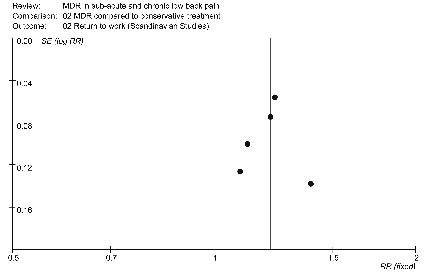
The second meta-analysis (Fig. 3) included Scandinavian studies only. The 5 studies in the second meta-analysis indicate no problem of heterogeneity, while the funnel plot (Fig. 4) reveals no publication bias. The difference of effect is now larger (21%, i.e. RR 1.21, Fig. 3), which is of reasonable clinical relevance.
Fig. 3. Meta-analysis of included multidisciplinary intervention studies from Scandinavia. Outcome of studies expressed as relative risk (RR) using fixed effect. CI: confidence interval; I2: describes the % of variation across studies due to heterogeneity; MDR: multidisciplinary rehabilitation; n: number of patients in the intervention group, and in the control group, respectively; N: all included patients in a study; P: probability; Z: statistics of effect.
Fig. 4. Funnel plot of included studies in Fig. 3. Plot of outcome of included studies expressed as relative risk (RR). MDR: multidisciplinary rehabilitation; SE: standard error..
DISCUSSION
The aim of this systematic review of people with low back pain lasting longer than 4 weeks was to assess whether multidisciplinary programmes more effectively improve RTW than the alternatives. A meta-analysis of all studies indicated a limited effect, combined with possible publication bias, which puts the evidence in question. However, limiting the studies to those conducted in Scandinavia, whose labour markets, social security systems and unemployment rates are similar, increased the differences of effects on RTW to a level of clinical relevance (21%).
Some aspects of this systematic review suggest limitations, the first being publication bias, as described by the funnel plot for Fig. 1. Although not absent from our analysis, publication bias was less relevant when limiting the meta-analysis to Scandinavian studies.
The search strategy was limited to PubMed and studies written in English. However, an analysis of 159 systematic reviews indicates that non-English and non-indexed trials tended to show larger treatment effects (16) than others. It is assumed that a missing study would not significantly change the outcome of the meta-analysis and thereby the conclusions.
One study involved self-reporting of RTW, the outcome on which this systematic review focuses (13), while the remaining studies used other methods. Self-reported data on sick leave have been called into question as being less reliable than register data, especially when covering a longer period of time and reporting several months retrospectively. However, a recently published study shows that self-reported data correlated well with register data (17).
The meta-analysis performed for this review was partly based on studies of higher quality (14, 15) included in the SBU report (4). The meta-analysis of all included studies shows only a limited difference in RTW, as well as the presence of publication bias. This result is somewhat in opposition to the systematic review performed by Meijer et al. (18). Two studies were in agreement with those included in our systematic review, i.e. Mitchell & Carmen (15), included from the SBU report for the meta-analysis, and Skouen et al. (12), whereas only one was in agreement with the meta-analysis (15). A systematic review by Meijer et al. (18), covering January 1990 to December 2004, assessed RCTs on RTW programmes for people on sick leave with non-specific musculoskeletal complaints (18). A total of 21 studies were included, of which 17 were assessed as having high study quality. The majority (68%) showed no significant difference in terms of RTW. However, if the analysis was limited to low back pain, a significant positive effect was found among the 5 included studies, 2 of which concerned functional restoration (15, 19), 2 concerned multidisciplinary team interventions (12, 20) and one concerned cognitive behavioural intervention (21). However, the study by Haldorsen et al. (20) concerned people with musculoskeletal pain in general.
A recently published systematic review concluded that multidisciplinary back training has a positive effect on work participation (22). That conclusion was based on 6 out of 10 included studies that had RTW or work capability as the outcome. Three of them show a significant effect on RTW, of which Skouen et al. (12) was not included in the SBU report (4) but in our systematic review. However, the systematic review by van Geen et al. (22) included no meta-analysis.
Another recently published systematic review on advice as part of managing low back pain was based on 39 RCTs. With regard to chronic low back pain, the conclusion was that “there is strong evidence to support the use of advice to remain active in addition to specific advice relating to most appropriate exercise” (23). A total of 19 studies included patients with sub-acute pain, and 7 included those with chronic low back pain (23). The latter studies had work disability as the outcome, and 5 of them showed significant differences compared with control groups. Three of the 5 studies were included in the SBU report (24–26), one was included in our systematic review (11), though showing no significant difference among the groups in terms of work capability, and one supplemented Mensendiek intervention (27) with advice. However, as Soukup et al. (27) concluded, there was no significant reduction in sick leave, only a trend. That systematic review did not perform a meta-analysis.
The presence of physical de-conditioning, such as loss of cardiovascular capacity, in people with chronic low back pain has been suggested as a reason for their RTW difficulties (28). Smeets et al. (29) investigated the hypothesis but found limited or no evidence. A recently published systematic review on functional restoration programmes found little evidence with regard to RTW (30). The authors concluded that the social security system probably has a larger impact on RTW than functional restoration programmes. Another study on rehabilitation found that caregiver attitudes and personal relationships were more important than the intervention itself (31).
In conclusion, this review of studies conducted in similar Scandinavian settings on people with low back pain who are on sick leave for longer than 4 weeks found evidence that multidisciplinary interventions have a significant effect on RTW.
REFERENCES
1. Bloch FS. Medical proof, social policy, and social security’s medically centered definition of disability. Cornell Law Rev 2007; 92: 189–234.
2. Alexanderson K, Norlund A, editors. Sickness abscence – causes, consequences and physicians’ sickness certification practice. A systematic literature review by the Swedish Council on Technology Assessment in Health Care (SBU). Basingstoke: Taylor & Francis; 2004.
3. Ahlgren A, Bergroth A, Ekholm J. Work resumption or not after rehabilitation? A descriptive study from six social insurance offices. Int J Rehabil Res 2004; 27: 171–180.
4. Nachemson A, Jonsson E, editors. Neck and back pain. The scientific evidence of causes, diagnosis, and treatment. Philadelphia: Lippincott, Williams & Williams; 2000.
5. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med 2002; 21: 1539–1558.
6. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997; 315: 629–634.
7. Jensen IB, Bergström G, Ljungquist T, Bodin L. A 3-year follow-up of a multidisciplinary rehabilitation programme for back and neck pain. Pain 2005; 115: 273–283.
8. Hagen EM, Eriksen HR, Ursin H. Does early intervention with a light mobilization program reduce long-term sick leave for low back pain? Spine 2000; 25: 1973–1976.
9. van den Hout JH, Vlaeyen JW, Heuts PH, Zijlema JH, Wijnen JA. Secondary prevention of work-related disability in nonspecific low back pain: does problem-solving therapy help? A randomized clinical trial. Clin J Pain 2003; 19: 87–96.
10. Indahl A, Haldorsen EH, Holm S, Reikeras O, Ursin H. Five-year follow-up study of a controlled clinical trial using light mobilization and an informative approach to low back pain. Spine 1998; 23: 2625–2630.
11. Bendix T, Bendix A, Labriola M, Haestrup C, Ebbehoj N. Functional restoration versus outpatient physical training in chronic low back pain: a randomized comparative study. Spine 2000; 25: 2494–2500.
12. Skouen JS, Grasdal AL, Haldorsen EM, Ursin H. Relative cost-effectiveness of extensive and light multidisciplinary treatment programs versus treatment as usual for patients with chronic low back pain on long-term sick leave: randomized controlled study. Spine 2002; 27: 901–909; discussion 909–910.
13. Jousset N, Fanello S, Bontoux L, Dubus V, Billabert C, Vielle B, et al. Effects of functional restoration versus 3 hours per week physical therapy: a randomized controlled study. Spine 2004; 29: 487–493; discussion 494.
14. Lindström I, Öhlund C, Eek C, Wallin L, Peterson LE, Nachemson A. Mobility, strength, and fitness after a graded activity program for patients with subacute low back pain. A randomized prospective clinical study with a behavioral therapy approach. Spine 1992; 17: 641–652.
15. Mitchell RI, Carmen GM. The functional restoration approach to the treatment of chronic pain in patients with soft tissue and back injuries. Spine 1994; 19: 633–642.
16. Egger M, Juni P, Bartlett C, Holenstein F, Sterne J. How important are comprehensive literature searches and the assessment of trial quality in systematic reviews? Empirical study. Health Technol Assess 2003; 7: 1–76.
17. Voss M, Stark S, Alfredsson L, Vingard E, Josephson M. Comparisons of self-reported and register data on sickness absence among public employees in Sweden. Occup Environ Med 2008; 65: 61–67.
18. Meijer EM, Sluiter JK, Frings-Dresen MH. Evaluation of effective return-to-work treatment programs for sick-listed patients with non-specific musculoskeletal complaints: a systematic review. Int Arch Occup Environ Health 2005; 78: 523–532.
19. Corey D, Koepfler LE, Etlin D, Day HI. A limited functional restoration program for injured workers: a randomized trial. J Occup Rehabil 1996; 6: 239–249.
20. Haldorsen EM, Grasdal AL, Skouen JS, Risa AE, Kronholm K, Ursin H. Is there a right treatment for a particular patient group? Comparison of ordinary treatment, light multidisciplinary treatment, and extensive multidisciplinary treatment for long-term sick-listed employees with musculoskeletal pain. Pain 2002; 95: 49–63.
21. Marhold C, Linton SJ, Melin L. A cognitive-behavioral return-to-work program: effects on pain patients with a history of long-term versus short-term sick leave. Pain 2001; 91: 155–163.
22. van Geen JW, Edelaar MJ, Janssen M, van Eijk JT. The long-term effect of multidisciplinary back training: a systematic review. Spine 2007; 32: 249–255.
23. Liddle SD, Gracey JH, Baxter GD. Advice for the management of low back pain: a systematic review of randomised controlled trials. Man Ther 2007; 12: 310–327.
24. Bendix AE, Bendix T, Haestrup C, Busch E. A prospective, randomized 5-year follow-up study of functional restoration in chronic low back pain patients. Eur Spine J 1998; 7: 111–119.
25. Bendix AF, Bendix T, Lund C, Kirkbak S, Ostenfeld S. Comparison of three intensive programs for chronic low back pain patients: a prospective, randomized, observer-blinded study with one-year follow-up. Scand J Rehabil Med 1997; 29: 81–89.
26. Bendix AF, Bendix T, Vaegter K, Lund C, Frølund L, Holm L. Multidisciplinary intensive treatment for chronic low back pain: a randomized, prospective study. Cleve Clin J Med 1996; 63: 62–69.
27. Soukup MG, Glomsröd B, Lonn JH, Bo K, Larsen S. The effect of a Mensendieck exercise program as secondary prophylaxis for recurrent low back pain. A randomized, controlled trial with 12-month follow-up. Spine 1999; 24: 1585–1591; discussion 1592.
28. Mayer T, McMahon MJ, Gatchel RJ, Sparks B, Wright A, Pegues P. Socioeconomic outcomes of combined spine surgery and functional restoration in workers’ compensation spinal disorders with matched controls. Spine 1998; 23: 598–605; discussion 606.
29. Smeets RJ, Wade D, Hidding A, Van Leeuwen PJ, Vlaeyen JW, Knottnerus JA. The association of physical deconditioning and chronic low back pain: a hypothesis-oriented systematic review. Disabil Rehabil 2006; 28: 673–693.
30. Poiraudeau S, Rannou F, Revel M. Functional restoration programs for low back pain: a systematic review. Ann Readapt Med Phys 2007; 50: 419–424, 425–429.
31. Östlund GM, Borg KE, Wide P, Hensing GK, Alexanderson KA. Clients’ perceptions of contact with professionals within healthcare and social insurance offices. Scand J Public Health 2003; 31: 275–282.