OBJECTIVE: To evaluate the short-term effects of high-intensity, task-specific vs regular rehabilitation programme on neuromuscular activity and functional changes in elderly inpatients.
DESIGN: Single-blind, randomized controlled trial.
Patients: Sixty-two patients, aged 74.1 (standard deviation (SD) 6.9) years, 12.8 (SD 3.6) days after operation of one lower limb.
METHODS: Allocation to either high- or regular-intensity strength training of non-operated limb, of 3 weeks duration. Outcome measurements: ratio of integrated electromyography per weight lifted (mm vastus medialis and lateralis), isometric electromyography (EMG), maximal weight lifted expressed as 1 repetition maximum, torque in Nm and isometric maximal force of uninvolved leg, timed “up and go“ test (TUG) and Western Ontario and McMaster Universities (WOMAC) questionnaire.
RESULTS: Both programmes resulted in significant improvements in: integrated EMG/weight lifted ratio, isometric EMG, 1 repetition maximum, torque and isometric force, TUG performance and WOMAC items (all p < 0.0001, Wilcoxon signed-rank test). Significant differences were found between the high- and regular-intensity groups for integrated EMG/weight lifted (p = 0.026), 1 repetition maximum and torque (p = 0.0014, Wilcoxon rank-sum test).
CONCLUSION: High-intensity, short-period, early postoperative muscle training has a superior effect on maximal weight lifted by the knee extensors and integrated EMG/weight lifted compared with regular training. These findings are in accordance with more rapid neuronal adaptation by a high-intensity rehabilitation programme.
Key words: elderly, postoperative rehabilitation, strength training, neuromuscular adaptations.
J Rehabil Med 2007; 39: 724–729
Correspondence address: Amir Tal, Berner REHA Zentrum, CH-3625 Heiligenschwendi, Switzerland. E-mail: a.tal@rehabern.ch
Submitted October 26, 2006; accepted June 4, 2007
Introduction
Ageing leads to sarcopenia, but also to a progressive loss in neural control over muscle activity (1). The latter is characterized by a functional and numerical decline in alpha-motor neurones and their regulation at the spinal cord level, i.e. a decrease in the number of alpha-motor neurones, decrease in the Ia (sensory) fibres and decrease in the conduction velocities (1–4). In addition, supraspinal mechanisms are responsible, through the inhibitory descending corticospinal tracts (5), for presynaptic inhibition (6). Collectively, these structural and functional changes result in reduced speed of movement, reaction time and motion control, and eventually to falls and fractures (2, 7, 8).
Fortunately, the neuromuscular system has an excellent ability to adapt to different demands and loss of function is principally reversible (9). Early increase in force following strength training is mainly due to motor learning and not to an increase in muscle mass (9–13). The effectiveness of neuronal control over muscle contractions can be measured by the ratio of motor units recruited per force developed (14–16). Therefore, positive training effects can be visualized by a decrease in electromyographic (EMG) activity for a given test load (1). In addition, early force gain is associated with an increase in motor unit recruitment and firing rates and better synchronization (9, 13, 17, 18). These latter effects can be quantified by the integrated EMG, the maximal isometric and maximal dynamic force, as has been shown by several studies (7, 8, 19–22).
After surgical intervention for fracture or joint replacement, elderly patients may be referred for stationary rehabilitation to improve muscle and joint functions, as well as gait and balance reactions. Due to economic restrictions, such rehabilitation programmes have to start a few days after surgery and the duration of inpatient programmes has to be kept as short as possible (23). However, the evidence for the effectiveness of rehabilitation programmes in the elderly is inconclusive (24, 25). Moreover, intensive muscular training of the operated leg is usually not possible during the early period after surgery.
The objectives of this study were, therefore, to evaluate the neuromuscular changes and the improvement in force and function after 3 weeks of task-specific, high-intensity muscle strength training on the non-operated leg, and to compare the measurements with a regular intensity training, in a cohort of elderly inpatients early after lower limb operation. In addition, we assessed integrative functions using the timed “up and go” (TUG) test and the Western Ontario and McMaster Universities (WOMAC) questionnaire.
Materials and methods
Patients and medical examination
Sixty-two consecutive elderly patients from our musculoskeletal rehabilitation department were recruited for this study. Thirty-four patients were referred after hip operation (8 osteosynthesis and 26 arthroplasty), 25 patients after knee operation (2 osteosynthesis and 23 arthroplasty) and 3 patients after osteosynthesis of a foot. Patients had heterogenic co-morbidities, such as osteoarthritis (OA; n = 46) or osteoporosis (OP; n = 12), and other rheumatic diseases, such as gout, rheumatoid arthritis or fibromyalgia (n = 8). Due to the recent surgical intervention patients were not allowed to exercise the operated limb. All subjects had a baseline medical examination with special focus on clinical signs of (poly-) neuropathy. Prior to training, standard laboratory examination was performed, including albumin, haemoglobin and creatine kinase measurement (Table I). Serum calcium and phosphate levels were normal in all patients.
| Table I. Patient characteristics (mean (SD)) |
| Characteristic | HIG (n = 33) | RIG (n = 29) | p |
| Age (years) | 73.7 (6.0) | 74.6 (7.8) | ns |
| Male/female | 11/22 | 7/22 | ns |
| Body mass index (kg/m²) | 26.8 (5.3) | 25.4 (6.3) | ns |
| No. of trainings | 11.4 (2.8) | 12.2 (3.1) | ns |
| Days after operation | 12.5 (3.6) | 13.3 (5.6) | ns |
| Length of stay (days) | 15.5 (3.7) | 16.6 (4.5) | ns |
| Haemoglobin (g/l) | 11.8 (1.2) | 11.8 (1.0) | ns |
| Creatine kinase (µ/I) | 63.5 (32.7) | 64.6 (38.0) | ns |
| Serum albumin (g/l) | 43.0 (3.8) | 43.2 (4.1) | ns |
| Type of operation | 18 Hip | 16 Hip | |
| | 15 Knee | 10 Knee | |
| | | 3 Foot | |
| HIG: high intensity group; RIG: regular intensity group (control); ns: non-significant; SD: standard deviation. |
Exclusion criteria
Patients with neuromuscular, cardiovascular or other disorders that could influence and/or limit their participation in a tailored strength training programme were excluded. Patients must not have participated in any muscle resistance training during the past 6 months. They must not have been taking medication such as corticosteroids or anabolic drugs, which could affect their physical performance. All subjects were informed about the research aims, test and training procedures and gave their written informed consent. The study protocol was approved by the local ethics committee (Berne).
Study design and randomization
Prospective randomized controlled trial. Within 24–48 hours after admission, patients were randomized to the high-intensity intervention group (HIG) or the regular-intensity group (RIG) serving as “control group”. Both groups performed a standardized rehabilitation programme (mean duration 16 days (standard deviation (SD) 4)) including strength training of the non-operated leg. In addition, the HIG performed a task-specific progressive high-intensity strength training of the non-operated lower limb.
Patients were randomized by an independent person at the hospital. The randomization process was computer-generated and concealed in sealed, sequentially numbered envelopes. These envelopes were opened only after a patient had definitely been enrolled in the study. A total of 33 patients were allocated to the HIG and 29 to the RIG.
Assessments were carried out within 48 h after admission and 24 h before leaving. Measurements of the non-operated limb were performed by a physiotherapist who was unaware of the treatment allocation (assessor blinding). Care was taken to repeat measurements at the identical time of day and at the same temperature (26). Training was supervised by an experienced physiotherapist.
Outcome measurements
Primary parameter. The ratio (26, 27) of the integrated EMG per weight lifted was used as a measure of the effectiveness of the neuronal control (µV*s/kg). The integrated EMG is the mathematical integral of the area under the curve (Fig. 1) and weight lifted is the 80% of 1RM pre-training,
Fig. 1. An example of electromyographic (EMG) measurements during dynamic contractions of the left side. The upper part shows the EMG of m. vastus medialis and the lower part of m. vastus lateralis. The left side demonstrates 1 set of 7 repetitions: Y axis shows the units in (microvolts) μV and the X axis the time of one set (in sec). On the right side a demonstration of averaged 3 sets: in the first column an average of the integrated EMG (area under the curve) in μV*s. The middle column demonstrates the peak values in μV. The third column presents the input of each muscle for the total work in %.
Secondary parameter. The measured EMG peaks of 3 consecutive maximal isometric contractions during 6 sec each were averaged and expressed as “isometric EMG” in µV.
Additional parameters: Maximal weight lifted (expressed as 1RM in kg), maximal concentric contractions expressed as torque in Newton metre (Nm) and maximal isometric force (mean of 3 consecutive measurements, in Newton) measured muscle function.
The WOMAC questionnaire was applied to measure subjective perception of pain, stiffness and activities of daily living (28; expressed in %).
The TUG test (29; expressed in sec) was applied to measure the time a patient needs to rise from a chair, walk 3 m, and return to sit on the chair. This parameter gives an idea of the minimal mobility of the patient.
The test-retest reliability of the integrated EMG, isometric EMG, 1RM and isometric force measurements were analysed by applying the intraclass correlation coefficient (ICC) using SPSS software version 14. In these reliability (test-retest) measurements we performed the exact same procedure as in the real study, including placing the electrodes, marking the place, testing EMG, removing them and placing them again for a retest. The ICC gave an excellent correlation between test and retest for all measurements (95% confidence interval (CI) for a one-way random effect model, α = 0.99).
Testing regime
Measurements of EMG, 1RM torque and isometric force were performed on the non-operated limb only. According to Alkner et al. (30) surface EMG recordings from m. vastus lateralis (VL) are the most reliable in predicting force output. Mizner et al. (31) claim that quadriceps strength plays a dominant role in predicting different functional outcome.
Measurements of surface EMG were performed according to Noraxon and Surface ElectroMyoGraphy for the Non-Invasive Assessment of Muscles (SENIAM) protocols (32, 33). For m. vastus medialis (VM), electrodes were placed at around 80% on the line between anterior spina iliaca superior and the joint space in front of the anterior border of the medial ligament. For the VL, electrodes were placed at 2/3 on the line from the anterior spina iliaca superior to the lateral side of the patella. The skin over the selected areas of VM and VL was palpated, shaved, cleaned with “Every – Abrasive skin cleaning paste” and washed with isopropanol 100%.
Two single-use surface electrodes (Noraxon Dual Electrode, 272, Noraxon USA, Inc., Arizona, USA) were placed longitudinally on these muscles. One ground electrode (Noraxon Single Electrode, 270, Noraxon USA, Inc.) was placed on the patella. The location of the electrodes was marked with a permanent marker in order to be reproducible for the second measurement.
EMG data were collected during a maximal isometric contraction and during a dynamic 80% of 1RM effort, using the “MyoTrace Plus, Isolated A/D system” and MyoTrace 200 Handheld EMG device. Data were sent real-time to the computer via the USB port and recorded and analysed by Myoresearch XP 1.04.02 Master Edition software (Noraxon USA, Inc., Scottsdale, AZ). The data source was: smoothed/rectified root mean square (RMS) EMG (in µV*s).
Maximal isometric force testing was performed unilaterally on the Leg-Press-Functional instrument “CTT-BMC” and computer-supported Biofeedback motor control software (BfMC GmbH, Leipzig, Germany).
The operated leg was laid and fixed in a sliding cast (developed for this study by Proxomed Medizintechnik, Steckborn, Switzerland; Fig. 2) in order to avoid any potential damage by the study procedure. The patient’s position and range of motion (ROM) for testing and training was standardized and saved in the data-bank of the BfMC.
Fig. 2. Patient’s position during testing.
Patients were asked to start maximal isometric contraction and hold for 6 sec. They repeated the test 3 times, with one min rest between efforts. The result was calculated by the computer and given as the mean of the 3 contractions (in Newtons).
Maximal weight lifted: 1RM is the absolute maximum load a person can lift in an exercise only once. This is a theoretical maximum based on a lighter test load and a small number of repetitions. (This test is safer than trying to lift a maximum weight). Patients were asked to push a weight estimated as 50% of their maximal isometric force (tested previously). Range of movement was standardized at 25 cm, with a starting position of knee flexion at 90°. Patients were asked to repeat the movement at a speed of 2 sec per cycle (flexion/extension) as many times as possible until fatigued (supported by the Biofeedback). Maximal values were then calculated using the software “Proxomed, BfMC – Biofeedback Motor Control® GmbH (Leipzig, Germany, 1999), giving the 1RM in kg and converted into values of concentric torque (Nm).
Integrated EMG during dynamic contractions: 80% of 1RM was calculated, and set on the machine for EMG test, measuring 3 sets of 7 repetitions at speed of 2 sec per cycle with 1 min rest between sets. EMG recordings of each set (i.e. 7 repetitions) were averaged. The average of 3 sets was calculated (Fig. 1).
Patients were asked to evaluate their subjective perception of function, stiffness and pain, using the WOMAC self-assessment questionnaire (28).
TUG was performed using the standardized testing procedure (29).
Treatment protocol
All patients completed a standardized therapy programme, including walking school, climbing stairs, pain treatment, massage, hot/cold packs, passive mobilization of the operated joint and strength training for the upper extremities. In addition, according to prior randomization, a tailored knee and hip extensors training for the non-operated limb was performed 5 times a week once a day.
For the HIG we used the Leg-Press-Functional instrument at a range of knee flexion/extension/flexion set at 90°/0°/90°. Prior to training, patients performed a warm-up in the form of one set of 20 repetitions at very low intensity (< 30% of 1RM). One min rest between warm-up and training was given.
Training started with the “complex-strength development method” (10). Patients performed 3 sets of 8 repetitions. Training intensity was set at 45% of 1RM. The same intensity was used for the next few sessions until 3 sets of 15 repetitions were reached.
Then the weight was adjusted and training was progressed further until it reached the intensity of 65% of 1RM with 3 sets and 15 repetitions. At this stage, 1RM was reassessed and training was progressed to the “differentiated method-standard MA I” (10). Weight increased to 70% of 1RM with 3 sets and 8–15 repetitions. Those patients who reached this intensity were progressed to 80% of 1RM, with 3 sets and 8–15 repetitions (with the same progression as described above).
Regular intensity (control) group (RIG): patients completed 3 sets of 8 repetitions, 5 times a week, once a day, using “weight-cuffs” of minimal intensity (500 g). Exercises were performed in the sitting position, with the knee extended from 90° flexion to 0°. Each set required 30 sec of effort with 60–90 sec rest between sets.
Statistical analysis
The Wilcoxon signed-rank test was used for the analysis of the changes within groups, whereas the Wilcoxon rank-sum test was performed for the analysis of changes between groups. Influences of gender, number of training day sessions, and age were evaluated for the primary parameter of interest (ratio integrated EMG/weight lifted) using an analysis of covariance (ANCOVA). Confidence levels for all analysis were set at 95%. All data analyses were performed by the Institute of Mathematical Statistics and Actuarial Science at the University of Berne, Switzerland.
Results
All patients in both groups completed the entire training protocol. No complications or increase in pain were documented.
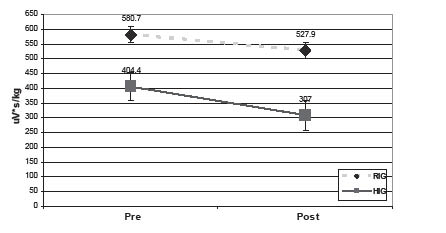
After randomization, baseline values for the ratio integrated EMG/weight lifted were significantly different (p < 0.001) between the groups. However, ANCOVA analysis proved that only group allocation and not baseline values played a significant role for the change in the primary outcome parameter, namely the ratio integratedEMG/weight lifted (p = 0.01; Fig. 3). Moreover, there was no significant influence of gender, number of trainings, or age on the ratio integratedEMG/weight lifted for this population.
Fig. 3. Changes in ratio integrated electromyography/weight lifted (μV*s/kg) pre-/post-training for each group (mean +/– standard error). HIG: high intensity group (n = 33); RIG: regular intensity group (control) (n = 29).
Significant differences were found between the groups (Tables II and III; Fig. 3) regarding changes in integrated EMG/weight lifted (p = 0.026; one-sided, lower confidence bound 9.1). This parameter decreased in the HIG from 404.4 to 307.0 μV*s/kg, corresponding to an improvement of 24% (p < 0.0001). The ratio integrated EMG/weight lifted decreased in the RIG from 580.7 to 527.9 μV*s/kg, corresponding to 9% (p = 0.014) improvement.
| Table II. Summary of univariate statistics: changes (∆) within and between groups |
| Parameter* | ∆ pre/post HIG† | ∆ pre/post RIG† | ∆ between groups‡ |
| Ratio iEMG/weight lifted (μV*s/kg) ↓ | p < 0.0001 | p = 0.014 | p = 0.026 |
| Isometric EMG↑ (μV) | p < 0.0001 | p = 0.044 | ns |
| 1RM↑ (kg) | p < 0.0001 | p = 0.0026 | p < 0.0014 |
| *↓: the value after the training is smaller than before, the change in HIG is stronger than in RIG. ↑: the value after the training is larger than before training; the change in HIG is stronger than in RIG. †Wilcoxon signed-rank test (for changes within group) ‡Wilcoxon rank-sum test (for changes between groups) iEMG: integrated electromyography; HIG: high-intensity intervention group; ns: non significant; 1RM: 1 repetiton maximum. |
| Table III. Summary of the results expressed as raw data |
| Parameter | HIG (n = 33) | RIG (n = 29) |
| Δ pre/post | % | Δ pre/post | % |
| Ratio iEMG/weight lifted (μV*s/kg) ↓ | 97.4 | 24.0 | 52.8 | 9.0 |
| iEMG (μV*s) ↓ | 3510.8 | 24.3 | 1167.3 | 8.1 |
| Isometric EMG (μV) ↑ | 212.6 | 18.1 | 49.5 | 4.2 |
| 1RM (kg) ↑ | 32.1 | 61.3 | 9.4 | 22.4 |
| Maximal concentric torque (Nm) ↑ | 78.5 | 61.1 | 22.9 | 22.3 |
| Δ: mean change; ↑: increase; ↓: decrease; %: percentage change. HIG: high-intensity intervention group; RIG: regular-intensity group. iEMG: intergrated electromyography; 1RM: 1 repetition maximum. |
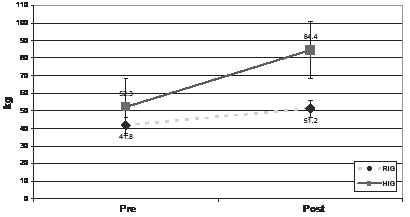
Significant differences between the groups were also found for 1RM (p = 0.0014) (Tables II and III; Fig. 4). The 1RM increased significantly in the HIG from 52.3 to 84.4 kg (61.3%; p < 0.0001) corresponding to an improvement from 128.4 Nm to 206.9 Nm (61.1%) in maximal concentric torque. Patients in the RIG also did better post-rehabilitation, showing an increase from 41.8 to 51.2 kg (22.4%; p = 0.0026), corresponding to an improvement from 102.7 Nm to 125.6 Nm (22.3%).
Fig. 4. Changes in 1 repetion maximum (in kg) pre-/post-training for each group (mean +/– standard error). HIG: high-intensity group (n = 33); RIG: regular-intensity group (control) (n = 29).
The isometric EMG improved in the HIG from 1169.9 to 1382.5 μV, corresponding to an increase of 18.1% (p < 0.0001) in recruited motor units. The same parameter increased in the RIG from 1169.4 to 1218.9 μV, corresponding to an improvement of 4.2 % (p = 0.044). The difference between the groups regarding this parameter was not significant.
Significant improvements were found for all WOMAC items and the TUG test for both groups at the end of rehabilitation (p < 0.0001 for both assessments). These parameters did not significantly differ between the groups (Table IV).
| Table IV. Western Ontario and McMaster Universities (WOMAC) and Timed “up & go” (TUG) test |
| Test | HIG (n = 33) | RIG (n = 29) |
| WOMAC | Pre- | Post- | p < | Pre- | Post- | p < |
| Pain | 22.67 | 11.95 | 0.01 | 28.98 | 11.49 | 0.0001 |
| Stiffness | 27.06 | 13.25 | 0.01 | 29.22 | 12.86 | 0.0001 |
| Function | 41.90 | 22.05 | 0.0001 | 43.36 | 21.58 | 0.0001 |
| Global | 35.27 | 18.46 | 0.001 | 38.08 | 18.00 | 0.0001 |
| TUG | 27.60 | 15.90 | 0.0001 | 29.60 | 17.60 | 0.0001 |
| WOMAC: Mean scales normalized: 0 (no symptoms) to 100 (maximal symptoms); Pre: mean values at baseline; Post: mean values at the end of rehabilitation; p <: Wilcoxon signed-rank test for changes within group. HIG: high-intensity intervention group; RIG: regular-intensity group. |
Discussion
This clinical trial provides evidence that for elderly inpatients a short rehabilitation programme in an early phase after lower limb operation is effective in improving force and function.
Previous studies had shown that unilateral strength training has cross-educational effects on the non-trained limb (1, 13, 34, 35), offering an opportunity for a training programme that can be used for the non-operated side in patients who are not allowed to train their operated limb.
Due to surgical restrictions, we could not measure the level of cross-over effects or make muscle strength assessments on the operated limb, and thus had to limit our conclusions to the training effects on the non-operated leg.
The early increase in force and the changes in EMG following strength training are hypothesized to be due mainly to motor learning rather than to an increase in muscle mass (9, 13). We therefore focused on EMG and force parameters to measure the effect of short period training. Our findings are in perfect agreement with these considerations: for the same load (80% 1RM), a lower activity of EMG was recorded post-intervention (integrated EMG per weight lifted).
Both high- and regular-intensity strength training were effective in producing functional adaptations in the neuromuscular system. Patients in the high-intensity training group showed a better integrated EMG/weight-lifted ratio, better ability to overcome more weight and higher concentric torque increase than patients in the regular intensity group.
Several explanations are possible: in order to gain functional and structural adaptations, training loads must be greater than loads encountered during activities of daily living (36). Moreover, task-specific strength programmes have been shown to enhance the increase in strength (37).
A limitation of the present study is the fact that the rehabilitation groups could not be compared with the spontaneous recovery of patients after surgery. However, as all patients were referred by orthopaedic surgeons for an inpatient rehabilitation setting, it would not have been ethical to allocate patients to a programme with no specific training elements.
Regarding some authors (38), the combination of asymmetry and weakness is prevalent in woman aged 65 years and over and may be predictive of future falls. Due to surgical restrictions, we performed asymmetrical muscle training. It is important to encourage such patients to continue their training programme post-rehabilitation, addressing the muscle imbalance. This is likely to be important in order to control disturbances in postural balance and thereby to prevent falls and fractures.
The heterogeneity of our patients prompted statistical analysis of the influence of several variables. None of them had an effect on the results described. Furthermore, the differences between the two rehabilitation groups cannot be explained by the time interval between operation and training intervention or by other patient characteristics.
The functional benefit of a comprehensive inpatient rehabilitation programme of 3 weeks is demonstrated nicely by the WOMAC self-assessment questionnaire for pain, stiffness and function. This is in perfect agreement with Rogenmoser et al. (39), who found significant improvements in WOMAC score, SF-36 and quality of life after 3 weeks of inpatient rehabilitation. In our study, we documented a significant decrease in the TUG test, a standardized instrument for mobility assessment (26). In contrast to the neuromuscular differences between high-intensity and regular training, these functional assessments did not differ significantly between the 2 patient groups in our study. This appears likely to be due to the functional restrictions by the operated limb, given for both groups. It would be interesting to determine whether additional analysis after longer periods would result in significant differences in functional mobility tests. Our WOMAC results are in agreement with a pilot study in elderly total hip arthroplasty patients (40). They found significant differences in WOMAC in both groups. Moreover, these authors found also significant differences in the 6-min walk test in favour of the intervention group. These results do not correspond with our TUG results. This discrepancy might be explained by the test character. The 6-min walk test gives more information when testing improvement in physical fitness, whereas the TUG supplies information concerning minimal mobility of the patient.
In conclusion, the results show that high-intensity early short-period postoperative muscle strength training has an effect on maximal weight lifted by the knee extensors, on isometric EMG and on the integrated EMG/weight-lifted ratio compared with regular training in the non-operated lower extremity of elderly limb-operated patients. However, no between-group differences could be demonstrated for gait ability and subjectively perceived pain, stiffness and function.
Acknowledgements
This study was supported by the “Stiftung für Medizinische Weiterbehandlung, Rehabilitation und Prävention BRH” and industrial grants by Astra-Zeneca AG, Mepha Pharma AG, MSD AG, Sanofi Aventis AG and Novartis AG.
References
1. Bemben MG, Murphy RE. Age related neural adaptation following short term resistance training in women. J Sports Med Phys Fitness 2001; 41: 291–299.
2. Koceja DM, Mynark RG. Comparison of heteronymous monosynaptic Ia facilitation in young and elderly subjects in supine and standing positions. Int J Neurosci 2000; 103: 1–17.
3. Morita H, Shindo M, Yanagawa S, Yoshida T, Momoi H, Yanagisawa N. Progressive decrease in heteronymous monosynaptic Ia facilitation with human ageing. Exp Brain Res 1995; 104: 167–170.
4. Hultborn H, Meunier S, Morin C, Pierrot-Deseilligny E. Assessing changes in presynaptic inhibition of I a fibres: a study in man and the cat. J Physiol 1987; 389: 729–756.
5. Bear M, Connors B, Paradiso M, editors. Neuroscience Exploring The Brain. 2nd edn. Baltimore; Maryland, USA: Lippincott Williams & Wilkins; 2001, p. 465–493.
6. Earles D, Vardaxis V, Kojeja D. Regulation of motor output between young and elderly subjects. Clin Neurophysiol 2001; 112: 1273–1279.
7. Ferri A, Scaglioni G, Pousson M, Capodaglio P, van Hoecke J, Narici MV. Strength and power change of the human plantar flexors and knee extensors in response to resistance training in old age. Acta Physiol Scand 2003; 177: 69–78.
8. Pfeifer M, Sinaki M, Geusens P, Boonen S, Preisinger E, Minne HW. Musculoskeletal rehabilitation in osteoporosis: a review. J Bone Miner Res 2004; 19: 1208–1214.
9. Jones DA, Rutherford OM, Parker DF. Physiological changes in skeletal muscle as a result of strength training. Q J Exp Physiol 1989; 74: 233–256.
10. Radlinger L, Bachmann W, Homburg J, Leuenberger U, Thaddey G, editors. Methoden des Krafttrainings. In: Rehabilitatives Krafttraining. Stuttgart; New York: Thieme; 1998, p. 49–87.
11. Rioult-Pedotti MS, Friedman D, Hess G, Donoghue JP. Strengthening of horizontal cortical connections following skill learning. Nat Neurosci 1998; 1: 230–234.
12. Rioult-Pedotti MS, Friedman D, Donoghue JP. Learning-induced LTP in neocortex. Science 2000; 290: 533–536.
13. Gabriel DA, Kamen G, Frost G. Neural adaptations to resistive exercise: Mechanisms and recommendations for training practices. Sports Med 2006; 36: 133–149.
14. Akataki K, Mita K, Watakabe M. Electromyographic and mechanomyographic estimation of motor unit activation strategy in voluntary force production. Electromyogr Clin Neurophysiol 2004; 44: 489–496.
15. Häkkinen K, Komi PV. Changes in neuromuscular performance in voluntary and reflex contraction during strength training in man. Int J Sports Med 1983; 4: 282–288.
16. Poyhonen T, Avela J. Effect of head-out water immersion on neuromuscular function of the plantarflexor muscles. Aviat Space Environ Med 2002; 73: 1215–1218.
17. Häkkinen K, Kallinen M, Izquierdo M, Jokelainen K, Lassila H, Mälkiä E, et al. Changes in agonist-antagonist EMG, muscle CSA, and force during strength training in middle-aged and older people. J Appl Physiol 1998; 84: 1341–1349.
18. Radlinger L, Bachmann W, Homburg J, Leuenberger U, Thaddey G, editors. Steuerung der Muskulatur: Koordination. In: Rehabilitative Trainingslehre. Stuttgart; New York: Thieme; 1998, p. 106–107.
19. Häkkinen K, Alen M, Kallinen M, Newton RU, Kraemer WJ. Neuromuscular adaptation during prolonged strength training, detraining and re-strength-training in middle-aged and elderly people. Eur J Appl Physiol 2000; 83: 51–62.
20. Tracy BL, Ivey FM, Hurlbut D, Martel GF, Lemmer JT, Siegel EL, et al. Muscle quality. II. Effects of strength training in 65- to 75-yr-old men and women. J Appl Physiol 1999; 86: 195–201.
21. Hortobagyi T, DeVita P. Favorable neuromuscular and cardiovascular responses to 7 days of exercise with an eccentric overload in elderly women. J Gerontol A Biol Sci Med Sci. 2000; 55(8):B401-B410.
22. Hortobagyi T, Devita P, Money J, Barrier J. Effects of standard and eccentric overload strength training in young women. Med Sci Sports Exerc 2001; 33: 1206–1212.
23. Suetta C, Magnusson SP, Rosted A, Aagaard P, Jakobson AK, Larsen LH, et al. Resistance training in the early postoperative phase reduces hospitalization and leads to muscle hypertrophy in elderly hip surgery patients – a controlled, randomized study. J Am Geriatr Soc 2004; 52: 2016–2022.
24. Gillespie WJ. Clinical review, Extracts from “clinical evidence” hip fracture. BMJ 2001; 322: 968–975.
25. Ulreich A, Kullich W, Klein G, Ramach W. Ergebnisse der stationären postoperativen Rehabilitation nach Hüftgelenkersatz. Rehabilitation 1998; 37: 117–122.
26. Bell DG. The influence of air temperature on the EMG/force relationship of the quadriceps. Eur J Appl Physiol Occup Physiol 1993; 67: 256–260.
27. Hamlin MJ, Quigley BM. Quadriceps concentric and eccentric exercise 2: differences in muscle strength, fatigue and EMG activity in eccentrically-exercised sore and non-sore muscles. J Sci Med Sport 2001; 4: 104–115.
28. Bellamy N. The WOMAC Knee and Hip Osteoarthritis Indices: development, validation, globalization and influence on the development of the AUSCAN Hand Osteoarthritis Indices. Clin Exp Rheumatol 2005; 23:148–153.
29. Podsiadlo D, Richardson S. The timed “up & go”: A test of basic functional mobility for frail elderly persons. J Am Geriatric Soc 1991; 39: 142–148.
30. Alkner BA, Tesch PA, Berg HE. Quadriceps EMG/force relationship in knee extension and leg press. Med Sci Sports Exerc 2000; 32: 459–463.
31. Mizner RL, Petterson SC, Stevens JE, Axe MJ, Snyder-Mackler L. Preoperative quadriceps strength predicts functional ability one year after total knee arthroplasty. J Rheumatol 2005; 32: 1533–1539.
32. Konrad P. The ABC of EMG. A practical introduction to kinesiological electromyography. Version 1.0.Powered by Noraxon inc. USA. Available from: www.noraxon.com/emg/ABC; 2005.
33. Recommendations for sensor locations on individual muscles. Available from: www.seniam.org.
34. Shima N, Ishida K, Katayama K, Morotome Y, Sato Y, Miyamura M. Cross education of muscular strength during unilateral resistance training and detraining. Eur J Appl Physiol 2002; 86: 287–294.
35. Lagerquist O, Zehr EP, Docherty D. Increased spinal reflex excitability is not associated with neural plasticity underlying cross-education effect. J Appl Physiol 2006; 100: 83–90.
36. Häkkinen A. Effectiveness and safety of strength training in rheuma toid arthritis. Curr Opin Rheumatol 2004; 16: 132–137.
37. Häkkinen K, Kallinen M, Linnamo V, Pastinen UM, Newton RU, Kraemer WJ. Neuromuscular adaptations during bilateral versus unilateral strength training in middle-aged and elderly men and women. Acta Physiol Scand 1996; 158: 77–88.
38. Skelton DA, Kennedy J, Rutherford OM. Explosive power and asymmetry in leg muscle function in frequent fallers and non-fallers aged over 65. Age Ageing 2002; 31: 119–125.
39. Rogenmoser M, Klaghofer R, Meyer RP, Kappeler U, Burki H, Hausner P, et al. Effekte der Hüftarthroplastik und der nachfolgenden stationären postoperativen Rehabilitation auf körperliche Funktion und Lebensqualität. Praxis 2003; 92: 1515–1522.
40. Maire J, Faillenet-Maire AF, Grange C, Dugué B, Tordi N, Parratte B, et al. A specific arm-interval exercise programme could improve the health status and walking ability of elderly patients after total hip arthroplasty: a pilot study. J Rehabil Med 2004; 36: 92–94.