OBJECTIVE: To develop and determine the reliability of a newly -designed resistance-enhanced dynamometer for muscle strength measurement, and to test the hypothesis that enhancing the examiner’s resisting force improves the reliability of manual muscle strength measurements.
DESIGN: An intra-examiner, inter-examiner, intra-session and inter-session reliability study.
SUBJECTS: Twenty-five men (mean age 22.5 (standard deviation (SD) 1.7) years) were tested separately by 2 examiners using the resistance-enhanced dynamometer and a traditional hand-held dynamometer for an intra- and inter-examiner reliability study. Twenty-seven volunteers (mean age 22.1 (SD 0.8) years) were tested by a female examiner using the resistance-enhanced dynamometer for an intra- and inter-session reliability study.
METHODS: Maximum resisting forces for the knee flexors and extensors were measured using the resistance-enhanced dynamometer and the traditional hand-held dynamometer.
RESULTS: The traditional hand-held dynamometer had good intra-examiner reliability (intra-class correlation coefficient (ICC) = 0.79–0.93) but poor inter-examiner reliability (ICC = 0.11–0.28). The resistance-enhanced dynamo meter had very good intra-examiner (ICC = 0.91–0.94), inter-examiner (ICC = 0.98), intra-session (ICC = 0.93–0.99) and inter-session (ICC = 0.91–0.92) reliability. The resistance-enhanced dynamometer also had better inter-examiner agreement (smallest real difference (SRD) 9–16% for resistance-enhanced dynamometer, 21–43% for traditional hand-held dynamometer).
CONCLUSION: The resistance-enhanced dynamometer had very good reliability. Enhancing the examiner’s resisting force appeared to improve the reliability of manual muscle strength measurements. The resistance-enhanced dynamometer is useful for muscle strength measurements in clinical practice.
Key words: isometric contraction, reliability, rehabilitation.
J Rehabil Med 2007; 39: 679–684
Correspondence address: Tung-Wu Lu, Institute of Biomedical Engineering, National Taiwan University, No. 1, Sec. 1, Jen-Ai Road, Taipei 100, Taiwan, ROC. E-mail: twlu@ntu.edu.tw
Submitted December 12, 2006; accepted May 7, 2007.
INTRODUCTION
Precise quantification of patients’ muscle strength during rehabilitation is essential for clinical assessment, therapeutic intervention and prediction of functional capacity. In comparison with stationary, computerized isokinetic dynamometers, manual muscle testing (MMT) and hand-held dynamometers (HHD) have greater flexibility and can be used to evaluate patients’ maximum muscle strength in different settings (1–3). While MMT assesses the maximum resisting force of the examiner’s hand using an ordinal scale, HHD provides objective, quantitative and more precise values of the maximum muscle strength with force sensors. However, test results of the HHD can be influenced by factors such as the sensitivity and construction of the dynamometer (4), the subject’s test position and stabilization (4, 5) and the examiner’s strength (4, 6–9). A dynamometer’s sensitivity may be maintained by calibration (4), while straps can be useful for subject stabilization (8, 10). Methods to address this issue of examiner strength have been proposed (11–16), but there is room for further improvement.
The examiner’s strength appeared to be a determinant of the inter-examiner reliability of HHD-measured forces if the subject’s muscle strength – including knee extensors (7) – was greater than 120 N. The knee extensors muscle strength measured by female examiners was 20–30% lower than that measured by male examiners (9). Different values of muscle strength were also found between the break and make tests. Since a break test requires the examiner to overcome the intended segmental movement of the subject, it yields at least 1.06 times greater muscle strength values than a make test during which the examiner need only resist the subject’s force (17–21). However, it is difficult to perform a break test on strong muscle groups unless the force applied by the examiner is large enough. Attaching the HHD to a fixed frame or using a belt-resisted method removes the need for the examiner to apply force to the subject (11–16), which may accommodate the issue of insufficient examiner strength. However, this eliminates the force interaction between the examiner and the subject. Sensing the subject’s force by hand helps the examiner to provide appropriate and immediate encouragement to evoke greater muscle contraction from the subject. It seems that a portable device can be reliable if the examiner can produce forces large enough to overcome the testing muscle force.
The objectives of the study were: (i) to develop a new device that can increase the force applied by the examiner in order to avoid unreliable muscle strength measurements owing to insufficient strength of the examiner; (ii) to determine the intra -examiner, inter-examiner and inter-device reliability of the new device and a traditional HHD; and (iii) to determine the intra-session and inter-session reliability of the new device.
Materials and Methods
Instruments
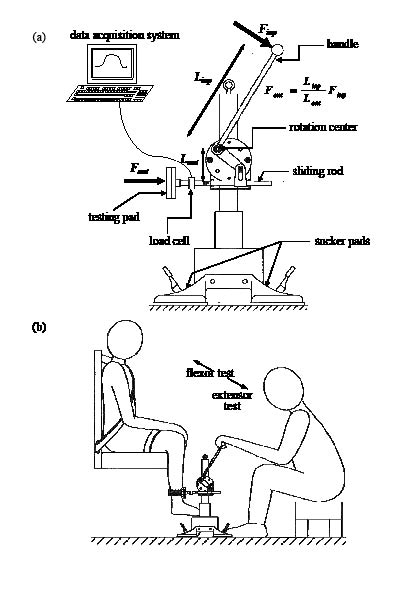
A new device called a resistance-enhanced dynamometer (RED) was developed and built by the authors to assist examiners to apply resisting forces, which can be many times greater than their own strength, to the tested limbs, (Fig. 1a). This was achieved using a leverage mechanism that amplifies the examiner applied (input) force to a much greater (output) force applied to the body segment under test (Fig. 1a). The magnification factor is given as the ratio of the input lever arm length, determined by adjusting the length of the handle, and the fixed output lever arm length (Fig. 1a). The output force Fout quantifying the subject’s muscle strength was measured by a load cell (capacity 2000 N; precision 0.0045 N; Sensotec Inc., Columbus, Ohio, USA) before being amplified, A/D converted (DAQ card-516, National Instrument Co.) and was registered by an in-house-developed program in Labview 5.0.1 (National Instrument Co., Austin, USA). The RED is a portable device because various components of the RED weighed approximately 4.5 kg and could be assembled in less than 5 minutes, with an assembled volume of approximately 46.5 × 30 × 50 cm3. The setup of the RED for knee muscle strength testing is shown in Fig. 1b. A hand-held dynamometer (GT-10, OG Giken, Inc., Okayama, Japan) with a capacity of 1000 N and an accuracy of 0.98 N was also used.
Fig. 1. (a) Schematic of the resistance-enhanced dynamometer (RED) system. The device was fixed to the ground (or wall) using 6 sucker pads, each providing a maximum suction force of 450 N. Other types of fixation structure were also developed to allow fixation to a fixed object such as a chair or table. (b) Knee flexor/extensor muscle strength testing using the RED.
Finp: input force; Fout: output force; Linp:input lever arm length; Lout:output lever arm length.
Participants
Six male and 6 female examiners with extensive clinical experience in MMT were recruited and their maximal push and pull capabilities measured (Kin-Com 500H, Isokinetic International, Tennessee, USA) in a position simulating the knee extensors/flexors strength testing (Table I). Since including all the examiners in the subsequent reliability study would cause muscle fatigue in the tested subjects, only one male and one female average-strength examiner were chosen. The selected examiners were allowed to practise using the RED and the HHD for one month before the subsequent experiments.
| Table I. Mean, standard deviation (SD) and coefficient variance (CV) of the measured push and pull forces of the male and female examiner groups |
| | Push force (N) | Pull force (N) |
| Mean (SD) | CV | Mean (SD) | CV |
| Men (n = 6) | 416.7 (47.8) | 11.5 | 552.7 (40.8) | 7.4 |
| Women (n = 6) | 252.3 (16.5) | 6.6 | 207.3 (23.7) | 11.4 |
For the intra-examiner, inter-examiner and inter-device reliability study of the RED and the HHD, 25 men volunteers (mean age 22.5 years (SD 1.7); mean weight 69.7 kg (SD 10.5); mean height 172 cm (SD 6.8)) were recruited, while 12 women and 15 men adults (mean age 22.1 years (SD 0.8); mean weight 57.9 kg (SD 12.6); mean height 165.1 cm (SD 6.3)) participated to establish the intra-session and inter-session reliability for the RED. None of the subjects had a history of injury to the test limb and all participants gave written informed consent. Permission to conduct the study was provided by the institutional human research ethics committee.
Measurement procedure
Intra-examiner, inter-examiner and inter-device reliability. All subjects underwent evaluation of knee extensors/flexors strength by the 2 examiners using the RED and the HHD. Each subject was tested 3 times per examiner, muscle group and device, with a random order of the test conditions. All subjects performed stretching exercises to warm up the testing muscles before the tests, and were then seated with the knee and hip flexed to 90° (9, 22–24), while the trunk, thigh and leg segments were stabilized using straps. The dynamometer pad was placed on the anterior surface of the lower leg, approximately 1 cm proximal to the ankle joint. For each test condition, the subject performed three 5-second maximum isometric contractions of the tested muscle, with a 2-minute rest period between contractions. Five-minute rest periods were allowed between test conditions. For knee extensor tests, the examiner applied force to the lower leg by pushing down the handle of the RED and asked the subject to “hold, don’t let me push down” (break test). For knee flexor tests, the examiner pulled the handle of the RED to apply force to the posterior surface of lower leg and asked the subject to “hold, don’t let me straighten it” (break test). Since a break test can only be performed successfully when the examiner’s strength is greater than the tested muscle strength, it was used to determine whether the RED could increase the force applied by the examiner to break the tested muscle. For tests using the HHD, a make test had to be used because the tested knee muscles were too strong for either examiner to break during our pilot study. Both subject and examiner were blind to the muscle-testing grade given by the other examiner.
Intra-session and inter-session reliability for the RED. Using the same test method for the RED as described above, each subject was tested 3 times per muscle group by the same female examiner, with a 2 minute rest between sessions on the first day. The order of the tested muscles was randomized. The re-test was performed at approximately the same time of day on a subsequent day within a period of 5 days after the first session, following the same test procedure.
Data analysis
For comparisons between test conditions, a 2 (RED and HHD) × 2 (female and male examiners) × 3 (1, 2 and 3 trials) analysis of variance (ANOVA) with repeated measurements was used. Where interactions between factors were found, multiple comparisons were performed (α = 0.008). Reliability between measures was assessed in terms of the ICC (25) using a 2-way mixed-effects model (ICC3,1) for intra-examiner assessments and a 2-way random-effects model (ICC2,k) for inter-examiner and inter-device assessments. For analysis of intra-session reliability, a 2-way mixed-effects model (ICC3,1) was used while a 2-way mixed-effects model (ICC3, k) was used for inter-session reliability. The values of the ICC ranging from 0.81 to 1.0 indicate very good; 0.61–0.80 good; 0.41–0.60 moderate; 0.21–0.40 fair; and below 0.2 poor reliability (26). Statistical analysis was performed using SPSS 13.0 (SPSS Inc., Chicago, USA).
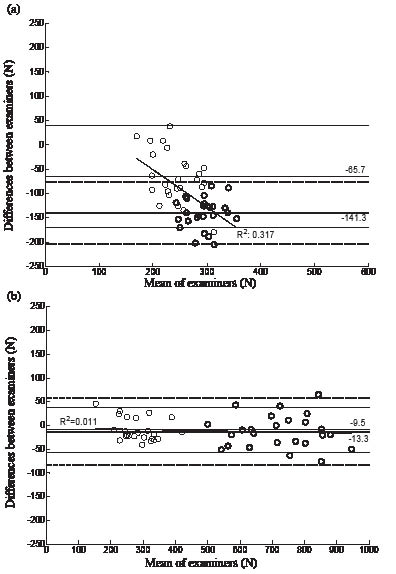
The standard error of measurement (SEM) and the smallest real difference (SRD) were used to quantify the inter-examiner and inter-session reproducibility of an assessment. The SEM was calculated using the square root of the within-subjects error variance (SEM = √WMS). The SRD (SRD = 1.96*√2* SEM, expressed as a percentage of the parameter’s grand mean) represents the limit for the smallest change that indicates a real (clinical) improvement for an individual following, for example, an intervention. Bland & Altman plots (27) were used to visualize the difference between examiners against the corresponding mean of the 2 examiners for each subject.
Results
The mean forces of the 2 muscle groups for each of the 3 trials measured by the RED and the HHD are shown in Table II. No trial main effect was found (p > 0.05). Interactions between device and examiner were found. For the knee extensors, the RED measurements between the 2 examiners were not different (p = 0.068), but both were significantly greater than those using the HHD (p < 0.001). For the knee flexors, the RED measurements for both examiners and the HHD measurements for the men were not different (p > 0.05), but all were significantly greater than the HHD measurements for the women (p < 0.001).
Good to very good intra-examiner reliability was found for the HHD in measuring knee extensors and flexors (Table II). Very good intra-examiner reliability was found for the RED for all test conditions (Table II). Very good inter-examiner reliability was also found for the RED (Table III). However, only poor to fair inter-examiner reliability was found for the HHD. Measurement errors of the RED were much smaller than those of the HHD (Table III). There was no systematic bias between examiners for the RED measurements, as opposed to the HHD measurements (Fig. 2). Poor inter-device reliability was found for knee extensors (ICC: 0.05 for male examiner, –0.001 for female examiner). Poor to good inter-device reliability was found for knee flexors (ICC: 0.79 for male examiner, 0.16 for female examiner). Very good intra-session and inter-session reliability, and acceptable measurement errors were found for the RED (Tables IV and V).
| Table II. Mean (standard deviation, SD) muscle forces of knee extensors and flexors of each of the 3 trials, and the intra-examiner reliability for all test conditions (n = 25) |
| Device | Examiner | Trial | Extensors | Flexors |
| Muscle Force (N) Mean (SD) | ICC (95% CI) | Muscle Force (N) Mean (SD) | ICC (95% CI) |
| RED | Men | 1 | 727.2 (125.5) | 0.93 (0.87–0.97) | 282.3 (55.8) | 0.93 (0.88–0.97) |
| | | 2 | 732.8 (129.0) | 281.6 (65.1) |
| | | 3 | 726.1 (122.7) | 287.8 (68.5) |
| | Women | 1 | 717.2 (116.5) | 0.94 (0.88–0.97) | 278.5 (64.0) | 0.91 (0.84–0.96) |
| | | 2 | 710.6 (127.0) | 273.8 (62.4) |
| | | 3 | 718.4 (128.8) | 273.0 (59.5) |
| HHD | Men | 1 | 365.1 (38.0) | 0.79 (0.64–0.89) | 278.5 (57.7) | 0.93 (0.88–0.97) |
| | | 2 | 362.6 (32.2) | 273.8 (54.7) |
| | | 3 | 363.9 (36.7) | 273.0 (53.4) |
| | Women | 1 | 221.7 (34.7) | 0.91 (0.83–0.95) | 211.7 (37.4) | 0.88 (0.81–0.95) |
| | | 2 | 225.7 (37.6) | 209.1 (33.8) |
| | | 3 | 220.5 (37.1) | 207.3 (36.4) |
| CI: confidence interval; RED: resistance-enhanced dynamometer; HHD: hand-held dynamometers; ICC: intra-class correlation coefficient. |
| Table III. Inter-examiner reliability of the measurements of the muscle strength of the knee extensors (A) and flexors (B) for the resistance-enhanced dynamometer (RED) and the hand-held dynamometers (HHD) (n = 25) |
| Device | Examiner | Muscle force (N) Mean (SD) | ICC (95% CI) | SEM (N) | SRD (%) |
| (A) | | | | | |
| RED | Men | 728.7 (122.9) | 0.98 (0.95–0.99) | 24.7 | 9.5 |
| | Women | 715.4 (121.5) |
| HHD | Men | 363.9 (33.1) | 0.11 (–0.05–0.44) | 22.5 | 21.3 |
| | Women | 222.6 (35.3) |
| (B) | | | | | |
| RED | Men | 287.9 (64.4) | 0.96 (0.89–0.98) | 16.7 | 16.4 |
| | Women | 278.4 (56.7) |
| HHD | Men | 275.1 (54.1) | 0.28 (–0.35–0.67) | 37.2 | 42.5 |
| | Women | 209.4 (34.7) |
| CI: confidence interval; SD: standard deviation; SEM: standard error of measurement; ICC: intra-class correlation coefficient.; SRD: smallest real difference |
Fig. 2. Bland & Altman plots for knee extensors (thick circles/lines) and flexors (thin circles/lines) for both the hand-held dynamometers (a) and the resistance-enhanced dynamometer (b). Solid lines show the mean difference; dashed lines show the 95% limits of agreement. A linear regression line with R2-value for all data is also shown for each device.
| Table IV. Means and standard deviations (SD) of the strength of the knee extensors and flexors measured with the resistance-enhanced dynamometer in 2 sessions (days) and the associated intra-session reliability (n = 27) |
| | | Extensors | Flexors |
| Session | Trial | Muscle force (N) Mean (SD) | ICC (95% CI) | Muscle force (N) Mean (SD) | ICC (95% CI) |
| First | 1 | 666.8 (241.0) | 0.99 (0.98–0.99) | 251.5 (63.7) | 0.94 (0.88–0.97) |
| | 2 | 669.6 (229.6) | 247.5 (63.9) |
| | 3 | 673.4 (229.2) | 242.4 (62.3) |
| Second | 1 | 661.1 (203.8) | 0.96 (0.93–0.98) | 255.3 (70.2) | 0.97 (0.94–0.98) |
| | 2 | 660.7 (217.5) | 248.5 (67.8) |
| | 3 | 663.6 (209.5) | 253.4 (67.3) |
| CI: confidence interval; ICC: intra-class correlation coefficient. |
| Table V. Inter-session reliability of the strength of the knee extensors and flexors measured with the resistance-enhanced dynamometer in 2 sessions (days) (n = 27) |
| Muscle | Session | Muscle force (N) Mean (SD) | ICC (95% CI) | SEM (n) | SRD (%) |
| Knee extensors | First | 669.9 (232.4) | 0.95 (0.90–0.98) | 66.2 | 27.6 |
| Second | 661.8 (207.7) |
| Knee flexors | First | 244.9 (61.4) | 0.96 (0.91–0.98) | 17.8 | 20.0 |
| Second | 250.1 (67.1) |
| CI: confidence interval; SD: standard deviation; SEM: standard error of measurement; SRD: smallest real difference; ICC: intra-class correlation coefficient. |
Discussion
Both the RED and the HHD had good to very good intra- examiner reliability for the measurement of knee muscle strength (Table II). Similar intra-examiner reliability for the HHD was also found in previous studies (20, 28, 29). Although both devices had comparable intra-examiner reliability, the maximum muscle strengths measured by the RED were greater than those measured by the HHD, especially for the extensors. The knee extensor strength measured by the HHD was within the range (100–579 N) published in the literature (20, 28, 30). In contrast, the RED measurements (710–732 N) (Table II) were similar to those measured by the KinCom, which were used as a gold standard for comparisons with the HHD measurements (31). This indicates that the HHD may have underestimated the strength of the knee extensors as a result of insufficient examiner muscle strength. The use of the RED allowed the examiners to perform break tests that might also contribute to the greater values of the RED measurements (4, 18, 19, 21).
Insufficient examiner strength might also affect the inter-examiner reliability of the HHD (5, 7, 29, 32). It would be the most important factor if the strength of the tested muscle were more than 120 N (7). Results from the current study (Fig. 2 and Table III) agree with the literature, namely that the HHD has poor inter-examiner reliability when measuring powerful muscle groups, such as shoulder extensors or knee extensors, of healthy or strong individuals (29, 32). Inter-examiner reliability between the HHD measurements carried out by female and male examiners could be even worse, as female examiners produced less resistance than male examiners when measuring the strength of powerful lower extremity muscles, as shown by Mulroy et al. (9) and the current study. This suggests that clinical decisions based on HHD measurements of powerful muscle groups may be different between clinicians, especially when the examiners’ strengths are smaller than those of the muscles under test.
Compared with the HHD, the RED had much better inter-examiner reliability when measuring the strength of knee extensors and flexors (Table III). The RED also had very good intra- and inter-session reliability. The RED increased the applied force by increasing the leverage available to the examiner by 4.5 times, so that both the female and the male examiners could produce higher resistance forces than the strengths of the knee flexors and extensors. This feature of the RED allows the examiners to perform break tests even if their own muscular strength is smaller than that of the tested muscle group. Although methods to overcome the effect of insufficient examiner strength by removing the need for the examiner to apply force to the subject have been described in the literature (11–16), break tests cannot be performed using these methods. By eliminating the problem of insufficient examiner strength, the RED achieved not only very good reliability, but also significantly better inter-examiner agreement than the HHD, and acceptable inter-session agreement, as indicated by the SRD (Tables III–V). An SRD equal to or greater than 27.55% (for knee extensors) and 19.95% (for knee flexors) between different sessions should be interpreted as the real changes in a patient’s knee muscle strength. The results of the current study suggest that enhancing the examiner’s output force by the leverage offered by the RED system helped to improve the reproducibility of the muscle strength measurements by the 2 examiners during the 2 sessions. Since the 2 examiners represented the average-strength examiner for their group, the results may be applicable to the examiner groups in the current study. Nonetheless, further studies with more examiners during more sessions are warranted to verify a general applicability.
With the portable, resistance-enhanced design, the RED system has been shown to have very good reliability in measuring muscle strength of the knee extensors and flexors, suggesting that it will be useful in clinical applications, especially for professional athletes or physically powerful populations. Although the RED can be applied to most muscle groups in its current form, additional attachments may be needed when being applied to some particular muscle groups, such as trunk muscles or hip muscles in a supine position. Further improvement of the RED system may also include adapting the data acquisition system into a display panel to reduce the time required to set up the RED system. The validity of the RED and its reliability in performing make tests will also be the subject of further study.
In conclusion, the examiner’s muscle strength affects the inter-examiner reliability of muscle strength measurements using the HHD. Insufficient examiner muscle strength leads to poor inter-examiner reliability with the HHD. A new device, the RED, which enhances the examiner’s output forces, solved this problem by increasing the leverage available to the examiner. Within the tested conditions, the RED was shown to have very good intra-examiner, inter-examiner, intra-session and inter-session reliability, as well as acceptable inter-examiner and inter-session agreement. Being portable and reliable, it is suggested that the RED can be considered as an alternative to the HHD in clinical practice and may be preferred when the examiner’s strength is less than that of the muscles under test.
REFERENCES
1. Bohannon RW. Is the measurement of muscle strength appropriate in patients with brain lesions? A special communication. Phys Ther 1989; 69: 225–236.
2. Fransen M, Crosbie J, Edmonds J. Isometric muscle force measurement for clinicians treating patients with osteoarthritis of the knee. Arthritis Rheum 2003; 49: 29–35.
3. Taylor NF, Dodd KJ, Graham HK. Test-retest reliability of hand-held dynamometric strength testing in young people with cerebral palsy. Arch Phys Med Rehabil 2004; 85: 77–80.
4. Bohannon RW. Hand-held dynamometry: factors influencing reliability and validity. Clin Rehabil 1997; 11: 263–264.
5. Byl NN, Richards S, Asturias J. Intrarater and interrater reliability of strength measurements of the biceps and deltoid using a hand-held dynamometer. J Orthop Sports Phys Ther 1988; 9: 399–405.
6. Edwards RHT, McDonnel M. Hand-held dynamometer for evalua ting voluntary muscle function. Lancet 1974; 28: 757–758.
7. Wikholm JB, Bohannon RW. Hand-held dynamometer measurements: tester strength makes a difference. J Orthop Sports Phys Ther 1991; 13: 191–198.
8. Keating JL, Matyas TA. The influence of subject and test design on dynamometric measurements of extremity muscles. Phys Ther 1996; 76: 866– 889.
9. Mulroy SJ, Lassen KD, Chambers SH, Perry J. The ability of male and female clinicians to effectively test knee extension strength using manual muscle testing. J Orthop Sports Phys Ther 1997; 26: 192–199.
10. Hart DL, Stobbe TJ, Till CW, Plummer RW. Effect of trunk stabilization on quadriceps femoris muscle torque. Phys Ther 1984; 64: 1375–1380.
11. Kramer JF, Vaz MD, Vandervoort AA. Reliability of isometric hip abductor torques during examiner- and belt-resisted tests. J Gerontol 1991; 46: M47–51.
12. Desrosiers J, Prince F, Rochette A, Raiche M. Reliability of lower extremity strength measurements using the belt-resisted method. J Aging Phys Act 1998; 6: 317–326.
13. Nadler SF, DePrince ML, Hauesien N, Malanga GA, Stitik TP, Price E. Portable dynamometer anchoring station for measuring strength of the hip extensors and abductors. Arch Phys Med Rehabil 2000; 81: 1072–1076.
14. Ford-Smith CD, Wyman JF, Elswick Jr RK, Femandez T. Reliability of stationary dynamometer muscle strength testing in community-dwelling older adults. Arch Phys Med Rehabil 2001; 82: 1128–1132.
15. Fenter PC, Bellew JW, Pitts TA, Kay RE. Reliability of stabilised commercial dynamometers for measuring hip abduction strength: a pilot study. Br J Sports Med 2003; 37: 331–334.
16. Gagnon D, Nadeau S, Gravel D, Robert J, Belanger D, Hilsenrath M, et al. Reliability and validity of static knee strength measurements obtained with a chair-fixed dynamometer in subjects with hip or knee arthroplasty. Arch Phys Med Rehabil 2005; 86: 1998–2008.
17. Bohannon RW. Make tests and break tests of elbow flexor muscle strength. Phys Ther 1988; 68: 193–194.
18. van der Ploeg RJO, Oosterhuis HJGH. The “make/break test” as diagnostic tool in functional weakness. J Neurol Neurosurg Psychiatry 1991; 54: 248–251.
19. Stratford PW, Balsor BE. A comparison of make and break tests using a hand-held dynamometer and the Kin-Com. J Orthop Sports Phys Ther 1994; 19: 28–32.
20. Bohannon RW. Reference values for extremity muscle strength obtained by hand-held dynamometry from adults aged 20 to 79 Years. Arch Phys Med Rehabil 1997; 78: 26–32.
21. Burns SP, Breuninger A, Kaplan C, Marin H. Hand-held dynamo metry in persons with trtraplegia: comparison of make- versus break-testing techniques. Am J Phys Med Rehabil 2005; 84: 22–29.
22. Bohannon RW. Manual muscle test scores and dynamometer test scores of knee extension strength. Arch Phys Med Rehabil 1986; 67: 390–392.
23. Stuberg WA, Metcalf WK. Reliability of quantitative muscle testing in healthy children and in children with Duchenne muscular dystrophy using hand-held dynamometer. Phys Ther 1988; 68: 977–982.
24. Andrew AW, Thomas MW, Bohannon RW. Normative values for isometric muscle force measurements obtained with hand-held dynamometers. Phys Ther 1996; 76: 248–529.
25. Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing rater reliability. Psychol Bull 1979; 86: 420–428.
26. Altman DG, editor. Practical statistics for medical research. London: Chapman & Hall; 1991.
27. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1: 307–310.
28. Bohannon RW. Test-retest reliability of hand-held dynamometry during a single session of strength assessment. Phys Ther 1986; 66: 206–209.
29. Agre JC, Magness JL, Hull SZ, Wright KC, Baxter TL, Patterson R, et al. Strength with a portable dynamometer: reliability for upper and lower extremities. Arch Phys Med Rehabil 1987; 68: 454–458.
30. Bohannon RW. Measuring Knee Extensor Muscle Strength. Am J Phys Med Rehabil 2001; 80: 13–18.
31. Deones VL, Wiley SC, Worrell T. Assessment of quadriceps muscle performance by a hand-held dynamometer and an iso kinetic dynamometer. J Orthop Sports Phys Ther 1994; 20: 296–301.
32. Bohannon RW. Intertester reliability of hand-held dynamometry: a concise summary of published research. Percept Motor Skills 1999; 88: 899–902.