OBJECTIVE: To assess to what extent individual physical therapy treatment goals for children with cerebral palsy are reflected in 2 standardized measures: the GMFM-88 and the PEDI.
SUBJECTS: A total of 36 paediatric physical therapists working in primary healthcare with children with cerebral palsy in their caseload.
METHODS: The International Classification of Functioning, Disability and Health was used as a measure to link individual treatment goals to the GMFM-88 and the PEDI.
RESULTS: Sixty percent of the treatment goals were covered by the 2 measures. Twenty-seven percent and 21% of the goals were reflected in the GMFM-88 and the PEDI, respectively; 12% of the goals were reflected in both instruments. Another 26% of the treatment goals appeared to be partly covered (21% in PEDI and 5% in GMFM-88). Fourteen percent of the goals were not covered by the 2 measures.
CONCLUSION: Individual goals set in a physical therapy practice for children with cerebral palsy can be linked, to a large extent, to items and activities of 2 standardized measures.
Key words: treatment goals, physical therapy, cerebral palsy, ICF, GMFM-88, PEDI.
J Rehabil Med 2007; 39: 225–231
Correspondence address: Marjolijn Ketelaar, Centre of Excellence for Rehabilitation Medicine, Rehabilitation Centre De Hoogstraat, Rembrandtkade 10, NL-3583 TM Utrecht, The Netherlands. E-mail: m.ketelaar@dehoogstraat.nl
Submitted March 7, 2006; accepted October 12, 2006
INTRODUCTION
Setting goals and evaluating them are essential steps in physical therapy intervention (1). In the last decade, the importance of setting goals and measuring outcomes in terms of meaningful activities has been stressed more and more (1–5). Goals and measures should reflect the person’s own wish to improve or change; the things that he or she feels are important. People are likely to make the greatest gains when therapy and the related goals focus on activities that are meaningful to them and that will make a difference in their lives (6). In paediatric rehabilitation this means that both the child and the parents should be involved.
In some studies with children with cerebral palsy (CP) it was found that the formulation of specific measurable goals, together with the parents and the child, was associated with an improvement in functional skills (7–9). In these studies, the Gross Motor Function Measure (GMFM) (10) and the Paediatric Evaluation of Disability Inventory (PEDI) (11) have been used as outcome measures. The results of these studies are very important, supporting the idea that goals should be specific, measurable and focus on aspects relevant to the child and the family. However, they do not give us insight into the evaluation of the individual goals. Since, in most studies, general outcome measures were used to determine the treatment effect, we do not know to what extent the individual goals were reflected in the standardized instruments used. This information is essential, because for the child and family individual problems and goals are the most relevant outcomes. Moreover, the use of standardized outcome measures in clinical practice has been emphasized more and more (5, 12). How do we know which measures to use, when we do not have information on how individual goals are related to standardized measures of first choice?
Two standardized measures widely used in the evaluation of children with CP are the GMFM and the PEDI. The GMFM measures gross motor function in a standardized situation. The PEDI assesses the child’s abilities in 3 domains: self-care, mobility and social function. Both measures have been developed for use in both clinical and research settings. In a review of measures for children with CP (13), it was concluded that these 2 instruments fulfil the criteria of reliability and validity with respect to responsiveness to change. It was suggested that the GMFM and PEDI are complementary to one another when trying to attain a complete picture of the child in evaluating changes over time or after treatment. Both measures focus on different aspects of functioning.
The aim of the present study was to find out to what extent individual physical therapy treatment goals of children with CP are reflected in 2 standardized measures, the GMFM and the PEDI. For this purpose, it was decided to use the International Classification of Functioning, Disability and Health (ICF) as a method to link individual goals to the measures. The ICF is an international framework that provides a common language and classification of different aspects of functioning and health (14), which is also useful to describe different domains of functioning in children (15, 16). Cieza et al. (17, 18) described rules to link outcome measures to ICF classifications. In this study these rules were used to link the individual goals, the GMFM and the PEDI to the ICF, in order to relate goals and measures on the basis of their content.
METHODS
As part of an intervention study in physical therapy, treatment goals were collected over a period of one year (8). At the time of that intervention study (1996) the GMFM and the PEDI were unknown in clinical practice in the Netherlands; both measures were used only for research purposes.
Subjects
Thirty-six paediatric physical therapists, working in primary healthcare with children with CP in their case-load, participated in the study. These therapists were asked to describe the treatment goals of the children with CP they treated during a period of one year. The children were between 2 and 7 years of age. All children were diagnosed with spastic CP, classified at level I, II or III of the Gross Motor Classification System (GMFCS) (19).
Instruments
Questionnaire on goals of treatment
In a period of one year, the therapists twice received a short questionnaire with open-ended questions regarding the goals of therapy. The question relevant for the present study was: “What are, at this moment, the goals of therapy for child X?” There was no minimum or maximum for the number of goals that could be reported.
Gross Motor Function Measure
The GMFM-88 is a standardized observational instrument for children with CP, developed to measure change in gross motor function over time. The test consists of 88 items that have been grouped into 5 dimensions of gross motor function: Lying and Rolling (17 items), Sitting (20 items), Crawling and Kneeling (14 items), Standing (13 items), and Walking, Running and Jumping (24 items) (10, 20).
Paediatric Evaluation of Disability Inventory
The PEDI measures both capability and performance of functional activities in daily situations in 3 domains: Self-Care, Mobility, and Social Function (11). Capability is measured by the identification of functional skills the child has mastered. For this functional skills scale, the parent indicates whether the child is capable of performing each of 197 subtasks, covered in 42 activities in the 3 domains, i.e. 15 activities in the domain Self-Care, 14 activities in the domain Mobility, and 13 activities in the domain Social Functioning. Performance of daily functional activities is measured by the level of caregiver assistance the child needs, in order to accomplish major functional activities. This is also measured by the number of modifications or amount of adaptive equipment the child uses within each domain. The Caregiver Assistance Scale measures the extent of help the caregiver provides in typical daily situations. The activities in the Caregiver Assistance Scale cover the same activities as the Functional Skills Scale. Therefore, in the present study, only the items of the Functional Skills Scale were used.
International Classification of Functioning, Disability and Health
The treatment goals, the GMFM-88 items and the PEDI activities were classified and coded according to the ICF (14). This was done using the ICF linking rules of Cieza et al. (18).
The ICF has 2 parts, each containing 2 components. The first part covers functioning and disability and includes the 2 components: (1) body functions (b) and body structures (s), and (2) activities and participation (d). The second part covers contextual factors and includes the 2 components: (1) environmental factors (e), and (2) personal factors. Every component contains several categories, which are the units of the ICF classification. The component personal factors is only broadly described, as categories have not (yet) been defined. In the ICF classification, the letters b, s, d and e, which refer to the components of the ICF, are followed by a numeric code starting with the first level category, the chapter number (1 digit), followed by the second (2 digits), third (1 digit), and sometimes the fourth (1 digit) level. The component letter with the suffix of 1, 3, 4 or 5 digits corresponds with the code of the categories. An example selected from the component activities and participation (d) would result in the following code: d4 “mobility” is the first level, d420 “transferring oneself” represents the second level, and d4200 “transferring oneself while sitting” corresponds with the third level.
Classification and coding treatment goals
The goals were divided into 2 groups: (1) goals on the ICF level of activities and participation (d), and (2) goals not on the ICF level of activities and participation (not d), using the definitions of activities and participation. In the ICF, Activity is defined as: “the execution of a task or activity by an individual”, and Participation is defined as: “involvement in a life situation” (14). For example, the goal “jumping” would be classified in the first group, as a goal on the ICF level of activities and participation, whereas a goal such as “improving balance” would be classified in the second group, as a goal not on the ICF level of activities and participation. If a goal encompassed different constructs, the information in each construct was individually linked. For instance, the goal “improving coordination of the legs in order to walk without help”. In this case “improving coordination of the legs” would not be classified as a goal on the ICF level of activities and participation, but “to walk without help” would. Eventually, only the goals classified on the level of activities and participation were further analysed in the study. For the purpose of the present study, goals not formulated at the level of activities and participation were left out of consideration.
Next step was to link an ICF code for each goal identified on the level of activities and participation. This was done by first finding a code on the first level, then a code on the second level, after that the third level followed and, if applicable and possible, the fourth too. For example, the goal “jumping”: first chapter d4 (mobility, “4”) was linked, than second level d455 (moving around, “55”) and, finally, third level d4553 (jumping, “3”). Each goal was classified and linked to codes independently by 2 researchers in paediatric rehabilitation (one social scientist/researcher and one physical therapist/social scientist/researcher). Consensus between the 2 professionals was used to decide which ICF code should be linked to each goal. To resolve disagreement between the 2 researchers concerning the selected code, a third person (human movement scientist/researcher), was consulted. After a discussion, led by the third person, that third person made an informed decision.
Classification and coding GMFM-88 and PEDI
Although both the GMFM-88 and the PEDI claim to measure on the level of activities and participation of the ICF (13), this is not necessarily so for individual items. Therefore, first, all items of the GMFM-88 and all activities of the PEDI were classified into 2 groups (as was done for the goals): (1) items on the ICF level of activities and participation, and (2) items not on the ICF level of activities and participation. After this, the items classified in the first group were linked to ICF codes. Assigning these codes took place in the same way as was done for the treatment goals. Again, 2 researchers in paediatric rehabilitation performed both the classification and the coding procedure. A third rater was consulted in case of disagreement.
Important to note, is that GMFM-88 and PEDI were approached slightly different from each other. Within the GMFM-88 each item was assigned a code. However, GMFM-88 items always begin with the starting position. For the purpose of the present study only the activity described after the starting position was coded. For example, item 2 “Supine: brings hands to midline, fingers one with the other”. In this item “supine” (the starting position) was ignored and “brings hands to midline, fingers one with the other” (the activity) was linked to a code.
With respect to the PEDI, ICF codes were assigned to each of the 42 activities, and not to all 197 items, since the items are subtasks of the activities. Coding these subtasks would be confusing and overdone for the purpose of this study, because this would result in a lot more codes. This phenomenon is confirmed by a recent study in which the PEDI was linked to the ICF (21). For instance: domain Self Care, activity C “Use of drinking containers”, items 10–14. Activity C could very well be coded as d560 (drinking), whereas item 10 “Holds bottle or spout cup (with a lid)” could be assigned code d445 (hand and arm use), which is more global and not necessarily related to drinking. When coding the items, the true activity might get lost out of sight. Therefore only the activities were coded.
Goals related to instruments
To relate the treatment goals of children with CP with the GMFM-88 and the PEDI, the ICF codes of the treatment goals were compared with the ICF codes of the instruments. The percentage of goals of which the ICF code matched the ICF code in the GMFM-88 or the PEDI was calculated.
The following procedure was carried out. For each goal, the accompanying ICF code was checked against the list of ICF codes belonging to the GMFM-88 and the PEDI. Only 100% overlap was counted. Thus, for instance, if a goal was assigned code d5400 (putting on clothes), than code d5400 should at least be reflected once in the GMFM-88 and/or PEDI items, in order to attain 100% overlap. Code d540 (dressing) for example, would not be sufficient, because this code has a (slightly) different meaning from d5400. “Putting on clothes” is not the same as “dressing”: maybe a child with CP is able to take off clothes, but not yet to put them on. In that case, code d5400 is much more specific and accurate, than code d540. Therefore, only 100% overlap was considered.
RESULTS
Agreement
For the majority of the goals, the 2 researchers found consensus concerning the correct ICF code. In 22% of the goals there was disagreement. This disagreement was mainly caused by vaguely and broadly formulated goals, which made these goals multi-interpretable. Examples of such goals are “stimulating functional skills”, “self care functions” and “improving the overall quality of movement: ball skills”.
With respect to the GMFM-88 there was a difference of opinion between the 2 researchers in 23% of the items. In most of these cases it was unclear what part of the item was the core of that particular item. For example Domain C: Crawling and Kneeling, item 43: “4 Point: Reaches forward with left arm, hand above shoulder level”. To be able to assign an ICF code, it was necessary for the researchers to know if the core of this item was maintaining a position (d4158, maintaining a body position, other specified) or making a movement (d4452, reaching). With respect to the PEDI, similar questions were raised and for 33% of the activities the third rater was consulted. For example, Mobility Domain, A: Toilet Transfers. The core of this activity could very well be changing position (d410, changing basic body position), but also a transfer (d4200, transferring oneself while sitting).
Treatment goals
In total 451 treatment goals were evaluated. Of these 451 goals, only 92 (20.4%) appeared to be formulated at the ICF level of activities and participation. The remaining treatment goals (79.6%) were coded mainly at the ICF level of body function (b) and body structure (s).
ICF codes were assigned to 81 goals (18.0%) at the level of activities and participation. The results are summarized in Table I. For 11 goals, which were found to be at the level of activities and participation, no code could be linked. These were goals that were too general, such as “training self care activities”. In total, 26 ICF codes were obtained, of which 16 had 4 digits and 10 had 3 digits. Most frequently mentioned goals were d4750 (driving human powered transportation: e.g. “riding a bicycle”) and d440 (fine hand use: e.g. “writing”). The codes d4551 (climbing: e.g. “walking up the stairs”), d5400 (putting on clothes: e.g. “putting on pyjamas”), d4553 (jumping: e.g. “jumping with two feet”), d5401 (taking off clothes: e.g. “using right arm while undressing”) and d450 (walking: e.g. “learning to walk independently”) were also often found in the treatment goals of children with CP.
| Table I. International Classification of Functioning, Disability and Health (ICF) codes assigned to treatment goals. |
| ICF | Treatment goals (n) |
| Total | 451 |
| Activities & Participation level | 81 |
| Activities & Participation level, not definable | 11 |
| Not Activities & Participation level | 359 |
| Percentage (goals on level of Activities and Participation) | 18.0% |
| ICF Code – Activities & Participation (d) | |
| 410 (changing basic body position) | 2 |
| 415 (maintaining a body position) | 1 |
| 440 (fine hand use) | 9 |
| 450 (walking) | 6 |
| 455 (moving around) | 2 |
| 465 (moving around using equipment) | 2 |
| 469 (walking and moving, other specified and unspecified) | 2 |
| 530 (toileting) | 1 |
| 550 (eating) | 1 |
| 560 (drinking) | 1 |
| 4103 (sitting) | 1 |
| 4104 (standing) | 1 |
| 4351 (kicking) | 1 |
| 4454 (throwing) | 2 |
| 4455 (catching) | 2 |
| 4501 (walking long distances) | 1 |
| 4551 (climbing) | 8 |
| 4552 (running) | 2 |
| 4553 (jumping) | 7 |
| 4750 (driving human powered transportation) | 10 |
| 5301 (regulation defecation) | 1 |
| 5400 (putting on clothes) | 8 |
| 5401 (taking off clothes) | 6 |
| 5402 (putting on footwear) | 2 |
| 5403 (taking off footwear) | 1 |
| 9200 (play) | 1 |
Instruments
GMFM-88. The GMFM-88 comprises 88 items, of which only 7 were not found to be at the level of activities and participation of the ICF. In total, 22 codes were linked to the 81 GMFM-88 items: 16 had 4 digits and 6 had 3 digits (Table II). The 7 items not classified on the level of activities and participation were: Domain A: Lying and Rolling, item 1: Supine, head in midline: Turns head with extremities symmetrical, item 3: Supine: Lifts head 45 degrees, item 4: Supine: Flexes right hip and knee through full range, item 5: Supine: Flexes left hip and knee through full range, item 10: Prone: Lifts head upright. Domain B: Sitting, item 21: Sitting on mat, supported at thorax by therapist: Lifts head upright, maintains 3 seconds, item 22: Sitting on mat, supported at thorax by therapist: Lifts head to midline, maintains 10 seconds.
| Table II. International Classification of Functioning, Disability and Health (ICF) codes assigned to the Gross Motor Function Measure (GMFM)-88 items. |
| ICF | GMFM-88 items (n) |
| Total | 88 |
| Activities & Participation level | 81 |
| Activities & Participation level, not definable | 0 |
| Not Activities & Participation level | 7 |
| Percentage (items on level of Activities and Participation) | 92.0% |
| ICF Code – Activities & Participation (d) | |
| 410 (changing basic body position) | 4 |
| 415 (maintaining a body position) | 1 |
| 429 (changing and maintaining body position, other specified and unspecified) | 10 |
| 445 (hand and arm use) | 1 |
| 450 (walking) | 2 |
| 455 (moving around) | 7 |
| 4100 (lying down) | 8 |
| 4102 (kneeling) | 2 |
| 4103 (sitting) | 4 |
| 4104 (standing) | 3 |
| 4106 (shifting the body’s center of gravity) | 1 |
| 4153 (maintaining a sitting position) | 5 |
| 4154 (maintaining a standing position) | 2 |
| 4301 (carrying in the hands) | 1 |
| 4351 (kicking) | 2 |
| 4452 (reaching) | 6 |
| 4500 (walking short distances) | 7 |
| 4501 (walking long distances) | 1 |
| 4550 (crawling) | 2 |
| 4551 (climbing) | 9 |
| 4552 (running) | 1 |
| 4553 (jumping) | 2 |
| Table III. International Classification of Functioning, Disability and Health (ICF) codes assigned to the Paediatric Evaluation of Disability Inventory (PEDI) activities. |
| ICF | PEDI activities (n) |
| Total | 42 |
| Activities & Participation level | 36 |
| Activities & Participation level, not definable | 4 |
| Not Activities & Participation level | 2 |
| Percentage (activities on level of Activities and Participation) | 85.7% |
| ICF Code – Activities & Participation (d) | |
| 310 (communicating with – receiving – spoken messages) | 2 |
| 330 (speaking) | 2 |
| 349 (communication – producing, other specified and unspecified) | 1 |
| 410 (changing basic body position) | 1 |
| 429 (changing and maintaining body position, other specified and unspecified) | 3 |
| 430 (lifting and carrying objects) | 1 |
| 469 (walking and moving, other specified and unspecified) | 2 |
| 510 (washing oneself) | 2 |
| 520 (caring for body parts) | 1 |
| 530 (toileting) | 1 |
| 540 (dressing) | 4 |
| 550 (eating) | 1 |
| 560 (drinking) | 1 |
| 649 (household tasks, other specified and unspecified) | 1 |
| 729 (general interpersonal interactions, other specified and unspecified) | 1 |
| 4551 (climbing) | 2 |
| 4600 (moving around within the home) | 1 |
| 4602 (moving around outside the home and other buildings) | 2 |
| 4750 (driving human powered transportation) | 1 |
| 5201 (caring for teeth) | 1 |
| 5202 (caring for hair) | 1 |
| 5300 (regulating urination) | 1 |
| 5301 (regulating defecation) | 1 |
| 9200 (play) | 2 |
All GMFM-88 items that were found to be at the level of activities and participation were linked to codes in chapter d4 of ICF: Mobility. Code d429 (changing and maintaining body position, other specified and unspecified: e.g. “Domain D: Standing, item 57: Standing: Lifts left foot, arms free, 10 seconds”) was used most often (10 times). Also the codes d4551 (climbing: e.g. “Domain E: Walking, Running and Jumping, item 86: Standing: Walks up 4 steps, alternating feet”), d4100 (lying down: e.g. “Domain B: Sitting, item 19: Supine: Rolls to right side, attains sitting”), d455 (moving around: e.g. “Domain C: Crawling and Kneeling, item 38: Prone: Creeps forward 6 feet”) and d4500 (walking short distances: e.g. “Domain E: Walking, Running and Jumping, item 71: Standing: Walks backwards”) were frequently linked to the GMFM-88.
PEDI. Almost 86% of the PEDI activities could be classified within the level of activities and participation of the ICF (Table III). Four activities could not be linked: Mobility Domain: C: Car Transfers, Social Function Domain: E: Problem resolution, L: Self-Protection, and M: Community Function. This was also partly found in a study by Østensjø et al., (21). They classified the last 2, self-protection and community function, as “not covered” by ICF.
Many codes were obtained, covering several chapters (3, 4, 5, 6 and 9) at the level of activities and participation of the ICF. Overall, 24 codes were assigned to the PEDI, of which 9 had 4 digits and 15 had 3 digits.
The ICF codes most frequently linked were d540 (dressing: e.g. “Self-Care Domain, I: Pullover/Front-Opening Garments”, and d429 (changing and maintaining body position, other specified and unspecified: e.g. “Mobility Domain, E: Tub Transfers”). More than half of the codes were linked only once.
Treatment goals in relation to instruments
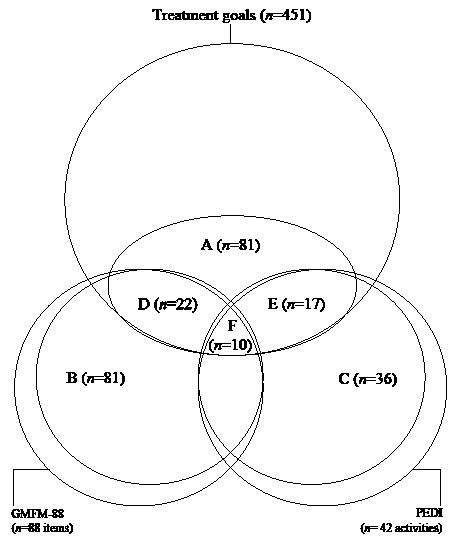
Ten (12%) treatment goals at the level of activities and participation were reflected in both the GMFM-88 and the PEDI (Fig. 1). These goals reflected 2 ICF codes: d410 (changing basic body position; n = 2), and d4551 (climbing; n = 8). Twenty-two (27%) of the goals were covered solely in the GMFM-88, and 17 (21%) of the treatment goals were measured only by the PEDI. Thus, in total, 49 goals (60%) were reflected in the GMFM-88 and/or the PEDI. Thirty-two (40%) goals were left uncovered by both instruments. These goals were linked to the ICF codes: d440 (fine hand use), d465 (moving around using equipment), d4454 (throwing), d4455 (catching), d5400 (putting on clothes), d5401 (taking off clothes), d5402 (putting on footwear) and d5403 (taking off footwear).
Fig. 1. The extent to which treatment goals overlap GMFM-88 items and PEDI activities.
A = 81 goals (18%) formulated on ICF activities and participation level;
B = 81 GMFM-88 items (92%) formulated on ICF activities and participation level;
C = 36 PEDI activities (86%) formulated on ICF activities and participation level;
D = 22 goals (27%) formulated on ICF activities and participation level are covered in the GMFM-88;
E = 17 goals (21%) formulated on ICF activities and participation level are covered in the PEDI;
F = 10 goals (12%) formulated on ICF activities and participation level are covered by both GMFM-88 and PEDI.
DISCUSSION
This study is the first to show that individual goals at the ICF activities and participation level set in a physical therapy practice for children with CP can be linked, to a large extent, to items and activities of 2 standardized measures. Twenty-seven percent and 21% of the goals were reflected in the GMFM-88 and the PEDI, respectively; 12% of the goals were reflected in both instruments. Thus, the ICF codes show that there is some, limited, overlap between the GMFM-88 and PEDI, indicating that they are complementary to a large degree and, moreover, the 2 measures together cover the majority of individual goals at the level of activities and participation of the ICF. Nevertheless, 40% of the goals on ICF activities and participation level are not covered by GMFM-88 and PEDI.
Two findings are interesting in this respect. First, rather strict criteria were used to decide whether a goal was reflected in the instruments. The codes had to be exactly the same, not taking into account the fact that both 3 and 4 ICF-digit-codes were linked. Four-digit codes are more precise than 3-digit codes, but reflect the same domain. For example, code d5400 means “putting on clothes” and d540 is defined as “dressing”. Using our strict criteria, a goal with code d5400 was not related to a PEDI activity with code d540. When analysing the relations less strictly and checking 4-digit codes in matching 3-digit code and vice versa, more relations were found. Another 21 (26%) goals are (partly) covered by the PEDI, of which 4 goals were already fully linked to the GMFM-88 (d455 moving around, n = 2; d4103 sitting, n = 1; d4104 standing n = 1) and 4 (5%) are (partly) covered by the GMFM-88. The 17 goals partly covered by the PEDI are related to the ICF codes d5400 (putting on clothes, n = 8), d5401 (taking off clothes, n = 6), d5402 (putting on footwear, n = 2) and d5403 (taking off footwear, n = 1). The goals partly covered by the GMFM-88 are related to the ICF codes d4454 (throwing, n = 2) and d4455 (catching, n = 2). In sum, the percentage partly covered goals (26%) added to the percentage fully covered goals (60%), makes a total of 86% of the treatment goals that is (partly) covered by the 2 measures.
Secondly, when looking at which goals are still not covered (14%), after checking the relations with these less strict criteria, it becomes clear that these goals are related to hand function (codes d440 fine hand use and d465 moving around using equipment). Therefore, evaluation of these specific treatment goals requires an additional measure.
The method used in this study to capture the treatment goals by asking open-ended questions might have influenced the preciseness of ICF classifying and coding in a way that some goals were classified either at the activities and participation level or not, and by this – have increased the number of false positives (to classify the goal at the activities and participation level even when it is not) and false negatives (failure to classify at the activities and participation level even when it is the case). An example of a false positive goal could be “walking on toes”. The researchers interpreted this goals as “the child wants to learn how to walk on his or her toes, because he or she wants to be able to reach or participate in play” (activities and participation). However, this goals could also have aimed at “walking on toes, in order to strengthen the muscles of the leg or improve balance” (not activities and participation). An example of a possible false negative goal is “improving hand function”. The researchers interpreted this goal as “improving mobility, strength or coordination” (not activities and participation), but maybe the intention of this goals was “improving hand function in order to write”. Moreover, the goals were described in the therapist’s own words: most goals were formulated rather generally, while others were presented in detail. This might have also caused “noise” in the classification. However, all goals were interpreted by 2 researchers independently and discussed in case of disagreement; therefore we think that the coding did not influence the overall picture.
For the purpose of this study we took advantage of data on treatment goals collected within a larger study on physical therapy, which was carried out 1996 by Ketelaar et al. (8). The advantage was a large number of goals (n = 451), collected in a standardized way, and not influenced or biased by knowledge of specific items of the GMFM-88 and the PEDI, since both instruments were unknown in clinical practice at the time of the study. A disadvantage is, that it is reasonable to assume that the process of goal setting has changed considerably in clinical practice in last 10 years. An important finding in this respect is the relatively low percentage of goals at the level of activities and participation (20.4%). Moreover, in the present study, a large number of the goals were not formulated as very specific or measurable. A lot of goals were stated rather boldly and shortly: e.g. “improve walking”, “control mobility” or just a single word “balance”. Also, it should be noted that the goals in the present study were set for children (2–7 years old) with CP, GMFCS level I, II or III. Goals of children with CP and more severe activity restrictions, i.e. GMFCS level IV or V, were not included in the study. Future studies should also contribute to our insights into the treatment goals of these children. Furthermore, we are unaware as to what extent the therapists involved the child or parents in formulating the goals. Over the last decade the importance of setting goals in terms of meaningful activities has been stressed (1–5), and some important tools to support goal setting have gained more and more attention; the Canadian Occupational Performance Measure (COPM) and Goal Attainment Scaling (GAS) (22, 23). It is probable that, when collecting treatment goals again, now 10 years later, this percentage of goals at the level of activities and participation might be higher, and goals might be formulated as more specific and measurable. In the coming years, when the COPM and GAS will probably become part of clinical practice, it would be worth studying goals again.
In conclusion, the present study provided important insight into the match between goals and measures: the GMFM-88 and the PEDI to a large extent capture the goals in everyday physical therapy practice. The ICF framework and the definitions of activities and participation provided us with a solid and unequivocal system for coding the treatment goals, the GMFM-88 items and the PEDI activities. This approach, based on the ICF linking rules published recently by Cieza et al. (18), made it possible to compare documented goals and instruments in order to know how individual goals are related to these standardized measures. This information is of utmost importance now that standardized measures are introduced – more and more – in paediatric rehabilitation and physical therapy settings for a systematic individual, client, service, and program evaluation and for accountability reasons. When therapists want to evaluate changes in activities of an individual child with CP over time, they have to make decisions about the most appropriate outcome measure by looking at the goals of the child and the items of the measures, i.e. the GMFM-88 or the PEDI. This study also illustrates that additional measures may be needed in physical therapy, for example to evaluate change in manual activities or hand function.
ACKNOWLEDGEMENTS
We gratefully acknowledge all children and service providers who participated in the study. We thank Renate Siebes and Lotte Enkelaar, who linked, respectively, the treatment goals and the GMFM-88 and PEDI to the ICF.
REFERENCES
1. Rothstein JM, Echternach JL, Riddle DL. The Hypothesis-Oriented Algorithm for Clinicians II (HOAC II): a guide for patient management. Phys Ther 2003; 83: 455–470.
2. Schut HA, Stam HJ. Goals in rehabilitation teamwork. Disabil Rehabil 1994; 16: 223–226.
3. Jette AM. Outcomes research: shifting the dominant research paradigm in physical therapy. Phys Ther 1995; 75: 965–970.
4. Rothstein JM. Disability and our identity. Phys Ther 1994; 74: 375–378.
5. Bower E. Goal setting and the measurement of change. In: Scrutton D, Damiano D, Mayston M, editors. Management of motor disorders of children with cerebral palsy. 2nd edn. London: MacKeith Press; 2004, p. 32–51.
6. Randall KE, McEwen IR. Writing patient-centered functional goals. Phys Ther 2000; 80: 1197–1203.
7. Bower E, McLellan DL, Arney J, Campbell MJ. A randomised controlled trial of different intensities of physiotherapy and different goal-setting procedures in 44 children with cerebral palsy. Dev Med Child Neurol 1996; 38: 226–237.
8. Ketelaar M, Vermeer A, Hart H, van Petegem-van BE, Helders PJ. Effects of a functional therapy program on motor abilities of children with cerebral palsy. Phys Ther 2001; 81: 1534–1545.
9. Ahl LE, Johansson E, Granat T, Carlberg EB. Functional therapy for children with cerebral palsy: an ecological approach. Dev Med Child Neurol 2005; 47: 613–619.
10. Russell D, Rosenbaum PL, Gowland C, Hardy S, Lane M, Plews N, et al. Manual for the Gross Motor Function Measure. Hamilton Canada: McMaster University; 1993.
11. Haley SM, Coster WJ, Ludlow LH, Haltiwanger J, Andrellos P, editors. Pediatric Evaluation of Disability Inventory (PEDI). Boston: New England Medical Centre Hospitals; 1992.
12. Russek L, Wooden M, Ekedahl S, Bush A. Attitudes toward standardized data collection. Phys Ther 1997; 77: 714–729.
13. Ketelaar M, Vermeer A, Helders PJ. Functional motor abilities of children with cerebral palsy: a systematic literature review of assessment measures. Clin Rehabil 1998; 12: 369–380.
14. World Health Organization. International Classification of Functioning, Disability and Health: ICF. Geneva: WHO; 2001.
15. Rosenbaum P, Stewart D. The World Health Organization International Classification of Functioning, Disability, and Health: a model to guide clinical thinking, practice and research in the field of cerebral palsy. Semin Pediatr Neurol 2004; 11: 5–10.
16. Simeonsson RJ, Leonardi M, Lollar D, Bjorck-Akesson E, Hollenweger J, Martinuzzi A. Applying the International Classification of Functioning, Disability and Health (ICF) to measure childhood disability. Disabil Rehabil 2003; 25: 602–610.
17. Cieza A, Brockow T, Ewert T, Amman E, Kollerits B, Chatterji S, et al. Linking health-status measurements to the international classification of functioning, disability and health. J Rehabil Med 2002; 34: 205–210.
18. Cieza A, Geyh S, Chatterji S, Kostanjsek N, Ustun B, Stucki G. ICF linking rules: an update based on lessons learned. J Rehabil Med 2005; 37: 212–218.
19. Palisano R, Rosenbaum P, Walter S, Russell D, Wood E, Galuppi B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol 1997; 39: 214–223.
20. Russell DJ, Rosenbaum PL, Cadman DT, Gowland C, Hardy S, Jarvis S. The gross motor function measure: a means to evaluate the effects of physical therapy. Dev Med Child Neurol 1989; 31: 341–352.
21. Østensjø S, Bjorbaekmo, Brogren Carlberg E, Vøllestad NK. Assessment of everyday functioning in young children with disabilities: an ICF-based analysis of concepts and content of the Pediatric Evaluation of Disability Inventory (PEDI). Disabil Rehabil 2006; 28: 489–504.
22. Law M, Baptiste S, Carswell A, McColl MA, Polatajko H, Pollock N. Canadian Occupational Performance Measure. Ottawa, Canada: CAOT Publications ACE; 1998.
23. Kiresuk TJ, Smith A, Cardillo JE, editors. Goal Attainment Scaling: applications, theory and measurement. Hillsdale, USA: Lawrence Erlbaum; 1994.