OBJECTIVE: To evaluate a selective implantable drop foot stimulator (ActiGait) in terms of effect on walking and safety.
DESIGN: A phase II trial in which a consecutive sample of participants acted as their own controls.
SUBJECTS: People who had suffered a stroke at least 6 months prior to recruitment and had a drop-foot that affected walking were recruited from 3 rehabilitation centres in Denmark.
METHODS: Stimulators were implanted into all participants. Outcome measures were range of ankle dorsiflexion with stimulation and maximum walking speed and distance walked in 4 minutes. Measurements were applied before implantation, at 90 days and at a long-term follow-up assessment. Changes over time and with and without stimulation are reported. Safety was evaluated by nerve conduction velocity and adverse events.
RESULTS: Fifteen participants were implanted and 13 completed the trial. Long-term improvements were detected in walking speed and distance walked in 4 minutes when stimulated, and the orthotic effect of stimulation showed statistically significant improvement. The device did not compromise nerve conduction velocity and no serious device-related adverse events were reported. Technical problems were resolved by the long-term follow-up assessment at which further improvement in walking was observed.
CONCLUSION: This trial has evaluated the safety and performance of the device, which was well accepted by patients and did not compromise safety.
Key words: electrical stimulation, implanted electrodes, rehabilitation, stroke and gait.
J Rehabil Med 2007; 39: 212–218
Correspondence address: Jane Burridge, SOHPRS, University of Southampton, Highfield, Southampton SO17 1BJ, UK.
E-mail: jhb1@soton.ac.uk
Submitted May 2, 2006; accepted October 12, 2006
INTRODUCTION
Drop-foot is a common problem following stroke, caused by a combination of weak anterior tibial muscles and calf spasticity or ankle stiffness (1), in which the individual is unable to lift the toes clear of the ground effectively during the swing phase of walking. It affects between 20% and 30% of patients undergoing rehabilitation (2) and is associated with an increased risk of falling, increased effort of walking and, in consequence, reduced mobility and independence.
The conventional approach to management of drop-foot is through the use of an orthosis, but recently functional electrical stimulation has been shown to be an effective alternative, with statistically and clinically significant improvements in walking speed and effort (3–6). A study to evaluate a surface drop-foot system (used by over 2000 patients, mainly in the UK) from the patient’s perspective identified that the main problems with the system were: inconvenience of the external components, especially in donning and doffing; positioning the self-adhesive electrodes in the correct place on the leg; and irritation of the skin under the electrodes (7). Although these problems can potentially be overcome by implanted systems, previous systems developed in the 1970s and 1980s (8–10) did not provide selective stimulation of nerve fascicles to achieve a balance between inversion and eversion of the ankle necessary for normal walking and were in some cases rejected by patients because they caused excessive ankle eversion. More recently, preliminary studies have been reported of a 2-channel implanted system that uses electrodes located under the epineurium of the deep and superficial peroneal nerves. Improvement in walking speed of 10% and 44% was shown in 2 participants (11) and good selectivity in 10 participants, identified as ankle dorsiflexion, plantarflexion, inversion and eversion torques measured in a specially designed rig (12). The effect of the system on walking with these 10 participants was not reported. The first prototype of the ActiGait system was implanted in 3 people in 1999, and has since undergone some design revisions. The objectives of this trial were to evaluate the performance and safety of the device.
METHOD
Institutional review and ethical approval was granted for the trial (VN 2002/56mch), which was performed according to the Helsinki Declaration (1983 revision). This work was funded by Neurodan A/C Denmark.
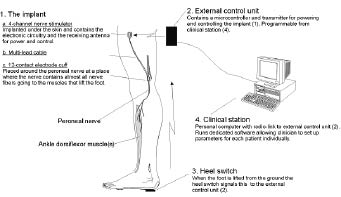
ActiGait drop-foot stimulator
The ActiGait (Fig. 1) is an implantable drop-foot stimulator that allows independent adjustment of stimulation output from each of 4 channels via a single nerve cuff. The system comprises an implant, a control unit, a heel switch that triggers the initiation and termination of each stimulation sequence, and a clinical station. The implant cuff is placed around the common peroneal nerve, just proximal to its bifurcation into the deep and superficial branches to tibialis anterior and the peronei muscles. At this point the nerve fascicles have become spatially organized within the nerve, so that each set of electrodes within the cuff is adjacent to fascicles travelling to different motor points or muscles; thus activating slightly different movements. A cable from the nerve cuff travels subcutaneously to the receiver positioned laterally on the thigh. A transmitter coil (antenna) is positioned on the skin over the receiver and is hard-wired externally to the control unit worn on the belt.
Fig. 1. The ActiGait system.
The user is able to switch stimulation on and off and make adjustments to the level of stimulation via the control unit. Stimulation is activated by a radio frequency wireless signal from a footswitch that can either be worn in the shoe, or within a sock to allow bare-foot walking. The antenna, which is attached to the skin on the upper thigh over the receiver, is easily reached by the patient without bending. Stimulation parameters are set up within the control unit via the clinical station – a standard computer (PC) and graphical software program. The clinician can control frequency, stimulation intensity, ramping and timing of the stimulation channels and can test the effect of individual and combined channels of stimulation.
Trial design
A consecutive sample of participants, recruited from 3 stroke rehabilitation centres in Denmark, acted as their own controls. Participants were assessed at baseline, at a follow-up assessment 90 days post-implantation and at a final assessment 15 months after the first participant was implanted. All assessments took place in the rehabilitation centres where the participants were recruited and were conducted by the local physiotherapists who had undergone training sessions (approximately 8 hours) in programming the ActiGait and performing the assessments.
Eligibility criteria
All participants gave written informed consent, were over the age of 18 years, and had a drop-foot following a stroke at least 6 months prior to recruitment. Drop-foot was defined as: “lacking ability to obtain normal heel contact during gait which can be corrected by electrical stimulation of the peroneal nerve”. All participants had at least 30° of passive ankle movement and were able to stand upright with heels touching the floor when the hip and knee were in a neutral position. Participants who were unable to walk 100 metres without stopping prior to their stroke, who walked faster than 1.2 metres/second (m/s), or who were unable to stand without an ankle foot orthosis at the time of screening, were excluded. Further exclusion criteria were: uncontrolled epilepsy; unstable diagnosed psychological conditions; and the presence of other implanted devices such as a cardiac pacemaker. Following screening there was an interval of at least 5 weeks before the surgical procedure. Participants understood that they were free to withdraw from the trial at any time prior to or after implantation.
Surgical procedure
Implantation was performed under spinal anaesthetic in 8 participants, and general anaesthetic in 7. The common peroneal nerve was exposed through a longitudinal incision along the tendon of the biceps femoris muscle and a second incision was made on the lateral side of the femur, posterior to the location for the stimulator body. The cuff electrode was placed around the motor part of the common peroneal nerve and the system was tested before the cuff sutures were closed. The stimulator body was secured with 1 or 2 sutures to the lateral femoral fascia and the skin incisions closed in 2 layers. The mean time for surgery was 38 minutes.
Outcome measures
Outcome measures were distance walked in 4 minutes, maximum walking speed and range of ankle dorsiflexion. Range of ankle dorsiflexion was measured by electro-goniometer (Neurodan model 01, Neurodan A/S, Aalborg, Denmark), with stimulation and without voluntary assistance in supine lying and sitting at the 90 day assessment. Maximum movement in response to 3 bursts of stimulation was recorded. Distance walked, as a measure of endurance, is an effective measure of recovery following stroke (13, 14) and speed of walking is a simple measure of walking that correlates well with other walking parameters (15). In this trial, participants walked for 4 minutes around a 20 metre figure-of-eight track marked on the floor and were given at least 15 minutes rest between tests. Total distance walked in 4 minutes and maximum walking speed over one complete circuit was recorded. Walking tests were recorded on video-tape for independent verification. Two sets of baseline walking data were recorded pre-implantation, one week apart, the first enabled participants to become accustomed to the procedure; the second was used in the analysis. Follow-up tests were performed stimulated (S) and not stimulated; order of tests was randomized by asking participants to choose 1 of 2 opaque sealed envelopes each containing a card with the words either: “with stimulation” or “without stimulation” to indicate which test was performed first.
In addition to the outcome measures, participants were asked at each assessment about how much they used of the system and any problems or benefits they had experienced. Comments were documented verbatim.
To evaluate safety, all adverse events were documented. Because of the potential risk of nerve damage due to the cuff, nerve conduction velocities were measured (16) pre-implantation and no less than 90 days post-implantation in the deep branches of the peroneal nerve to the extensor digitorum brevis, tibialis anterior muscles and the superficial branch.
Statistical analysis of the effect of stimulation
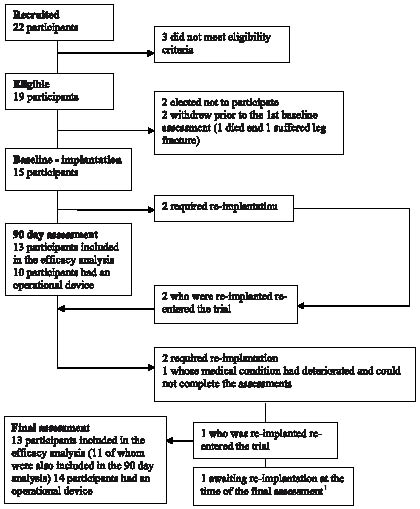
Using an intention to treat (ITT) approach to analysis, all cases for which outcome data were available were included in the analysis, including 3 participants whose devices were not working optimally at the time of assessment. Assessments were not performed with participants whose devices required re-implantation and one participant whose medical condition had deteriorated and was unable to complete the assessments. Details of problems encountered with the device and consequent availability of assessment data are shown in Fig. 2.
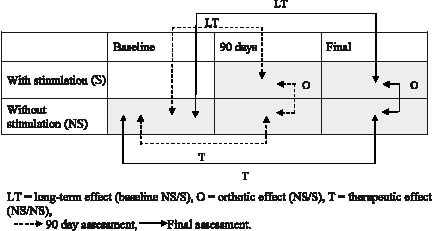
Characteristics of the trial participants at baseline and distribution of ankle range of movement were summarized using descriptive statistics. The mean standard deviation (SD) and range for walking test data amongst all participants included at each assessment are presented. The long-term effect of stimulation was based on the comparison of measurements made with stimulation at the 90 day and final assessments, and measurements made without stimulation at baseline and is the most important assessment of benefit to participants. Although we did not expect to see long-term therapeutic benefits in this group of chronic stroke patients, long-term therapeutic effects were measured based on the comparison of measurements made without stimulation at the 90 day and final assessment, and measurements made without stimulation at baseline. Finally, the short-term orthotic effect of stimulation was based on the comparison of measurements made with and without stimulation at each follow-up assessment. Comparisons are summarized in Fig. 3. Long-term, therapeutic and orthotic effects were estimated as the mean change in the relevant test values amongst participants who were included at both assessments involved, and 95% confidence intervals around mean changes were calculated. The significance of the effects was assessed using paired t-tests, and because comparisons were made at 2 time points (90 days and the final assessment) they were judged significant at the 5% level if the p value was less than the Bonferroni corrected value of 0.025.
Fig. 3. Assessment scheme, showing what comparisons were made with and without stimulation at each assessment.
RESULTS
Recruitment and progress of participants through the trial
Recruitment and progress of participants through the trial are summarized in Fig. 2. Fifteen participants underwent implantation surgery. The 90 day assessment took place within 87 and 94 days post-implantation, with the exception of one subject whose assessment was delayed until 114 days. The final assessment, took place between 6 and 15 months post-implantation (mean (SD): 11.6 (3.6) months).
Fig. 2. Progress of participants through the trial. 1Not included in the final assessment.
Baseline characteristics of the 15 participants who were implanted with the device are presented in Table I.
| Table I. Baseline characteristics of the 15 participants who were implanted with the device. |
| Characteristics | |
| Gender n (%) Female Male | 4 (27) 11 (73) |
| Age (years (y) and months (m)) Mean (SD) Min to max | 56 y 10 m (7 y 7 m) 46–68 |
| Height (cm) Mean (SD) Min to max | 172.6 (8.6) 160–187 |
| Weight (kg) Mean (SD) Min to max | 77.2 (12.9) 54–110 |
| Blood pressure (diastolic/systolic) (mmHg) Mean (SD) Min to max | 143/86 (20/5) 120/80 – 176/95 |
| Resting heart rate (bpm) Mean (SD) Min to max | 73 (9.8) 60–92 |
| Side of hemiplegia n (%) Right Left | 7 (47) 8 (53) |
| First/subsequent stroke n (%) First Second > 2 Unknown | 9 (60) 3 (20) 2 (13) 1 (7) |
| Time since last stroke (years) Mean (SD) Min to max | 4.9 (1.9) 6 m – 22 y |
| Cause of stroke n (%) Haemorrhage Infarct Unknown | 5 (33) 9 (60) 1 (7) |
| SD: standard deviation. |
The effect of stimulation on ankle angle is presented in Table II. For all participants, stimulation resulted in ankle dorsiflexion, which was on average just over 20° in both lying and sitting.
| Table II. Range of ankle joint movement (degrees) measured in lying and sitting when stimulation at the 90 day assessment: n = 13. |
| Range of ankle movement | Lying | Sitting |
| Mean (SD) Min to max 95% CI for the mean | 24.2 (11.3) 7–47 (17.4, 31.0) | 22.5 (12.3) 5–47 (16.7, 29.7) |
| CI: confidence interval; SD: standard deviation. |
During the course of the trial, 4 participants experienced problems with the system that were found to be due to the nerve cuff being too large. The protocol for determining cuff size was therefore amended and 3 participants underwent re-implantation with smaller cuffs between the 90 day and the final assessment. Two of the 3 participants were not included at the 90 day assessment, but re-entered at the final assessment; one was included at the 90 day assessment before re-implantation and at the final assessment after re-implantation. The fourth participant, included in the 90 day assessment, was still awaiting re-implantation surgery at the final assessment. At the 90 day assessment, 3 participants were experiencing problems with the wireless communication between the foot switch and the stimulator; this problem was resolved by a small redesign of the control unit.
Descriptive statistics for the maximum speed of walking and the distance walked in 4 minutes are shown in Table III at each time point for all available cases (15 at baseline, 13 at the 90 day assessment, and 13 at the final assessment). Table IV shows the long-term and long-term therapeutic effects of using stimulation, respectively, at 90 days, and at the final assessment, compared with baseline. Effects are calculated using data only from participants assessed at both time points.
| Table III. Distance walked in 4 min and maximum walking speed over one complete circuit (20 m) with and without stimulation, at the 90 day and final assessments. |
| | Baseline (n = 15) NS | 90 days (n = 13) | Final (n = 13) |
| NS | S | NS | S |
| Distance walked (m) Mean (SD) Min to max | 117.3 (46.7) 34–184 | 115.4 (49.3) 40–189 | 124.9 (47.0) 54–194 | 131 (51.5) 43–203 | 142.9 (49.3) 59–199 |
| Max speed (m/sec) Mean (SD) Min to max | 0.50 (0.20) 0.15–0.80 | 0.51 (0.22) 0.19–0.83 | 0.55 (0.20) 0.25–0.83 | 0.58 (0.23) 0.18–0.87 | 0.66 (0.22) 0.25–0.87 |
| NS: not stimulated; S: stimulated; SD: standard deviation. |
Comparisons of maximum walking speed and distance walked measured at the 90 day and final assessments with stimulation, with values measured at baseline, showed a mean improvement at both time points (Table IV). At 90 days improvements were not significant, but at the final assessment max speed showed a statistically significant improvement by virtue of its p-value falling below the Bonferroni corrected level of 0.025. Overall, there was a 19% improvement in maximum walking speed at the final assessment measured with stimulation. Although there was a trend towards an increase in both distance walked and maximum walking speed measured without stimulation at the final assessment compared with baseline (the therapeutic effect) this was not significant (Table IV). Table IV also presents orthotic effects, comparing walking with and without stimulation at each time-point. There were significant orthotic effects for both walking parameters at the 90 day assessment. At the final assessment there was a trend to greater orthotic effect than at the 90 day assessment, though the orthotic effect on distance walked did not achieve statistical significance.
| Table IV. Long-term therapeutic and orthotic effects of stimulation in distance walked in 4 min and maximum walking speed over one complete circuit (20 m): n = 13. Figures are mean difference (95% CI), paired t-test p-value. |
| | Mean diff (95% CI) | p | Mean diff (95% CI) | p |
| Long-term effects of stimulation | 90 days (S) – baseline (NS) | | Final (S) – baseline (NS) | |
| Distance walked (m) | 9.23 (–0.67, 19.13) | 0.065 | 16.23 (2.03, 30.43) | 0.028 |
| Max speed (m/sec) | 0.05 (0.00, 0.10) | 0.041 | 0.10 (0.03, 0.17) | 0.008 |
| Long-term therapeutic effects of stimulation | 90 days (NS) – baseline (NS) | | Final (NS) – baseline (NS) | |
| Distance walked (m) | –0.31 (–10.57, 9.96) | 0.949 | 4.77 (–8.42, 17.96) | 0.446 |
| Max speed (m/sec) | 0.01 (–0.04, 0.06) | 0.634 | 0.04 (–0.04, 0.11) | 0.282 |
| Orthotic effect of stimulation | 90 days (S – NS) | | Final (S – NS) | |
| Distance walked (m) | 9.54 (2.53, 16.55) | 0.012 | 11.46 (–0.12, 23.04) | 0.052 |
| Max speed (m/sec) | 0.04 (0.01, –0.07) | 0.023 | 0.07 (0.02, 0.11) | 0.011 |
| CI: confidence interval. |
At both the 90 day and long-term follow-up assessments, 11 of the 13 (91%) participants reported using the system everyday and one between 3 and 6 days per week.
Safety
No adverse events were reported during surgery. In 2 cases minor wound infections required treatment with antibiotics and in one case wound healing was delayed. No serious device-related adverse events were reported. There were no changes in nerve conduction velocity related to the nerve cuff. Table V shows the pre- and post-operative conduction velocities for each participant and each nerve branch tested. Conduction velocity > 39 m/sec is considered normal in the nerves tested (16). In 12 out of 15 subjects all assessments of conductance velocity in n. peroneus profundus, derivate m. extensor digitorum brevis and derivate m. tibialis anterior and n. peroneus superficialis were normal. In 3 subjects (3, 11, 15) the conductance velocity of n. profundus to m. extensor digitorum brevis was reduced distally in the lower leg pre-operatively, but these participants experienced no further reduction post-operatively. Although most participants showed change in conduction velocity, none were considered clinically relevant and none fell outside normal range.
| Table V. Conduction velocity (m/sec) of n. peroneus profundus, deriviate to m. extensor digitorum brevis (m.EDB) and m. tibialis anterior (m.TA) and n. peroneus superficialis (n.PS) pre- and > 90 days post-surgery. |
| ID | m.EDB | m.TA | n.PS |
| Pre-surgery | Post-surgery | Pre-surgery | Post-surgery | Pre-surgery | Post-surgery |
| 1 | 48 | 55 | 66 | 71 | 62 | 77 |
| 2 | 40 | 41 | 55 | 63 | 57 | 59 |
| 3 | 36* | 37* | 46 | 52 | 58 | 63 |
| 4 | 43 | 42 | 72 | 100 | 65 | 86 |
| 5 | 47 | 51 | 75 | 63 | 87 | 83 |
| 6 | 45 | 49 | 75 | 80 | 90 | 88 |
| 7 | 45 | 47 | 64 | 64 | 60 | 56 |
| 8 | 49 | 47 | 61 | 55 | 61 | 61 |
| 9 | 40 | 49 | 58 | 58 | 52 | 52 |
| 10 | 50 | 51 | 52 | 52 | 52 | 52 |
| 11 | 38* | 41 | 57 | 50 | 50 | 52 |
| 12 | 48 | 54 | 73 | 92 | 83 | 80 |
| 13 | 47 | 44 | 55 | 58 | 58 | 58 |
| 14 | 50 | 49 | 77 | 78 | 76 | 79 |
| 15 | 34* | 37* | 78 | 77 | 80 | 66 |
| *Abnormally reduced nerve conduction velocity. |
DISCUSSION
The ActiGait drop foot stimulator has been evaluated in terms of safety (16) and performance, and results suggest that it may be a safe and feasible way of improving walking in people who have a drop foot as a result of a stroke. As with surface systems reported previously in the literature, our results show a similar improvement in maximum walking speed over time (19%). At the final assessment, however, 91% of participants who had a functioning system reported using the system regularly, compared with 53% using a comparable surface system (7). The only implanted system reported in the literature recently (11) showed slightly better results than ours, but was only reported on 2 patients. In this study we did not measure the selectivity achieved by individual control of the 4 stimulation channels, but in all cases it was possible to achieve satisfactory ankle movement during walking. Walking appears to continue to improve beyond 3 months, as shown by greater improvement both with and without stimulation at the final assessment compared with baseline and 90 days, in both maximum walking speed and distance walked in 4 min.
Although this study recruited participants from a chronic stroke population, evidence for continuing change, either improvement or deterioration, and especially in gait parameters, beyond 12 months from stroke (17) means that the interval between assessments is important. Subsequent trials should therefore not only include a control group, but should also ensure that assessments are performed at the same intervals for all participants.
Two participants (who required re-implantation with a smaller cuff-size) did not have a functioning device at the time of the 90 day assessment, did not have assessments made and could not be included in the analysis at that time point. Both participants were, however, included in the final assessment following re-implantation. The trial sample at each assessment was therefore not the same and because of the small sample this may have influenced the results. Assessments with participants who experienced footswitch communication problems at the 90 day assessment and whose walking was therefore suboptimal were included in the analysis following an ITT approach. This trial has provided an opportunity to resolve both these problems so that we are now in a good position to perform a larger trial incorporating ITT analysis with all participants at follow-up.
Because this was a phase II trial we did not specifically define efficacy comparisons as primary and secondary. Nevertheless, there were expectations that the long-term effect of stimulation and the orthotic effects would show worthwhile improvements, with no expectation of long-term therapeutic benefit. To take account of the testing at 2 time-points Bonferroni corrections to the significance levels were used. Although the findings concerning efficacy are encouraging, the study was essentially exploratory and we would like to see the results replicated in a larger randomized controlled trial.
Our experience in conducting this trial has led us to consider the relevance of measurements taken in the artificial environment of a physiotherapy department, as they may not reflect the actual benefit that patients regard as being important in their everyday life. Discussions with participants identified individual’s different reasons for using the system – each participant had their own expectations and goals, although increased confidence in walking seemed to be predominant. It may therefore be more appropriate in future investigations to use a patient-centred outcome measure, such as the Canadian Occupational Performance Measure (COPM) (18–20), which has recently been shown to be sensitive to changes following use of a surface drop-foot system with patients suffering from multiple sclerosis (21). In addition to this, as well as recording walking parameters in a controlled environment, we are considering using an activity monitor to record activity in the everyday environment over a period of 7 days.
Participants who took part in the trial were younger than the average stroke population, without co-morbidity and at least 6 months post-stroke – it may be that this is a more active sub-population, for whom the problem of drop-foot has persisted, who are most appropriate for this intervention. The system may also be feasible for use in other upper motor neurone lesions, such as multiple sclerosis and incomplete spinal cord injury.
In conclusion, the ActiGait drop foot stimulator is a safe and feasible way of correcting drop foot in stroke patients. There were no incidences of clinically relevant reduction in nerve conduction velocity due to the implant; therefore it is concluded that the risk of nerve damage due to the surgical procedures and the encircling of the nerve by the cuff-electrode is minimal. Acceptance in this group of patients was better than reported in a previous study of a surface system. Based on the experience and results of this phase II trial, we recommend a larger randomized controlled trial be carried out incorporating patient centred objective outcome measures that reflect the perceived benefit of the device.
REFERENCES
1. Burridge JH, McLellan DL. Relation between abnormal patterns of muscle activation and response to common peroneal nerve stimulation in hemiplegia. J Neurol Neurosurg Psychiatry 2000; 69: 353–361.
2. Karsnia A, Dillner S, Ebefors I, Lundmark P. Why patients use or reject a peroneal muscle stimulator. Advances in External Control of Human Extremities 1990; 251–260.
3. Burridge JH, Taylor PN, Hagan SA, Wood DE, Swain ID. The effects of common peroneal stimulation on the effort and speed of walking: a randomized controlled trial with chronic hemiplegic patients. Clin Rehabil 1997; 11: 201–210.
4. Taylor PN, Burridge JH, Dunkerley AL, Wood DE, Norton JA, Singleton C, et al. Clinical use of the Odstock Dropped Foot Stimulator. Its effect on speed and effort of walking. Arch Phys Med Rehabil 1999; 80: 1577–1583.
5. Glanz M, Klawansky S, Stason W, Berkey C, Chalmers TC. Functional electrical stimulation in post-stroke rehabilitation: a meta-analysis of the randomised controlled trials. Arch Phys Med Rehabil 1996; 77: 549–553.
6. Wieler M, Stein RB, Ladouceur M, Whittaker M, Smith AW, Naaman S, et al. Multicenter evaluation of electrical stimulation systems for walking. Arch Phys Med Rehabil 1999; 80: 495–500.
7. Taylor PN, Burridge JH, Dunkerley AL, Lamb A, Wood DE, Norton JA, et al. Patients’ perceptions of the Odstock Dropped Foot Stimulator (ODFS). Clin Rehabil 1999; 13: 439–446.
8. Waters RL, McNeal DR, Faloon W, Clifford B. Functional electrical stimulation of the peroneal nerve for hemiplegia. Long-term clinical follow-up. J Bone Joint Surg Am 1985; 67: 792–793.
9. Rozman J, Acimovic-Janezic R, Tekavcic I, Kljajic M, Trlep M. Implantable stimulator for selective stimulation of the common peroneal nerve: a preliminary report. J Med Eng Tech 1994; 18: 47–53.
10. Lyons GM, Sinkjaer T, Burridge JH, Wilcox DJ. A review of portable FES-based neural orthoses for the correction of drop foot. IEEE Trans Neural Syst Rehabil Eng 2002; 10: 260–279.
11. Kenney L, Bultstra G, Buschman R, Taylor P, Mann G, Hermens H, et al. An implantable two channel drop foot stimulator: initial clinical results. Artif Organs 2002; 26: 267–270.
12. Kottink AIR, Buschman R, Kenney L, Veltink PH, Slycke P. The sensitivity and selectivity of an implantable two-channel peroneal nerve stimulator system for restoration of dropped foot. Neuromodulation 2004; 7: 277–283.
13. Pohl PS, Duncan PW, Perera S, Liu W, Lai SM, Studenski S, et al. Influence of stroke-related impairments on performance in 6-minute walk test. J Rehabil Res Develop 2002; 39: 439–444.
14. Butland RJ, Pang J, Gross ER, Woodcock AA, Geddes DM. Two-, six-, and 12-minute walking tests in respiratory disease. BMJ (Clin Res Ed) 1982; 29: 284 (6329): 1607–1608.
15. Wade DT, Wood VA, Heller A, Maggs J, Hewer RL. Walking after stroke. Measurement and recovery over the first 3 months. Scand J Rehabil Med 1987; 19: 25–30.
16. Jay A, Liveson DMM, editors. Laboratory reference for clinical neurophysiology. Philadelphia: F.A. Davis company, 1992.
17. Kwakkel G, Kollen BJ, Wagenaar RC. Long term effects of intensity of upper and lower limb training after stroke: a randomised trial. J Neurol Neurosurg Psychiatry 2002; 72: 473–479.
18. Law M, Polatajko H, Pollock N, McColl MA, Carswell A, Baptiste S. Pilot testing of the Canadian Occupational Performance Measure: clinical and measurement issues. Can J Occup Ther 1994; 61: 191–197.
19. Law M, Baptiste S, McColl MA, Opzoomer A, Polatajko H, Pollock N. The Canadian Occupational Performance Measure: an outcome measure for occupational therapy. Can J Occup Ther 1990; 57: 82–87.
20. McColl MA, Doubt L, Paterson M, Law M. Validity and community utility of the Canadian Occupational Performance Measure. Can J Occup Ther 2000; 67: 22–30.
21. Esnouf JE, Taylor PN, editors. Does the Canadian occupational performance measure determine if the Odstock Drop Foot Stimulator improves activities of daily living for people with multiple sclerosis. Proceedings of the 9th Annual IFESS Conference 6–7 September 2004, Bournemouth UK, pp. 267–269. ISBN 1-85899-191-9.