OBJECTIVE: This study examined the additional therapeutic effects of electroacupuncture for patients with first-ever ischaemic stroke.
DESIGN: Randomized controlled study.
SUBJECTS: A total of 63 patients with first-ever ischaemic stroke.
METHODS: The study and control groups underwent a conventional rehabilitation program, with the former receiving an additional 8 courses of electroacupuncture over a period of one month. Therapeutic effects were assessed by the Fugl-Meyer Assessment for motor performance and the Functional Independence Measure (FIM™) for the independence of functional performance at 2 and 4 weeks after treatment, and 3 months and 6 months after stroke.
RESULTS: For total Fugl-Meyer Assessment score, improvement was more significant for the study group relative to the control group at 2 weeks (16.2 vs 10.6; p = 0.047) and 4 weeks after treatment (27.4 vs 17.1; p = 0.005), and at 3 months after the stroke (34.7 vs 21.8; p = 0.009). The Fugl-Meyer Assessment scores improved significantly, especially in upper-limb motor function for the study group. There was no statistically significant between-group difference in total FIM™ score improvement.
CONCLUSION: Electroacupuncture can improve motor function, especially in upper-limb motor function, for patients with first-ever ischaemic stroke.
Key words: electroacupuncture, ischaemic stroke, therapeutic effects, Fugl-Meyer Assessment, Functional Independence Measure.
J Rehabil Med 2007; 39: 205–211
Correspondence address: Wen-Chung Lee, Graduate Institute of Epidemiology, College of Public Health, National Taiwan University, No. 17, Xuzhou Road, Taipei 100, Taiwan.
E-mail: M001052@ms.skh.org.tw
Submitted April 7, 2006; accepted October 11, 2006
Introduction
Stroke is a disabling chronic disease, which imposes a great burden on the patient, family and community (1, 2). One-third of stroke survivors remain moderately-to-severely disabled after conventional rehabilitation (1) and half must live with the sequelae of stroke (2). In Taiwan, post-stroke rehabilitation accounts for 12% of patients visiting physical medicine and rehabilitation clinics and half of these are patients with first-ever ischaemic stroke (3).
After a stroke some patients request complementary therapies, such as acupuncture, in the hope of further improvement. According to traditional Chinese medicine based on the theory of yin and yang, there is an energy flow called qi through the organs, which is essential for health (4, 5). Acupuncture can correct the imbalance of energy circulation and has been used in China for more than 3000 years (5, 6). Studies focusing on the efficacy of acupuncture for stroke have been conducted previously and showed inconsistent results (1, 7–14). As the haematoma resolves, haemorrhagic stroke survivors have a better functional prognosis than ischaemic stroke survivors (15). In addition, recurrent stroke is an established poor prognostic indicator for stroke rehabilitation outcome (16). Meta-analysis by mix-up of different stroke types (ischaemic vs hemorrhagic, first-ever vs recurrent) may mask the real effect of electroacupuncture (EA) to different types of stroke (17, 18). A study by Hu et al. (12) is the only one that have examined the effects of needle EA on patients after first-ever ischaemic stroke. The study, which utilized the Scandinavian Neurological Stroke Scale for measurement of severity and Barthel index for functional activity, revealed significantly better neurological recovery and no effect in functional improvement for an acupuncture group. Unfortunately, sum score was used and between-item comparison of the scale was not performed. Therefore, we could not determine from the study which part of neurological recovery is statistically significant.
In this study, we conducted a randomized control trial to examine the additional therapeutic effects of EA for patients with first-ever ischaemic stroke in conjunction with conventional rehabilitation.
Methods
Patients diagnosed with first-ever ischaemic stroke admitted to Shin Kong Wo Ho-Su Memorial Teaching Hospital were recruited for this study. The research committee of the hospital approved the protocol. Inclusion criteria were: (i) first-ever ischaemic stroke (confirmed by computerized tomography (CT) scan or magnetic resonance imaging (MRI) according to World Health Organization definition); (ii) age over 40 years; (iii) admission within 2 weeks of onset; (iv) stable condition and suitable for rehabilitation program after consultation with a physiatrist; and (v) informed consent available from patients or families. A total of 316 patients were not referred to the rehabilitation program due to minimal functional or neurological deficit. Seventy-seven patients were excluded due to acute life-threatening illness, significant systemic disease and haemodynamic instability. Eight patients declined to participate in the study and 2 were excluded due to recurrent stroke during the hospitalization. Basic information, including age, gender, education level and systemic disease status, were collected. Pre-morbid social activities, such as social interaction with relatives and friends, and participation in formal, outdoor and leisure activities, were also recorded.
Patients were allocated into study and control groups following the principle of simple block randomization. The allocation of the groups was initially concealed. A concealed envelope was opened for each consecutive patient to reveal his/her group assignment at the time when he/she was recruited into the study. All patients, irrespective of group assignment, underwent a conventional program of stroke rehabilitation (physical and occupational therapy, with speech therapy if indicated). Drug therapy was not pre-specified, but was allowed at the discretion of the attending physicians. The study group underwent an additional 2 courses of EA treatment per week, with a total of 8 sessions in one month. If the patient was discharged within one month, post-discharge EA treatment was arranged at the originally scheduled time on an outpatient basis. If the patients in the control group requested EA, the treatment was administered 6 months after the stroke, when all evaluations related to the present study had been completed.
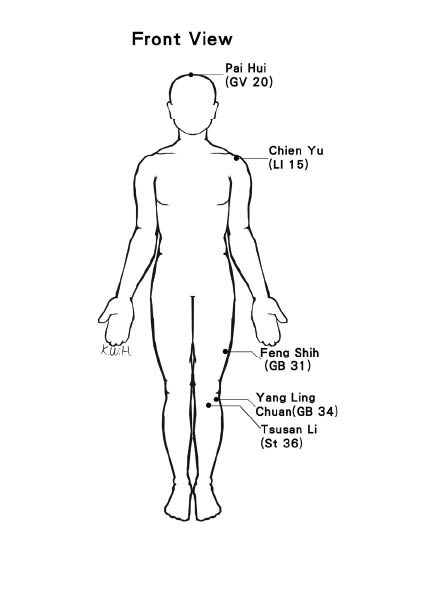
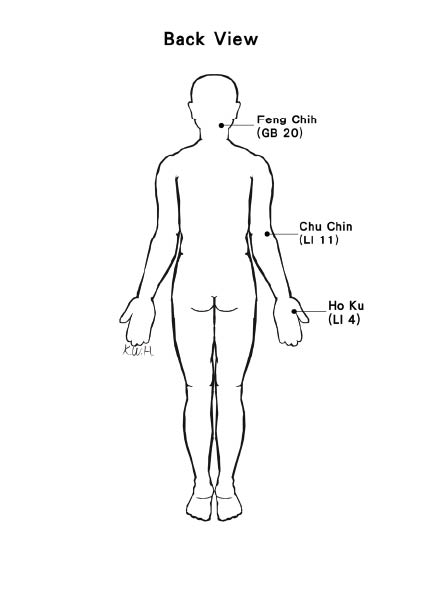
EA was performed by a qualified and experienced acupuncturist who was responsible for inserting needles into the acupoints. According to the traditional Chinese medicine (19), acupoints including Pai Hui (GV 20), bilateral Feng Chih (GB 20), and, Chien Yu (LI 15), Chu Chin (LI 11), Ho Ku (LI 4), Feng Shih (GB 31), Yang Ling Chuan (GB 34) and Tsusan Li (St 36) on the paralysed side (1, 7–9, 12) were selected (Fig. 1a and b). The disposable stainless steel needles (0.25 mm in diameter, 50 mm long) were sterilized and individually wrapped. Two bipolar leads from an electrical generator were connected to 2 pairs of needles (Chu Chin (LI 11) to Ho Ku (LI 4), and Feng Shih (GB 31) to Yang Ling Chuan (GB 34), respectively) (7–9). The electrical generator had a variable output of up to 10 mA (7), with alternating stimulation pulses (3 and 15 Hz). The intensity of the stimulation was raised to a level that was considered neither painful nor unbearable by the patients (7). The treatment lasted for 20 min (12).
Fig. 1. Acupoints used in the study.
A physiatrist who was unaware of group assignment assessed the patients before commencement, at 2 and 4 weeks after treatment, and at 3 and 6 months after stroke. Motor performance status was evaluated using the Fugl-Meyer Assessment (FMA), an instrument which incorporates Brunnstrom’s recovery sequence as a framework to evaluate 5 components, including upper- and lower-extremity motor function, balance, sensation, joint range-of-motion, and pain (20, 21). The maximum FMA score was 226. Individual items within each component are graded on a 3-point ordinal scale. We did not evaluate joint pain due to the poor expression in a few patients. Therefore, the maximal possible FMA score was 182 in this study. Functional Independence Measure (FIM) was used for functional assessment, with a 7-point scale for evaluation of a total of 18 items in the categories, self-care, sphincter control, mobility, locomotion, communication, and social cognition (total score range, 18–126 points) (22). The self-care, sphincter control, mobility and locomotion can be classified as motor subscale and the communication and social cognition as social-cognition subscale.
Chi-square or Student’s t-tests were used to analyse demographic data, such as age, gender and complications. Student’s t-test was also used to compare the between-group changes in score. Score change, which was derived by subtracting pre-treatment score from the scores at 2 and 4 weeks post-treatment, and at 3 and 6 months after stroke, respectively, was used to measure improvement. For both the FMA and FIM, a greater change in score implied more effective treatment, with the difference considered significant as p < 0.05.
We performed repeated measurement analysis of variance (ANOVA) to study the group × time interaction effect. Intention to treat (ITT) analysis (last observation carried forward) was also performed.
Results
In total, 63 patients (35 men, 28 women, age range 59–88 years) were recruited. There were 30 subjects in the study group and 33 in the control group. There were no significant between-group differences in age, education level, pre-morbid social activity, hypertension, diabetes mellitus, cardiovascular disease, total cholesterol level, triglyceride, or haemoglobin. However, there were more men and smokers in the control group (12 men in the study group and 23 men in the control group, p = 0.018; 4 smokers in the study group and 14 smokers in the control group, p = 0.011) (Table I). No significant differences were demonstrated for stroke-lesion site, electroencephalogram (EEG), or transcranial Doppler sonography comparing the 2 groups (Table I). There were also no significant differences in haemineglect, haemianopsia, nystagmus, dysphagia and aphasia conditions (data not shown). Furthermore, there was no significant between-group difference in the number of complications during hospitalization, such as urinary-tract infection, pneumonia, chronic obstructive pulmonary disease with secondary infection, cardiovascular disease (including coronary artery disease and arrhythmia), musculoskeletal disease (including tendenitis, muscle strain, and frozen shoulder), fracture, and gastric or duodenal ulcer (data not shown).
| Table I. Characteristics of the study subjects. |
| Characteristics | Study group (n = 30) | Control group (n=33) | p-value |
| Age, years (mean) | 68.8 | 70.7 | 0.470 |
| Sex, n | | | |
| Male | 12 | 23 | 0.018* |
| Female | 18 | 10 | |
| Education | | | |
| None | 9 | 9 | 0.811 |
| Yes | 21 | 24 | |
| Pre-morbid social activities, n | | | |
| No | 1 | 1 | 0.730 |
| Yes | 29 | 32 | |
| Medical history, n | | | |
| Hypertension | | | |
| No | 17 | 18 | 0.866 |
| Yes | 13 | 15 | |
| Diabetes mellitus | | | |
| No | 22 | 21 | 0.409 |
| Yes | 8 | 12 | |
| Ischaemic heart disease | | | |
| No | 23 | 25 | 0.933 |
| Yes | 7 | 8 | |
| Smoking, n | | | |
| No | 26 | 19 | 0.011* |
| Yes | 4 | 14 | |
| Triglyceride (mg/dl) | 153.3 (106.3) | 151.5 (95.3) | 0.943 |
| mean (SD) | | | |
| Total cholesterol (mg/dl) | 190.3 (41.0) | 182.5 (43.6) | 0.483 |
| mean (SD) | | | |
| Haemoglobin (g/dl) | 12.6 (1.68) | 13.2 (1.5) | 0.095 |
| mean (SD) | | | |
| Hemiplegia, n | | | |
| Right | 11 | 16 | 0.499 |
| Left | 18 | 15 | |
| Bilateral | 1 | 2 | |
| EEG1, n | | | |
| Normal | 3 | 2 | 0.598 |
| Abnormal | 19 | 21 | |
| Transcranial Doppler sonography1, n | | | |
| Normal | 14 | 7 | 0.781 |
| Abnormal | 12 | 17 | |
| *p< 0.05 1Not all cases had been studied. SD: standard deviation. |
The follow-up rates for the study group were 84% and 80% (at 2 and 4 weeks after treatment, respectively), and 73% and 67% (at 3 and 6 months after stroke, respectively); the corresponding figures for the control group were 94%, 91%, 73% and 67%, respectively. There was no significant difference in follow-up rate comparing the 2 groups. The major cause of loss to follow-up after discharge was inconvenience to the patient and/or family with respect to continuation of hospital rehabilitation away from home. Two patients in the study group and 3 in the control group were admitted to an institution after discharge. Two of the controls withdrew during follow-up due to medical complications. The comparison of patients’ characteristics between those followed and those dropped out showed no significant difference.
For FMA score, no significant difference was noted for the pre-treatment scores comparing the 2 groups (Table II). For total FMA score, improvement was more significant for the study group in relation to the control group at 2 (16.2 vs 10.6; p = 0.047) and 4 weeks after treatment (27.4 vs 17.1; p = 0.005), and at 3 months after the stroke (34.7 vs 21.8; p = 0.009). Six months after the event, the study group had improved by 35.3 and the control group by 25.6; however, statistical significance was not demonstrated comparing the 2 groups. In the category of upper-extremity motor function, more improvement was determined for wrist motor function comparing the study group with the control group at 4 weeks after treatment (2.4 vs 0.9; p = 0.018), and at 3 (3.0 vs 1.3; p = 0.024) and 6 months after stroke (3.4 vs 1.2; p = 0.010). As for hand motor function, more improvement was demonstrated for the study group relative to the controls at 2 (2.0 vs 0.7; p = 0.025) and 4 weeks after treatment (2.9 vs 1.0; p = 0.020), and at 3 (4.6 vs 1.4; p = 0.002) and 6 months after stroke (4.7 vs 2.1; p = 0.016). Further improvement was also demonstrated in upper-extremity coordination and speed comparing the study group with the control group at 2 (1.2 vs 0.5; p = 0.038) and 4 weeks post-treatment (1.7 vs 0.8; p = 0.044), and at 3 (2.5 vs 1.1, p = 0.017) and 6 months after stroke (2.5 vs 1.3; p = 0.049). There was no significant difference in the improvement in lower-extremity motor function and the related coordination and speed, balance, and sensation at the 4 follow- up assessments between the 2 groups. As for joint range-of-motion, the study group improved by 0.7 degrees while the control group decreased by 0.7 degrees at 3 months after stroke (p = 0.029). Repeated measurement ANOVA with/without ITT also showed significant group × time interaction effect in total FMA scores, wrist and hand motor function.
| Table II. Initial score and improvement in Fugl-Meyer Assessment after treatment. |
| Time point | Study group mean (SD) | Control group mean (SD) | p-value | Repeated measurement ANOVA p-value |
| Without ITT analysis | With ITT analysis |
| Total scores | | | | | |
| Initial score | 116.2 (34.6) | 125.8 (43.3) | 0.339 | | |
| A | 16.2 (11.3) | 10.6 (9.4) | 0.047* | | |
| B | 27.4 (12.9) | 17.1 (12.5) | 0.005** | 0.008** | 0.021* |
| C | 34.7 (17.4) | 21.8 (14.9) | 0.009** | | |
| D | 35.3 (25.6) | 25.6 (17.8) | 0.086 | | |
| Upper extremity | | | | | |
| Motor function | | | | | |
| Shoulder/elbow/wrist | | | | | |
| Initial score | 19.3 (13.5) | 17.5 (14.8) | 0.607 | | |
| A | 3.8 (5.1) | 2.5 (4.1) | 0.306 | | |
| B | 6.7 (7.3) | 3.3 (4.0) | 0.053 | 0.124 | 0.425 |
| C | 7.9 (8.2) | 5.3 (6.0) | 0.219 | | |
| D | 6.9 (7.8) | 7.1 (7.6) | 0.920 | | |
| Wrist | | | | | |
| Initial score | 3.8 (3.8) | 3.4 (4.2) | 0.734 | | |
| A | 1.2 (1.7) | 0.9 (1.8) | 0.540 | | |
| B | 2.4 (2.7) | 0.9 (1.8) | 0.018* | < 0.001*** | 0.026* |
| C | 3.0 (2.8) | 1.3 (2.0) | 0.024* | | |
| D | 3.4 (3.0) | 1.2 (2.1) | 0.010* | | |
| Hand | | | | | |
| Initial score | 4.8 (4.8) | 5.1 (6.0) | 0.852 | | |
| A | 2.0 (2.5) | 0.7 (1.3) | 0.025* | | |
| B | 2.9 (3.5) | 1.0 (1.6) | 0.020* | < 0.001*** | < 0.001*** |
| C | 4.6 (3.9) | 1.4 (2.2) | 0.002** | | |
| D | 4.7 (4.1) | 2.1 (2.7) | 0.016* | | |
| Coordination and speed | | | | | |
| Initial score | 1.8 (2.0) | 1.7 (2.2) | 0.941 | | |
| A | 1.2 (1.4) | 0.5 (1.1) | 0.038* | | |
| B | 1.7 (1.9) | 0.8 (1.5) | 0.044* | 0.002*** | 0.067 |
| C | 2.5 (2.0) | 1.1 (1.6) | 0.017* | | |
| D | 2.5 (2.1) | 1.3 (1.8) | 0.049* | | |
| Lower extremity | | | | | |
| Motor function | | | | | |
| Hip/knee/ankle | | | | | |
| Initial score | 12.1 (7.7) | 12.0 (8.0) | 0.948 | | |
| A | 2.8 (2.8) | 2.1 (2.8) | 0.344 | | |
| B | 4.4 (3.0) | 3.4 (3.7) | 0.312 | 0.436 | 0.767 |
| C | 6.1 (4.6) | 5.0 (5.2) | 0.457 | | |
| D | 7.2 (5.2) | 5.7 (5.6) | 0.384 | | |
| Coordination and speed | | | | | |
| Initial score | 2.1 (2.4) | 2.0 (2.4) | 0.825 | | |
| A | 0.9 (1.5) | 0.7 (1.4) | 0.725 | | |
| B | 1.5 (1.9) | 1.1 (1.5) | 0.433 | 0.861 | 0.930 |
| C | 1.8 (2.0) | 2.0 (2.0) | 0.707 | | |
| D | 2.4 (2.1) | 2.4 (2.2) | 0.984 | | |
| Balance | | | | | |
| Initial score | 5.5 (4.5) | 5.3 (4.1) | 0.902 | | |
| A | 2.7 (2.7) | 2.6 (2.3) | 0.904 | | |
| B | 4.9 (3.0) | 3.9 (2.8) | 0.220 | 0.584 | 0.933 |
| C | 5.6 (3.1) | 4.7 (3.7) | 0.365 | | |
| D | 6.1 (3.5) | 5.1 (4.3) | 0.416 | | |
| Sensation | | | | | |
| Initial score | 25.2 (23.1) | 35.4 (35.2) | 0.175 | | |
| A | 1.2 (3.9) | 0.7 (2.0) | 0.633 | | |
| B | 2.8 (3.7) | –0.9 (16.3) | 0.233 | 0.809 | 0.444 |
| C | 2.6 (4.0) | 1.7 (2.8) | 0.339 | | |
| D | 2.9 (4.2) | 2.1 (3.1) | 0.530 | | |
| Range of motion | | | | | |
| Initial score | 41.7 (8.2) | 43.4 (1.5) | 0.266 | | |
| A | 0.2 (1.8) | –0.2 (1.1) | 0.302 | | |
| B | 0.2 (1.6) | –0.1 (1.3) | 0.556 | 0.536 | 0.660 |
| C | 0.7 (2.2) | –0.7 (1.8) | 0.029* | | |
| D | –0.6 (5.5) | –1.3 (2.6) | 0.573 | | |
| *p< 0.05, **p< 0.01, ***p< 0.005. Time point: A = 2 weeks after treatment; B = 4 weeks after treatment; C = 3 months after stroke; D = 6 months after stroke. ITT: intention to treat; SD: standard deviation. |
For FIM score, no significant difference was demonstrated for the pre-treatment FIM scores between the 2 groups (Table III). For the total FIM scores, greater improvement was observed in the study group compared with the control group at 2 (15.0 vs 10.8) and 4 weeks after treatment (25.2 vs 19.7) and 3 (37.6 vs 27.4) and 6 months after stroke (44.0 vs 30.5). However, improvement did not differ statistically comparing the 2 groups, except for social cognition at 2 weeks after treatment, where significant improvement was demonstrated comparing the study group to the controls (1.2 vs 0.1; p = 0.012). Although repeated measurement ANOVA without ITT showed significant group × time interaction effect in total FIM scores and self-care functional independence, with ITT showed no significant interaction effect. There was also no significant group × time interaction effect in FIM scores by classification of motor and social-cognition function.
| Table III. Initial score and improvement in FIM after treatment. |
| Time point | Study group mean (SD) | Control group mean (SD) | p-value | Repeated measurement ANOVA p-value |
| Without ITT analysis | With ITT analysis |
| Total scores | | | | | |
| Initial score | 59.0 (27.4) | 60.7 (27.4) | 0.782 | | |
| A | 15.0 (9.8) | 10.8 (8.6) | 0.091 | | |
| B | 25.2 (12.9) | 19.7 (15.9) | 0.184 | 0.021* | 0.148 |
| C | 37.6 (18.9) | 27.4 (22.1) | 0.099 | | |
| D | 44.0 (19.1) | 30.5 (24.5) | 0.054 | | |
| Self-care | | | | | |
| Initial score | 16.3 (11.0) | 17.4 (9.9) | 0.671 | | |
| A | 6.3 (4.4) | 5.1 (4.8) | 0.328 | | |
| B | 10.6 (6.3) | 8.1 (6.2) | 0.164 | 0.033* | 0.097 |
| C | 15.1 (8.2) | 10.3 (8.1) | 0.054 | | |
| D | 16.9 (8.9) | 11.8 (9.4) | 0.076 | | |
| Sphincter control | | | | | |
| Initial score | 6.3 (3.8) | 6.0 (3.7) | 0.776 | | |
| A | 1.7 (2.0) | 1.6 (1.4) | 0.688 | | |
| B | 2.6 (2.3) | 2.6 (2.1) | 0.903 | 0.680 | 0.944 |
| C | 4.5 (2.9) | 4.0 (2.7) | 0.513 | | |
| D | 5.2 (3.0) | 4.3 (2.9) | 0.330 | | |
| Mobility | | | | | |
| Initial score | 8.4 (5.3) | 8.9 (5.3) | 0.688 | | |
| A | 3.1 (2.2) | 2.0 (1.9) | 0.051 | | |
| B | 5.0 (2.6) | 3.8 (2.9) | 0.097 | 0.116 | 0.402 |
| C | 7.1 (3.6) | 5.2 (3.7) | 0.101 | | |
| D | 8.2 (3.7) | 6.0 (4.2) | 0.079 | | |
| Locomotion | | | | | |
| Initial score | 4.1 (3.6) | 4.1 (3.0) | 0.960 | | |
| A | 1.9 (2.3) | 1.8 (2.7) | 0.825 | | |
| B | 4.0 (2.7) | 3.1 (3.3) | 0.311 | 0.109 | 0.448 |
| C | 5.8 (3.6) | 4.8 (3.6) | 0.356 | | |
| D | 7.1 (3.3) | 5.3 (3.7) | 0.093 | | |
| Communication | | | | | |
| Initial score | 9.7 (3.6) | 9.6 (4.8) | 0.931 | | |
| A | 0.9 (1.2) | 0.3 (1.8) | 0.193 | | |
| B | 1.2 (1.5) | 1.2 (3.1) | 0.998 | 0.175 | 0.398 |
| C | 2.1 (2.0) | 1.5 (4.0) | 0.498 | | |
| D | 2.7 (2.1) | 1.5 (4.0) | 0.207 | | |
| Social cognition | | | | | |
| Initial score | 13.9 (5.5) | 14.6 (6.5) | 0.647 | | |
| A | 1.2 (1.4) | 0.1 (1.6) | 0.012* | | |
| B | 1.8 (2.1) | 1.0 (3.4) | 0.312 | 0.072 | 0.123 |
| C | 3.1 (3.2) | 1.6 (4.8) | 0.208 | | |
| D | 4.0 (3.3) | 1.8 (5.1) | 0.102 | | |
| *p < 0.05. Time point: A = 2 weeks after treatment; B = 4 weeks after treatment; C = 3 months after stroke; D = 6 months after stroke. FIM: Functional Independence Measure; ITT: intention to treat; SD: standard deviation. |
Because the baseline comparability between the 2 groups is not complete (more women in the study group and smoker in the control group), we performed stratified analysis by sex and by smoking (group comparison limited to subjects of the same sex, and of the same smoking status, respectively) and reached the same conclusion (the FMA scores improved significantly in the study group, especially in the upper-limb motor performance; while there was no significant difference in FIM improvement between the 2 groups).
Discussion
Using FMA for the motor-status evaluation, our result showed that EA is effective in patients with first-ever ischaemic stroke for motor recovery, especially for upper-extremity motor recovery, including motor function of the wrist and hand. To our knowledge, this is the first study to demonstrate that EA has beneficial effects on upper limb motor performance in patients with first-ever ischaemic stroke.
In terms of functional improvement assessed by FIM, both the study group and the control group showed improvement in functional performance at 4 follow-up assessments. Although there was a tendency that the study group was superior to the control group in the total scores at 4 follow-up stages, it did not reach statistical significance. A type II error could have occurred with the FIM as the numbers in the trial was relatively small. Our result was compatible with the previous study by Hu et al. (12) and indicated that EA has no additional effects on the independence of functional performance in first-ever ischaemic stroke patients.
Why did the significantly greater improvement in upper limb motor performance not result in better functional independence in the study group? Possible reasons are: (i) the improvement in the upper motor performance (impairment level) was not enough to improve the functional performance (disability level) in patients after first-ever ischaemic stroke (22); (ii) learned non-use (23) and compensatory behaviours (24) may affect the actual hand and upper limb functional integrity; (iii) assessments focused on the upper limb functional performance rather than FIM may be more sensitive to the actual performance of upper limb; and (iv) due to high coherence among family members in traditional Chinese culture (25), disabled people were well cared for by families even when they had good motor performance.
The more detailed scoring system of FMA in upper extremity (maximum of 66) compared with lower extremity (maximum of 34) may result in better detection of the subtle change of upper extremity performance (21). This may also partly explain that the significant improvement by EA was noted only for upper extremity motor function and not for lower extremity motor function.
Previous research using functional MRI has demonstrated the effects of acupuncture stimulation on the central nervous system pathway (26). Furthermore, an association between activation of specific areas within the brain cortices and corresponding acupoints stimulation has been determined (27). Acupuncture also reduces increased excitability of motor neurones connected to the paretic limb by normalization of H-recovery time in patients after stroke (11). Injection of the radioactive tracer Technitium99 showed rapid progression of the tracer along the meridian pathway with different lymphatic/vascular flow or nerve conduction rate (28, 29). If acupuncture does, in fact, facilitate motor improvement, what is the mechanism? One hypothesis is that acupuncture increases blood circulation by decreasing blood viscosity and haematocrit and fibrinogen levels, which, in turn, leads to enhanced oxygen delivery to the hypoxic penumbra (17). Another explanation is that acupuncture may be regarded as a type of sensory stimulation (10). The acupuncture needles can stimulate sensory neurones located in muscle and activate the hypothalamus and pituitary gland and other subcortical gray structure by multi-synaptic pathways through the modulation of neurotransmitters, neurohormones and neuropeptides (5, 6, 30). Therefore, the sensory stimulation produced by acupuncture can activate multiple efferent pathways that enhance the functional plasticity of the brain. The final explanation is that EA may be a kind of physical therapy having similar effects to those of functional electrical stimulation or percutaneous electrical nerve stimulation. The acupoints are generally located between or at the edge of muscles with a high density of neurovascular structures (31). Therefore, we may speculate that EA at the acupoints may stimulate muscle strength and facilitate voluntary motor control, and even normalize the muscle tone. In this way, the selected EA points in the present study could stimulate the brachioradialis muscle (Chu Chin: LI11), hand intrinsic muscle (Ho Ku: LI4), vastus lateralis muscle (Feng Shih:GB31), and peroneal muscle (Yang Ling Chuan:GB34).
Despite the fact that needle acupuncture is a somewhat invasive procedure, with complications such as needle pain, fainting, minor bleeding or infection, no side-effects were noted in the present study. Acupuncture procedure may differ depending on differences in theory and meridians, the selection of acupoints, type of acupuncture (e.g. scalp acupuncture, otopuncture, needle acupuncture, surface acupuncture, etc), with or without electrical stimulation, and the experience of the acupuncturist. To avoid individual variability in terms of technique and experience, the same qualified acupuncturist using the same acupoints performed all EA treatment procedures in the present study. A double-blind placebo-controlled clinical trial is the gold standard of research. However, this procedure is difficult to follow in an acupuncture study because the acupuncturist always knows which method is being applied, and the patient can easily distinguish between active and non-active stimulation. A placebo acupuncture needle has recently been invented, but was not available for the present study (14). Applying needles at non-acupoints and to subcutaneous/superficial tissues, at intensities below those that produce therapeutic effects or using transcutaneous electrical nerve stimulation as a placebo control, cannot eliminate the possibility of subliminal sensory stimulation and activation of various biological and physiological responses (5, 30). Therefore, the use of sham and placebo acupuncture in control groups remains controversial (5, 30). In addition, to avoid the possible placebo effects of the acupuncture itself and the acupuncturist–patient relationship (32), EA was performed with as little extra attention to the patient as possible. We also limited communication with respect to prognosis and medical condition.
Although randomization was used for this study, there were more smokers in the control group. Cigarette smoking seemed to increase the risk of death in patients with intra-cerebral haemorrhage (33), although it is not an identified prognostic factor for first-ever stroke (34). On the other hand, there were more female patients in the study group. A recent investigation of first-ever stroke demonstrated that female sex was a significant predictor of disability and handicap at 3 months post-stroke (35). However, smoking and sex did not confound the study result, since our stratified analysis revealed that FMA score improved significantly in the study group when the comparison was limited to subjects of the same sex, and of the same smoking status.
In conclusion, EA has additional beneficial effects on long-term recovery of motor function in patients after first-ever ischaemic stroke, especially in the category of upper-limb motor function, in conjunction with conventional rehabilitation. However, the improvement in upper limb motor function did not result in better functional independence. Further research, focused on EA and upper limb functional performance, is needed.
AcknowledgEments
This study was supported in part by a research grant (SKH-8302-88-4503) from the Shin Kong Wu Ho-Su Memorial Hospital, Taipei, Taiwan.
We thank Chiao Chien Chen, Tsu-Chin Li, Yu-Chun Yen, Shu-Min Lin, and Wen Huei Guo for technical support in the preparation of this article.
Potential conflicts of interest: none.
References
1. Sze FKH, Wong EMA, Yi X, Woo J. Does acupuncture have additional value to standard post stroke motor rehabilitation? Stroke 2002; 33: 186–194.
2. Mayo NE, Wood-Dauphinee S, Cote R, Durcan L, Carlton J. Activity, participation, and quality of life 6 months poststroke. Arch Phys Med Rehabil 2002; 83: 1035–1042.
3. Hsieh RL, Lein IN, Hsieh LF, Wai YW, Hsu MH, Chou YT. Study on disease classification of rehabilitation patients in eight hospitals at northern and western Taiwan. J Rehab Med Assoc Repub China 1996; 24: 35–40.
4. Marnick C. Acceptance of some acupuncture applications. JAMA 1997; 319: 1725–1727.
5. Rabinstein AA, Shulman LM. Acupuncture in clinical neurology. Neurologist 2003; 9: 137–148.
6. Li G, Cheung RTF, Ma QY, Yang ES. Visual cortical activation on fMRI upon stimulation of the vision-implicated acupoints. Neuroreport 2003; 14: 669–673.
7. Wong AMK, Su TY, Tang FT, et al. Clinical trial of electrical acupuncture on hemiplegic stroke patients. Am J Phys Med Rehabil 1999; 78: 117–122.
8. Gosman-Hedstrom G, Claesson L, Klingenstierna U, Carlsson J, Olausson B, Frizell M, et al. Effects of acupuncture treatment on daily life activities and quality of life: a controlled, prospective, and randomized study of acute stroke patients. Stroke 1998; 29: 2100–2108.
9. Johansson BB, Haker E, von Arbin M, Britton M, Langstrom G, Terent A, et al. Acupuncture and transcutaneous nerve stimulation in stroke rehabilitation: a randomized, controlled trial. Stroke 2001; 32: 707–713.
10. Johansson K, Lindgren I, Widner H, Wiklund I, Johansson BB. Can sensory stimulation improve the functional outcome in stroke patients? Neurology 1993; 43: 2189–2192.
11. Yu YH, Wang HC, Wang ZJ. The effect of acupuncture on spinal motor neuron excitability in stroke patients. Clin Med J (Taipei) 1995; 56: 258–263.
12. Hu HH, Chung C, Liu TJ, Chen RC, Chen CH, Chou P, et al. A randomized controlled trial on the treatment for acute partial ischemic stroke with acupuncture. Neuroepidemiology 1993; 12: 106–113.
13. Naeser MA, Alexander MP, Stiassny-Eder D, Galler V, Hobbs J, Bachman D. Acupuncture in the treatment of paralysis in chronic and acute stroke patients-improvement correlated with specific CT scan lesion sites. Acupuncture & Electro-Therapeutic Res Int J 1994; 19: 227–249.
14. Park J, White AR, James MA, Hemsley AG, Johnson P, Chambers J, et al. Acupuncture for subacute stroke rehabilitation: a shame-controlled, subject- and assessor-blind, randomized trial. Arch Intern Med 2005; 165: 2026–2031.
15. Paolucci S, Antonucci G, Grasso MG, Bragoni M, Coiro P, De Angelis D, et al. Functional outcome of ischemic and hemorrhagic stroke patients after inpatient rehabilitation: a matched comparison. Stroke 2003; 34: 2861–2865.
16. Jongblood L. Prediction of function after stroke: a critical review. Stroke 1986; 17: 765–776.
17. Emst E, White AR. Acupuncture as an adjuvant therapy in stroke rehabilitation? Wiener Medizinische Wochenschrift 1996; 146: 556–558.
18. Sze FK, Wong E, Or KK, Lau J, Woo J. Does acupuncture improve motor recovery after stroke? A meta-analysis of randomized controlled trials. Stroke 2002; 33: 2604–2619.
19. Pan Long Shin. Acupuncture treatment in clinical common diseases and symptoms. 2nd edn. Taiwan: Din Yeng Publishing; 1992, p. 123–135.
20. Duncan PW, Propst M, Nelson SG. Reliability of the Fugl-Meyer assessment of sensorimotor recovery following cerebrovascular accident. Phys Ther 1983; 63: 1606–1610.
21. Sanford J, Moreland J, Swanson LR, Stratford PW, Gowland C. Reliability of the Fugl-Meyer Assessment for testing motor performance in patients following stroke. Phys Ther 1993; 73: 447–454.
22. Oczkowski WJ, Barreca S. The functional independence measure: its use to identify rehabilitation needs in stroke survivors. Arch Phys Med Rehabil 1993; 74: 1291–1294.
23. Tarkka I, Pitkanen K, Sivenius J. Paretic hand rehabilitation with constraint-induced movement therapy after stroke. Am J Phys Med Rehabil 2005; 84: 501–505.
24. Roby-Brami A, Feydy A, Combeaud M, Biryukova EA, Bussel B, Levin MF. Motor compensation and recovery for reaching in stroke patients. Acta Neurol Scand 2003; 107: 369–381.
25. Ujimoto K, Nishio H, Wong P, Lam L. Cultural factors affecting self-assessment of health satisfaction of Asian Canadian elderly. In: Whall J & Fawcett J, editors. Health and culture: exploring the relationships, vol. 1, Akville, ON: Mosaic Press; 1993, pp. 229–241.
26. Wu MT, Hsieh JC, Xiong J, Yang CF, Pan HB, Chen YC, et al. Central nervous pathway for acupuncture stimulation: localization of processing with functional MR imaging of the brain-preliminary experience. Radiology 1999; 212: 133–141.
27. Cho ZH, Chung SC, Jones JP, Park JB, Park HJ, Lee HJ, et al. New findings of the correlation between acupoints and corresponding brain cortices using functional MRI. Proc Nati Acad Sci USA 1998; 95: 2670–2673.
28. Sierpina VS, Frenkel MA. Acupuncture: a clinical review. South Med J 2005: 98; 330–337.
29. Darras JC, Albarede P, deVeernejoul P. Nuclear medicine investigation of transmission of acupuncture information. Acupuncture Med 1993: 11; 22–28.
30. NIH Consensus developmental panel on acupuncture (NIH consensus conference) Acupuncture. JAMA 1988; 280: 1518–1524.
31. Helms J, editor. Acupuncture Energetics. Berkeley, CA: Medical Acupuncture Publishers; 1996.
32. So DW. Acupuncture outcomes, expectations, patient-provider relationship, and the placebo effect: implication for health promotion. Am J Public Health 2002; 92: 1662–1667.
33. Saloheimo P, Lapp T-M, Juvela S, Hillbom M. The impact of functional status at three months of long-term survival after spontaneous intracerebral hemorrhage. Stroke 2006; 37: 487–491.
34. Appelros P, Nydevik I, Viitanen M. Poor outcome after first-ever stroke: predictors for death, dependency, and recurrent stroke within the first year. Stroke 2003; 34: 122–126.
35. Di Carlo A, Lamassa M, Baldereschi M, Pracucci G, Basile AM, Wolfe CD, et al. Sex differences in the clinical presentation, resource use, and 3-month outcome of acute stroke in Europe: data from a multicenter multinational hospital-based registry. Stroke 2003; 34: 1114–1119.