APPARATUS FOR DYNAMIC BALANCE TRAINING DURING TREADMILL WALKING
Zlatko Matjačić
From the Institute for Rehabilitation, Ljubljana, Slovenia
OBJECTIVE: A presentation of a novel apparatus for dynamic balance training during treadmill walking, which was tested in a case study.
Subject: The subject was a man with incomplete chronic spinal cord injury (C5), graded D on the American Spinal Injury Association Impairment Scale.
METHODS: Following a 6-month baseline period, 4 weeks of control treatment (treadmill walking) and a subsequent 4 weeks of experimental treatment (treadmill walking assisted by the apparatus) were compared. Outcome measures were Lower Extremities Motor Score, Berg Balance Scale, 10-metre walking test and 9-minute walking test.
RESULTS: During the baseline period the changes in the outcome measures were small. After the control treatment the balance score remained unchanged, while walking speed and walking endurance increased moderately. Experimental treatment resulted in further substantial changes in balance and walking endurance scores, while further increase in walking speed was moderate. At follow-up these values were maintained. Lower Extremities Motor Scores were almost identical in all study phases.
CONCLUSION: The subject’s walking and balancing abilities improved moderately after the control treatment, while greater improvement occurred during experimental treatment. This indicates that the apparatus developed might be an important tool for facilitating dynamic balancing training during treadmill walking.
Key words: posture, gait, rehabilitation, sensory-motor re- learning.
J Rehabil Med 2007; 39: 91–94
Correspondence address: Zlatko Matjačić, Assistant Professor, Institute for Rehabilitation, Republic of Slovenia, Linhartova 51, SI-1000 Ljubljana, Slovenia.
E-mail: zlatko.matjacic@mail.ir-rs.si
Submitted June 7, 2006; accepted October 11, 2006.
INTRODUCTION
One of the major consequences of neurological disorders or diseases is impaired walking ability (1). In the last decade a philosophy of task-oriented therapy has been proposed as a result of recent findings from basic research studies on the re-organization of the impaired brain subjected to a repetitive and intense practice of various functional movements (2). New techniques, such as partial body weight supported treadmill and overground walking (3, 4), functional electrical stimulation supported gait training (5, 6) and robotized gait trainers (3, 7, 8) were developed and evaluated. While exercising with these training modalities, trainees hold onto firm supports, for example parallel bars, to provide balance and, if needed, the force required for generation of propulsion if the leg muscles are weak. Thus, dynamic balance training incorporated into walking practice is not included in current rehabilitation practice, even though it represents an important aspect of bipedal locomotion (1). The main reason for not including dynamic balance training in gait training is a lack of adequate technical solutions. However, several studies that aimed to improve balance during standing have shown that adaptation of a task-oriented training program with the use of surface and vision manipulation of sensory input (standing on foam with the eyes open or closed) significantly increased the efficacy of training compared with a task-oriented training program where the sensory input was not altered (9, 10). Similarly, treadmill walking training with both arms holding onto parallel bars provides little challenge to the sensory-motor integration responsible for balance control during walking. We hypothesize that including a dynamic balance training component in bipedal walking practice would represent an important element, which could enable a particular subject to improve further their functional gait abilities within the constraints posed by the extent of a particular neurological impairment.
In this paper we propose a novel mechanical apparatus that enables dynamic balance training during walking on a treadmill. The mechanical apparatus developed was tested in a case study with in-series design, where a selected individual with an incomplete spinal injury practiced walking on a treadmill under 2 consecutive experimental conditions: (i) using his hands to hold onto parallel bars; and (ii) using his arms for reciprocal swinging while his balance was augmented by the mechanical apparatus.
MATERIAL AND METHODS
Device
Fig. 1 shows the subject walking on a treadmill while being supported by the apparatus developed for dynamic balance training. The mechanical components are indicated in Fig. 2a. The core of the apparatus is a helical spring housed in a steel cylinder. Between the walls of the steel cylinder and the spring there is a resistance adjustment ring with a handle. By displacing the adjustment ring vertically, the stiffness of the spring can be changed in the same manner as for the apparatus we developed previously for balance training during standing (11). If the position of the adjustment ring is higher, the bending length of the spring is shorter and the spring is stiffer. Conversely, by lowering the position of the adjustment ring, the action of the spring is more compliant. The spring is connected to a vertical rod that is coupled to the horizontal rod via a simple hinge joint that allows rotation in the sagittal plane, which is the plane of progression. At the other end of the horizontal rod there is another hinge joint coupled to a leader pelvic belt via a foam rubber disc. The foam rubber disc is very compliant, allowing pelvic tilt, list and rotation within the physiological ranges that occur during normal walking (± 8 degrees). If the subject, who is walking on a treadmill, leans forward or backward (Fig. 2b) or to the side (Fig. 2c) a stabilizing force acts on the pelvis in the transverse plane with a magnitude that depends on the position of the adjustment ring. The level of the supportive force should be selected to provide just enough support to allow a subject to walk without using their arms to hold onto the parallel bars or handles and should therefore depend on the current balancing abilities of the individual.
Fig. 1. Apparatus developed for dynamic balance training during treadmill walking. The apparatus is mounted on the static part of a treadmill and attached around the waist of the walking subject. An additional arm connects the static part of the apparatus and the vertical rod, allowing inclinations of the vertical rod in the sagittal and frontal planes, while preventing rotation of the vertical rod, which would take place due to torsional compliance of the helical spring. The parallel arms of the treadmill are not shown for better clarity of presentation.

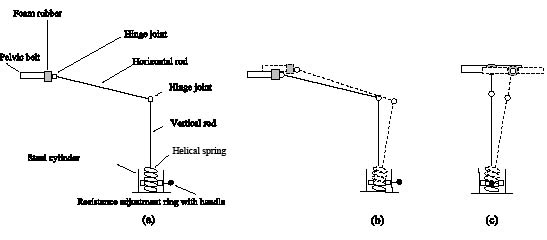
Fig. 2. (a) The apparatus developed for dynamic balance training, with mechanical components indicated. The main element of the apparatus is the helical spring that, depending on the vertical position of the adjustment ring, provides assistive forces to the pelvis of a walking subject. The action of the apparatus is shown in both principal planes of motion: (b) sagittal plane; (c) frontal plane.
Case description
The subject selected was a 32-year-old man with traumatic spinal cord injury (C5 level, 13 months post-injury). After surgical intervention he was admitted to the rehabilitation clinic and had completed a 7-month inpatient rehabilitation program. This subject’s injury was classified at the beginning of inpatient rehabilitation program as American Spinal Injury Association (ASIA) Impairment Scale C with lower-extremity motor score 20/50 (left extremity 3/25, right extremity 17/25). After completion of the inpatient rehabilitation program he was classified as ASIA D Impairment Scale with lower-extremity motor score 34/50 (left extremity 13/25, right extremity 21/25). At discharge the subject was able to walk with the aid of 2 crutches that were used mainly due to poor dynamic balance abilities – Berg Balance Scale (BBS) 37/55. He completed a 10-metre walking test in 19 seconds and could cover distance of 240 m in the 9-min walking test. Six months after completion of the inpatient rehabilitation program he returned for restorative rehabilitation of walking as an outpatient. His main goals were to improve walking ability, balance and endurance. The subject gave informed consent for the case study, which was approved by the Slovenian national ethics committee.
Study design and training procedures
A single-subject in-series design was used. A 6-month period from discharge and beginning of the study was used as a baseline period where the subject did not receive any treatment. During the first 4 weeks of restorative rehabilitation the subject practiced treadmill walking, during which he used his upper extremities for holding onto parallel bars (control treatment). A motorized treadmill (EN-TREND REHA, Enraf Nonius, Rotterdam, The Netherlands) was used. No partial body weight support was provided during the course of training. In total 16 training sessions (4 sessions per week) that lasted for 20 min with the belt speed set to around 1.2 km/h were completed. During the second 4 weeks of restorative rehabilitation the subject practiced treadmill walking where the apparatus developed for dynamic balance training was used (experimental treatment). The subject was not allowed to hold onto parallel bars, but was encouraged to perform reciprocal swinging of the upper extremities. The level of mechanical support was adjusted during the course of training to levels that enabled the subject to practice successfully without using the upper extremities for providing either balancing or propulsive forces. Also in this second period a total of 16 training sessions (4 sessions per week) that lasted for 20 min with the belt speed set to 1.2 km/h were completed.
Outcome measures
The BBS, 10-metre walking test and 9-min walking test were selected as outcome measures. The BBS is a standardized, reliable assessment tool for measuring a person’s balance during stance and transfers and was used previously in spinal cord injured population (12). It contains 14 sitting and standing tasks rated on a scale of 0 to 4 for each task. Rating is based on the time or distance requirements, supervision required and need for external support. The highest attainable score of balance function is 56. The 10-metre walking test is a simple, reliable, valid and correlates well with balance function (13). The 9-min walking test is predominantly used to determine gait endurance (13). The outcome measures were assessed 6 months prior to the beginning of the study (test 0), at the beginning (test 1), after 2 weeks of control treatment (test 2), at the end of control treatment and at the beginning of experimental treatment (test 3), after 2 weeks of experimental treatment (test 4), at the end of experimental treatment (test 5) and additionally at 1-month follow-up (test 6). Also, 6 months prior to initiation of the study (test 0), at the beginning (test 1) and at the end of training (test 5) Lower Extremity Motor Scores (LEMS) were assessed according to ASIA guidelines (14).
RESULTS
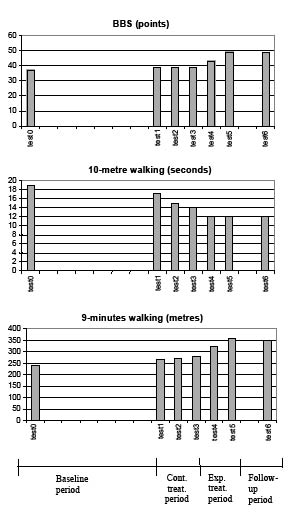
Fig. 3 shows the results for the BBS, 10-metre walking test and 9-min walking test. During the 6-month baseline period BBS increased from 37 to 39 points. The next 2 measurements taken at test 2 and at test 3 showed no change. The next 2 measurements, taken test 4 and at test 5, showed an increase to 43 and 49 points, respectively. This increase in BBS was maintained at test 6. The results of the 10-metre walking test showed a decrease from the initial 19 seconds (test 0) to 17 seconds (test 1) for the baseline period. The next 2 measurements showed further decrease; 15 seconds at test 2 and 14 seconds at test 3. At test 4 the time to complete the test decreased to 12 seconds and the remaining 2 weeks of experimental training did not change this result (test 5), indicating that a plateau in subject’s performance in terms of maximum walking speed was reached. This value was retained at test 6. Covering 10 m in 12 seconds corresponds to a walking speed of approximately 3 km/h. At test 0 the subject could cover the distance of 240 metres, corresponding to an average walking speed of 1.6 km/h in the 9-min walking test. At test 1 this result was increased to 265 m (1.76 km/h). At test 2 this distance was increased to 270 m and following the last 2 weeks of control treatment (test 3) the distance covered was 280 m (1.86 km/h). At test 4 the distance increased to 320 m and at test 5 the subject could cover 360 m, which corresponds to an average walking speed of 2.4 km/h. LEMS test results at test 0 were 34/50 (left leg 13/25, right leg 21/25), at test 1, which was performed prior to the study initiation, 35/50 (left leg 14/25, right leg 21/25), and at test 5, 35/50 (left leg 14/25, right leg 21/25).
Fig. 3. Results for Berg Balance Scale (BBS), 10-metre walking test and 9-minute walking test for the assessments taken in the distinctive study phases, as indicated on the time line.
DISCUSSION
This paper describes a novel mechanical apparatus that can be used for dynamic balance training during treadmill walking. The apparatus provides an adjustable level of supportive forces acting at the level of pelvis that enable a walking subject to let go of the parallel bars, thus creating training conditions in which a subject must progressively, as the level of support is decreased, exercise appropriate balancing activity in order to exercise stable treadmill walking. This single-subject, in-series case study has provided indications that the developed walking training paradigm may be useful in treadmill walking training for the rehabilitation of neurological individuals and that it may add a valuable training component, being practicing of dynamic balancing abilities that are an essential component of bipedal walking.
The results of the case study are interesting in several aspects. Firstly, the comparison of the results for the BBS, 10-metre walking test and 9-min walking test at the beginning and at the end of the baseline period show a slight increase in performance, which can be attributed partly to spontaneous recovery (period from 7th to 13th months after the injury) as it is currently believed that the major improvement due to spontaneous recovery will be within the first year after the injury (12). The results during and at the end of control treatment, show some improvement in the 10-metre walking test, only limited improvement in the 9-min walking test, and no improvement in the BBS. Conversely, the results during and at the end of the experimental treatment show marked improvement in the BBS and the 9-min walking test, while the results of the 10-metre walking test show a plateau in the subject’s performance. If we consider also the result of LEMS, which showed no change in muscle strength, we may argue that the observed improvement in the selected subject must have occurred due to a combined treadmill walking and dynamic balance training during walking practice. Several randomized controlled trials that compared the effects of a task-oriented exercise program on postural stability with and without altered sensory input have shown that task-oriented training combined with sensory manipulation (standing on foam instead of a firm surface with the eyes open or closed) was more effective (9, 10). Another randomized controlled trial involving people with Parkinson’s disease that included a balance recovery task into treadmill walking training by means of unexpectedly turning off and on the treadmill, thus challenging postural control, have demonstrated a significant improvement in postural control in the experimental group (15). In the light of the studies cited, it is not surprising that a 1-month control treatment did not lead to any improvement in the BBS, as when the subject was holding with both hands onto parallel bars the need for balancing activity was eliminated. On the other hand, when enabling a subject to release the parallel bars, a true bipedal walking task was practiced. Under these training conditions the subject needed to integrate the sensory information coming from the proprioceptive, vestibular and visual inputs and shape motor patterns accordingly in order to provide stable walking. In this way the experimental treatment conditions and the developed apparatus presumably enabled the subject to reorganize sensory-motor interaction, which is essential for dynamic balance during walking (1), within the limits of the injury and thus markedly improve their overall walking performance. Additionally, improvement in BBS indicates that dynamic balance training during walking is potentially a very useful training task that can also transfer to improved balance during standing and stepping, while improvement in standing balance does not necessarily transfer to walking (16). The subject selected for this case study was particularly suitable because, despite the apparent asymmetry between his left and right leg strength, the main difficulty he experienced during walking was poor balance. At the end of the study and at follow- up he did not need crutches for walking.
While the results of this case study are very encouraging it is not possible to draw firm conclusions about the presumed efficacy of the developed walking training. Since the control treatment also induced some improvement, it could be argued that this initial control treatment period enabled clinically significant improvement that appeared at the end of the experimental treatment and at follow-up. However, the high apparent correlation between the BBS scores and the increase in the 9-min walking test scores at tests 4 and 5 suggests that it was probably the improved dynamic balancing ability that this subject acquired during experimental treatment that brought about a significant increase in walking performance, given that the strength of his lower limbs did not change throughout the treatment period. The findings of this case study warrant a parallel randomized controlled trial, which could provide more a definitive conclusion about treadmill-based dynamic balance training during walking.
ACKNOWLEDGEMENTS
The author thanks the volunteer subject who participated in this study and Janez Špoljar, PT, who managed the treatment procedures. The financial support of the Agency for Research, Republic of Slovenia (contract P2-0228) is acknowledged.
REFERENCES
1. Sudarsky L. Neurologic disorders of gait. Curr Neurol Neurosci Rep 2001; 1: 350–356.
2. Liepert J, Bauder H, Wolfgang HR, Miltner WH, Taub E, Weiller C. Treatment-induced cortical reorganisation after stroke in humans. Stroke 2000; 31: 1210–1216.
3. Hesse S. Locomotor therapy in neurorehabilitation. NeuroRehabilitation 2001; 16: 1–7.
4. Barbeau H, Norman K, Fung J, Visintin M, Ladouceur M. Does neurorehabilitation play a role in the recovery of walking in neurological populations? Ann NY Acad Sci 1998; 860: 377–392.
5. Hesse S, Maležič M, Schaffrin A, Mauritz KH. Restoration of gait by combined treadmill training and multichannel electrical stimulation in non-ambulatory hemiparetic patients. Scand J Rehabil Med 1995; 27: 199–204.
6. Cikajlo I, Matjačić Z, Bajd T. Development of a gait re-education system in incomplete spinal cord injury. J Rehabil Med 2003; 35: 213–216.
7. Teasell RW, Bhogal SK, Foley NC, Speechley MR. Gait retraining post stroke. Top Stroke Rehabil 2003; 10: 34–65.
8. Wirz M, Zemon DH, Rupp R, Scheel A, Colombo G, Dietz V, et al. Effectiveness of automated locomotor training in patients with chronic incomplete spinal cord injury: a multicenter trial. Arch Phys Med Rehabil 2005; 86: 672–680.
9. Hu MH, Woollacott MH. Multisensory training of standing balance in older adults: I. Postural stability and one-leg stance balance. J Gerontol 1994; 49: M52–M61.
10. Bayouk J-F, Boucher JP, Leroux A. Balance training following stroke: effects of task-oriented exercises with and without altered sensory input. Int J Rehab Res 2006; 29: 51–59.
11. Matjačić Z, Hesse S, Sinkjaer T. BalanceReTrainer: a new standing-balance training apparatus and methods applied to a hemiparetic subject with a neglect syndrome. NeuroRehabilitation 2003; 18: 251–259.
12. Behrman AL, Harkema SJ. Locomotor training after human spinal cord injury: a series of case studies. Phys Ther 2000; 80: 688–700.
13. Wade DT, editors. Measurement in neurological rehabilitation. Oxford: Oxford University Press; 1992.
14. Maynard FM Jr, Bracken MB, Creasey G, Ditunno JF Jr, Donovan WH, Ducker TB, et al. International standards for neurological and functional classification of spinal cord injury. American Spinal Injury Association. Spinal Cord 1997; 35: 266–274.
15. Protas EJ, Mitchell K, Williams A, Qureshy H, Caroline K, Lai EC. Gait and step training to reduce falls in Parkinson’s disease. NeuroRehabilitation 2005; 20: 183–190.
16. Winstein CJ, Gardner ER, McNeal DR, Barto PS, Nicholson DE. Standing balance training: effect on balance and locomotion in hemiparetic adults. Arch Phys Med Rehabil 1989; 70: 755–762.

