USE OF INTERNATIONAL CLASSIFICATION OF FUNCTIONING, disability AND HEALTH (ICF) TO DESCRIBE PATIENT-REPORTED DISABILITY IN MULTIPLE SCLEROSIS AND IDENTIFICATION OF RELEVANT ENVIRONMENTAL FACTORS
Fary Khan, RACP1 and Julie F. Pallant, PhD2
From the 1Department of Rehabilitation Medicine, University of Melbourne Neurological Rehabilitation Physician – Royal Melbourne Hospital Melbourne and 2Faculty of Life and Social Sciences, Swinburne University of Technology, Melbourne, Hawthorn, Australia
OBJECTIVE: To use the International Classification of Functioning, Disability and Health (ICF) to describe patient-reported disability in multiple sclerosis and identify relevant environmental factors.
METHODS: Cross-sectional survey of 101 participants in the community. Their multiple sclerosis-related problems were linked with ICF categories (second level) using a checklist, consensus between health professionals and the “linking rules”. The impact of multiple sclerosis on health areas corresponding to 48 ICF categories was also assessed.
RESULTS: A total of 170 ICF categories were identified (mean age 49 years, 72 were female). Average number of problems reported was 18. The categories include 48 (42%) for body function, 16 (34%) body structure, 68 (58%) activities and participation and 38 (51%) for environmental factors. Extreme impact in health areas corresponding to ICF categories for activities and participation were reported for mobility, work, everyday home activities, community and social activities. While those for the environmental factors (barriers) included products for mobility, attitudes of extended family, restriction accessing social security and health resources.
CONCLUSION: This study is a first step in the use of the ICF in persons with multiple sclerosis and towards development of the ICF Core set for multiple sclerosis from a broader international perspective.
Key words: ICF, disability, multiple sclerosis, outcome assessment.
J Rehabil Med 2007; 39: 63–70
Correspondence address: Fary Khan, Department of Rehabilitation Medicine, University of Melbourne, Neurological Rehabilitation Physician – Royal Melbourne Hospital, Poplar Road Parkville, Melbourne VIC 3052, Australia.
E-mail: fary.khan@mh.org.au
Submitted November 21, 2005; accepted July 4, 2006.
Introduction
Multiple sclerosis (MS) is a chronic, often progressive, disease of the central nervous system. Its worldwide prevalence is estimated as 1–2.5 million cases (1). There are approximately 15,000 persons with MS in Australia (2) and it is the third leading cause of disability in adults between 20 and 50 years of age (3).
The demyelinating lesions in MS can produce disability and functional limitation with significant impact on the everyday life of persons with MS and their caregivers. The symptoms are varied and include fatigue, visual, motor and sensory deficits, bladder and bowel impairment, cognitive dysfunction and pain (4). Rehabilitation is an effective element in the overall management of MS (1, 5) and can minimize limitation in activity and restriction in participation (6, 7).
Environmental factors make up the physical, social and attitudinal environment in which people live their lives. These are external to the person, but interact with health conditions at all levels (body structure and function, everyday activities and participation in society) (8). These factors are common to all people (disabled or not), and interact with individual health conditions in unique ways to produce different disability outcomes (9). These physical, attitudinal and policy barriers can impact on activity and restrict participation in a person with MS, and need to be identified. The adaptation of the environment could then meet the unique needs of people with MS.
The International Classification of Functioning, Disability and Health (ICF) provides a framework of disability and functioning with different perspectives of health from a biological, individual and social perspective (8). ICF checklists have been used to identify patient problems in chronic conditions and in acute hospitals (10, 11). The concepts within health status measures have been linked with ICF categories using linking rules (12). Furthermore, core sets have been developed for many conditions (e.g. stroke) (13), for use in clinical studies and to guide multidisciplinary assessments. No studies in MS have used the ICF framework to describe patient disability. It is important to link the ICF categories with the perspective and experience of the person living with MS in terms of their reported limitation in activity and restriction in participation.
The objective of this study was to link patient-reported disability in an MS community cohort with ICF categories using a checklist and to identify relevant environmental factors. A further aim was to assess the impact of MS on specific health areas corresponding to ICF categories. The results of this study provide information regarding relevant health areas for persons with MS and these may serve to introduce the Australian perspective to the development of the ICF core sets for MS.
MethodS
Participants and setting
This study included a cross-sectional survey of persons residing in the community with a confirmed diagnosis of MS. These participants were identified from the MS database at the Royal Melbourne Hospital (RMH), a tertiary referral centre in Victoria, Australia. Persons on this database were recruited through the Multiple Sclerosis Society of Victoria, public and private neurology clinics across Victoria. All participants in this database were reviewed by a neurologist who confirmed diagnosis using diagnostic criteria (14, 15), the stage of MS (relapsing remitting, secondary or primary progressive, and relapsing remitting secondary progressive (overlapping) stage), and severity of disease using Expanded Disability Status Scale (EDSS) (16).
Participants selected for this study needed to reliably report the main problems in living with MS. They were between 18 and 65 years of age, with a confirmed diagnosis of MS, residing in the community (area of greater Melbourne <60 km radius), who had known limitations in their neurological status (including mobility) and EDSS scores between 2 and 7.5 and cognition (Kurtze Functional System (KFS) score between 0 and 2) (16). Participants with severe cognition deficits (KFS greater than 2), and those who were institutionalized and/or bedbound were excluded.
This study was approved by the University of Melbourne and the RMH, Human Research and Ethics Committees.
Data collection
At the time of recruitment 204 (20%) of 1023 patients listed on the RMH MS Database were eligible for this study due to entry criteria (Fig. 1). All were invited by post to participate in the study and the 101 who consented were recruited for the project. All interviews were conducted by trained research assistants and physicians who participated in 3 half-day structured ICF workshops at RMH. This involved education about the model and core ICF principles, and practical application of the ICF checklist.
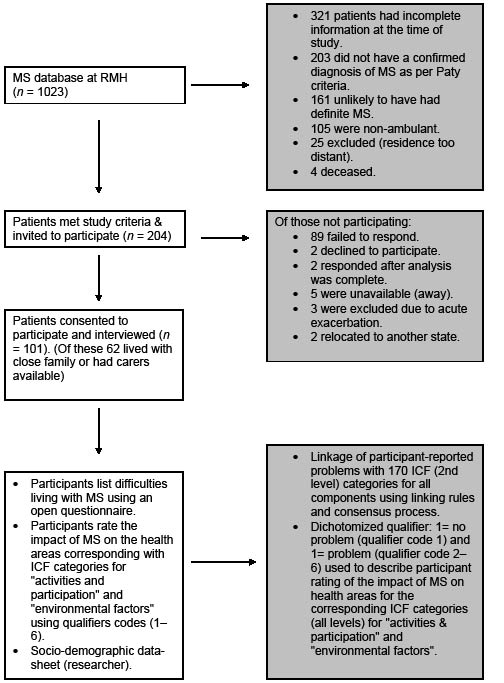
Fig. 1. Recruitment process. MS: multiple sclerosis; RMH: Royal Melbourne Hospital; ICF: International Classification of Functioning, Disability and Health.
Measures
Each participant was interviewed using a structured format and asked to nominate a list of the problems affecting their everyday life due to MS (available from authors). There was no prompting or use of MS problem lists. The information provided was checked and clarified with the patient medical record, RMH database and where possible with carers. Any discrepancies were resolved with discussion (with the participant) and consensus agreement between reviewers. Each problem was then linked with the ICF checklist of 170 second-level categories from the 362 second-level categories of the whole ICF classification system. This checklist incorporated the 125 categories in the World Health Organization (WHO) checklist (17) and another 45 added ICF categories that linked with participant answers (available from authors). With regards to all categories in the second level of the ICF, this checklist included 48 (42%) categories from the component body function, 16 (34%) from body structure, 68 (58%) from activities and participation and 38 (51%) from environmental factors.
Each participant then reviewed a checklist comprising 48 ICF categories (all levels of classification) for the 2 components of ICF categories “activities and participation” and “environmental factors”. Participants were asked whether MS had an impact in the health areas described in the corresponding ICF categories (available from authors). They rated areas of significant impact for them using a 6-point scale: 1=no impact (0%), 2=minimal (1–4%), 3=mild (5–24%), 4=moderate (25–49%), 5=severe (50–95%) and 6=extreme impact (96–100%). These correspond with the percentages for WHO ICF qualifiers 0–4 (8). We used the 6-point impact scale for improved responsiveness and sensitivity to describe the range of impact reported by participants for health areas in corresponding ICF categories, and to accommodate the fluctuating nature, paroxysmal symptoms and complexity of MS. Barriers (hindrances) were identified as a major influence on a persons’ ability to engage in activity, participation and good health practices. Impact was defined as subjectively perceived costs inherent in undertaking activity, participation and health behaviours.
Authors trained in ICF used the linking rules (12) to match each problem reported by the participant with an appropriate code from the ICF categories (second level). All problems pertaining to personal factors currently not coded within the ICF were grouped under “personal factors” (18). Consensus between health professionals was used to decide which categories should be linked to each answer. After data extraction, both reviewers compared their results. As in the report by Weigl et al. (19), any disagreements concerning selected categories and codes were resolved by a trained third health professional.
Information relating to participant socio-demographic and disease status was collated using a standard data form.
Statistical methods
Descriptive analysis was used to describe the study population. The frequency of participant-reported problems was linked with the ICF categories (second level). The stage of disease for participants corresponding with each ICF category was also reported.
We used a dichotomized qualifier: 0=no problem (qualifier code 1) and 1=problem (qualifier code 2–6) to describe participant rating of the impact of MS on 48 health areas for the corresponding ICF categories. The frequency of participants who reported limitation in the categories for the component “activities and participation” are presented. For environmental factors, the frequencies of persons reporting a specific category as a barrier are reported.
If the patient repeatedly assigned one ICF category, it was counted once only to avoid bias. Consensus opinion was used if there was a discrepancy in the MS-related problem listed by the participant and their carer. Carer report was included in the information used to link ICF categories for problems listed by the person with MS. All data was entered twice to avoid errors on data entry. SPSS 11.0 for Windows was used for analysis.
RESULTS
The socio-demographic and disease characteristics of the 101 participants with MS are shown in Table I. The number of problems reported by the participants with MS ranged from 8 to 30 (mean 18). Twenty-six carers reported at least 2 additional problems compared with participant report (to be presented in a separate paper). There was 100% agreement between reviewers for linkage of participant-reported problems with the ICF categories.
| Table I. Characteristics of participants with multiple sclerosis | |
| Characteristic | Average/frequency |
| Age, years (mean (SD), range) Male Female | 49.50 (9.19), 28–64 49.56 (9.11), 28–64 49.38 (9.56), 29–61 |
| Sex (n, %) Male Female | 29 (28.7) 72 (71.3) |
| Living (n, %) Alone Family Other | 24 (23.8) 71 (70.3) 6 (5.9) |
| Working (n, %) Retired/unemployed Working full-time (36 hours/week) Working part-time (20 hours/week) | 60 (59.4) 35 (34.7) 6 (5.9) |
| Pension (n, %) No Yes | 47 (46.5) 54 (53.5) |
| With permission from Lippincott, Williams and Wilkins. F. Khan, T McPhail, C. Brand, L. Turner-Stokes, T. Kilpatrick. Multiple sclerosis: disability profile and quality of life in an Australian community cohort. Int J Rehabil Res. 2006; 29: 87–96. | |
Tables II–V show the frequency of limitations in categories reported by at least one-third (33%) of the participants (for each category), linked with the ICF categories for all 4 components: “body function”, “body structure”, “activities and participation” and “environmental factors”. The frequency and participant disease stage for each category is also presented.
A total of 170 ICF categories were identified. In the component “body function”, 10 categories each were selected for mental function, and neuromuscular and movement-related functions, sensory function and pain (6 categories each) and genitourinary functions (5 categories). At least 90% of participants reported limitations in at least one of the categories of the chapters: mental function (b1), function of cardiovascular system (b4), genitourinary and reproductive function (b6), neuromuscular and movement related functions (b7).
| Table II. Frequency of limitation in the linked categories for the component body function reported by at least one-third (33%) of the participants with multiple sclerosis (n=101) | ||||||
| ICF Code | ICF Code description | Total number of participants linked responses n (%) | Number of participant and stage of disease | |||
| RR | SP | PP | rr-SP | |||
| b130 | Energy and drive functions | 98 (97.0) | 51 | 26 | 14 | 7 |
| b134 | Sleep | 84 (83.1) | 47 | 21 | 11 | 5 |
| b140 | Attention | 66 (65.3) | 37 | 17 | 9 | 3 |
| b144 | Memory | 62 (61.3) | 37 | 16 | 4 | 5 |
| b152 | Emotional functions | 97 (96.0) | 50 | 26 | 14 | 7 |
| b210 | Seeing | 47 (46.5) | 24 | 16 | 4 | 3 |
| b235 | Vestibular (incl. Balance functions) | 71 (70.3) | 34 | 19 | 13 | 5 |
| b265 | Touch* | 34 (33.6) | 15 | 10 | 7 | 2 |
| b280 | Sensation of pain | 76 (75.2) | 39 | 19 | 12 | 6 |
| B455 | Exercise tolerance functions* | 97 (96.0) | 50 | 27 | 13 | 7 |
| b525 | Defecation | 89 (88.1) | 49 | 21 | 14 | 5 |
| b620 | Urination functions | 94 (93.0) | 50 | 24 | 13 | 7 |
| b640 | Sexual functions | 57 (56.4) | 32 | 15 | 7 | 3 |
| b730 | Muscle power | 96 (95.0) | 50 | 27 | 13 | 6 |
| b735 | Muscle tone | 94 (93.0) | 50 | 26 | 13 | 5 |
| b740 | Muscle endurance function* | 93 (92.0) | 49 | 25 | 12 | 7 |
| b760 | Control of voluntary movement functions* | 66 (65.3) | 37 | 18 | 8 | 3 |
| b770 | Gait pattern functions* | 99 (98.0) | 51 | 27 | 13 | 8 |
| *Categories added to the ICF (checklist version 2.1a) (17) after linkage of participant responses. RR: relapsing remitting multiple sclerosis (MS); SP: secondary progressive MS; PP: primary progressive MS; rr-SP: relapsing remitting secondary progressive MS. | ||||||
| Table III. ICF – Frequency of limitation in the linked categories for the component body structure reported by at least one-third (33%) of the participants with multiple sclerosis (n=101) | ||||||
| ICF Code | ICF Code description | Total number of participants linked responses n (%) | Number of participant and stage of disease | |||
| RR | SP | PP | rr-SP | |||
| s110 | Brain | 100 (99.0) | 50 | 28 | 14 | 8 |
| s610 | Urinary system | 93 (92.0) | 49 | 25 | 12 | 7 |
| s730 | Upper extremity (arm, hand) | 44 (43.5) | 25 | 10 | 7 | 2 |
| s750 | Lower extremity (leg, foot) | 97 (96.0) | 49 | 27 | 14 | 7 |
| s760 | Trunk | 85 (84.1) | 44 | 23 | 12 | 6 |
| RR: relapsing remitting multiple sclerosis (MS); SP: secondary progressive MS; PP: primary progressive MS; rr-SP: relapsing remitting secondary progressive MS. | ||||||
| Table IV. ICF – Frequency of limitation in the linked categories for the component activities and participation reported by at least one-third (33%) of the participants with multiple sclerosis (n=101) | ||||||
| ICF Code | ICF Category description | Total number of participants linked responses. n (%) | Number of participant and stage of disease | |||
| RR | SP | PP | rr-SP | |||
| d160 | Focussing attention* | 70 (69.3) | 39 | 16 | 9 | 6 |
| d175 | Solving problems | 34 (33.6) | 22 | 8 | 2 | 2 |
| d177 | Making decisions* | 59 (58.4) | 35 | 16 | 5 | 3 |
| d220 | Undertaking multiple tasks | 88 (87.1) | 47 | 24 | 12 | 5 |
| d230 | Carrying out daily routine* | 80 (79.2) | 48 | 17 | 10 | 5 |
| d240 | Handling stress and other psychological demands* | 101 (100) | 51 | 28 | 14 | 8 |
| d430 | Lifting and carrying objects | 53 (52.4) | 30 | 12 | 8 | 3 |
| d440 | Fine hand use (picking up, grasping) | 51 (50.5) | 26 | 13 | 9 | 3 |
| d445 | Hand and arm use* | 37 (36.6) | 21 | 9 | 4 | 3 |
| d450 | Walking | 101 (100) | 51 | 28 | 14 | 8 |
| d455 | Moving around* | 99 (98.0) | 51 | 27 | 14 | 7 |
| d465 | Moving around and using equipment (wheelchair, skates, etc) | 98 (97.0) | 50 | 27 | 14 | 7 |
| d470 | Using transportation (car, bus, train, plane, etc) | 100 (99.0) | 51 | 27 | 14 | 8 |
| d475 | Driving (riding bicycle and motorbike, driving car, etc) | 99 (98.0) | 51 | 27 | 14 | 7 |
| d510 | Washing oneself (bathing, drying, washing hands, etc) | 41 (40.5) | 26 | 9 | 4 | 2 |
| d520 | Caring for body parts (brushing teeth, shaving, grooming, etc) | 40 (39.6) | 24 | 8 | 5 | 3 |
| d570 | Looking after one’s health | 88 (87.1) | 47 | 23 | 14 | 4 |
| d620 | Acquisition of goods and services (shopping, etc) | 92 (91.0) | 50 | 24 | 12 | 6 |
| d630 | Preparation of meals (cooking, etc) | 89 (88.1) | 48 | 24 | 12 | 5 |
| d640 | Doing housework (cleaning, washing, laundry, ironing) | 94 (93.0) | 51 | 23 | 14 | 6 |
| d650 | Caring for household objects* | 84 (83.1) | 46 | 22 | 12 | 4 |
| d660 | Assisting others | 87 (86.1) | 48 | 22 | 13 | 4 |
| d750 | Informal social relationships | 35 (34.6) | 19 | 12 | 2 | 2 |
| d760 | Family relationships | 73 (72.2) | 42 | 16 | 11 | 4 |
| d770 | Intimate relationships | 61 (60.4) | 35 | 15 | 7 | 4 |
| d845 | Acquiring keeping and terminating a job* | 73 (72.2) | 39 | 19 | 11 | 4 |
| d850 | Remunerative employment | 90 (89.1) | 45 | 24 | 13 | 8 |
| d870 | Economic self-sufficiency | 84 (83.1) | 44 | 22 | 13 | 5 |
| d910 | Community Life | 79 (78.2) | 40 | 21 | 13 | 5 |
| d920 | Recreation and leisure | 97 (96.0) | 50 | 26 | 14 | 7 |
| *Categories added to the ICF (checklist version 2.1a) (17) after linkage of participant responses. RR: relapsing remitting multiple sclerosis (MS); SP: secondary progressive MS; PP: primary progressive MS; rr-SP: relapsing remitting secondary progressive MS. | ||||||
| Table V. ICF- Frequency of limitation in the linked categories for the component Environmental factors reported by at least one third (33%) of the participants with multiple sclerosis (n=101) | ||||||
| ICF Code | ICF Code description | Total number of participants linked responses. n (%) | Number of participant and stage of disease | |||
| RR | SP | PP | rr-SP | |||
| e110 | For personal consumption (food, medicines) | 101 (100) | 51 | 28 | 14 | 8 |
| e120 | For personal indoor and outdoor mobility and transportation | 91 (90.1) | 47 | 25 | 12 | 7 |
| e150 | Design, construction and building products and technology of buildings for public use | 70 (69.3) | 39 | 18 | 9 | 4 |
| e210 | Physical geography* | 39 (38.6) | 21 | 11 | 5 | 2 |
| e225 | Climate | 99 (98.0) | 50 | 28 | 14 | 7 |
| e310 | Immediate family | 45 (44.5) | 27 | 9 | 7 | 2 |
| e315 | Extended family* | 42 (41.5) | 26 | 9 | 3 | 4 |
| e540 | Transportation services, systems and policies | 68 (67.3) | 38 | 17 | 8 | 5 |
| e580 | Health services, systems and policies | 79 (78.2) | 45 | 18 | 11 | 5 |
| *Categories added to the ICF (checklist version 2.1a) (17) after linkage of participant responses. RR: relapsing remitting multiple sclerosis (MS); SP: secondary progressive MS; PP: primary progressive MS; rr-SP: relapsing remitting secondary progressive MS. | ||||||
In the component “body structure”, 93 (92%) participants reported structure of genitourinary system (s6).
All 9 chapters of the “activities and participation” component had limitations and included 68 categories. The main areas linked: mobility (11 categories), learning and applying knowledge (10 categories), and major life areas such as employment (9 categories), and interpersonal relationships (7 categories). Thirty-eight categories in the “environment” component included: systems and policies (e5) 11 categories, 8 categories each in support and relationships (e3), and for attitudes (e4) and 6 categories for products and technology (e1). Products for personal consumption (medicines) (e1) and climate (e2) were considered relevant.
Tables VI and VII show the ICF categories for components “activities and participation” and “environmental factors”, and the frequency of MS participants-reporting impact (qualifier 1–6) for health areas corresponding with categories for 10 chapters. The most impact reported for corresponding ICF categories in the activities and participation components include: mobility, work, everyday home activities, and community and social activities. Extreme limitation was reported by 77 (77%) participants in ambulating distances > 1 kilometre, 67 (66%) involving sport, 56 (55%) in maintaining employment and 45 (45%) in accessing public transportation. In environmental factors, extreme impact (barrier) was reported by 33 (32%) participants for using products for mobility, 18 (17%) for attitudes of extended family members, 20 (20%) in accessing health resources and 19 (18%) with accessing social security services, and assistance programmes.
| Table VI. Frequency of participants reporting the impact of multiple sclerosis on health areas for corresponding ICF categories for “activities and participation” | |||||||
| Categories | ICF Code | No impact | Minimal impact | Mild impact | Moderate impact | Severe impact | Extreme impact |
| 0% | 1–4% | 5–24% | 25–49% | 50–95% | 96–100% | ||
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | ||
| Mobility | |||||||
| Changing basic body position, | d410 | 7 (6.9) | 11 (10.9) | 18 (17.8) | 15 (14.9) | 29 (28.7) | 21 (20.8) |
| Transferring oneself, transferring when sitting | d420 (d4200) | 27 (26.7) | 23 (22.8) | 18 (17.8) | 14 (13.9) | 10 (9.9) | 9 (8.9) |
| Lifting and carrying objects | d430 (d4300, 4301) | 9 (8.9) | 10 (9.9) | 14 (13.9) | 21 (20.8) | 25 (24.8) | 22 (21.8) |
| Moving around in different locations (moving within the home) | d460 (d4600) | 19 (18.8) | 20 (19.8) | 13 (12.9) | 19 (18.8) | 16 (15.8) | 14 (13.9) |
| Move outside home within the community | d460 (d4602) | 8 (7.9) | 8 (7.9) | 8 (7.9) | 12 (11.9) | 27 (26.7) | 38 (37.6) |
| Walking Walk short distances | d450 (d4500) | 9 (8.9) | 4 (4.0) | 8 (7.9) | 11 (10.9) | 12 (11.9) | 57 (56.4) |
| Walking long distances ( > 1 km) | d450 (d4501) | 3 (3.0) | 3 (3.0) | 4 (4.0) | 6 (5.9) | 8 (7.9) | 77 (76.2) |
| Driving, driving motorized vehicle | d475 (d4751) | 16 (16.2) | 17 (17.2) | 15 (15.2) | 6 (6.1) | 9 (9.1) | 36 (36.4) |
| Using transportation, using public motorized transportation | d470 (d4702) | 16 (16.0) | 9 (9.0) | 12 (12.0) | 8 (8.0) | 10 (10.0) | 45 (45.0) |
| Self care | |||||||
| Eating | d550 | 45 (44.6) | 14 (13.9) | 15 (14.9) | 9 (8.9) | 11 (10.9) | 7 (6.9) |
| Caring for body parts | d520 | 41 (40.6) | 18 (17.8) | 16 (15.8) | 8 (7.9) | 9 (8.9) | 9 (8.9) |
| Washing oneself | d510 | 43 (43.0) | 9 (9.0) | 15 (15.0) | 11 (11.0) | 12 (12.0) | 10 (10.0) |
| Dressing, upper body | d540 (d5400, 5401) | 31 (31.0) | 20 (20.0) | 19 (19.0) | 13 (13.0) | 12 (12.0) | 5 (5.0) |
| Dressing lower body | d540 (d5400, 5401) | 25 (25.0) | 17 (17.0) | 16 (16.0) | 11 (11.0) | 17 (17.0) | 14 (14.0) |
| Toileting | d530 | 50 (49.5) | 14 (13.9) | 10 (9.9) | 7 (6.9) | 9 (8.9) | 11 (10.9) |
| Wellbeing and health | |||||||
| Looking after one’s health, ensuring physical comfort | d570 (d5700) | 39 (38.6) | 19 (18.8) | 13 (12.9) | 14 (13.9) | 6 (5.9) | 10 (9.9) |
| Managing diet and fitness | d570 (d5701) | 59 (59.0) | 13 (13.0) | 8 (8.0) | 7 (7.0) | 9 (9.0) | 4 (4.0) |
| Managing one’s health | d570 (d5702) | 10 (9.9) | 7 (6.9) | 10 (9.9) | 17 (16.8) | 18 (17.8) | 39 (38.6) |
| Everyday home activities | |||||||
| Acquisition of goods & services (shopping) | d620 (d6200) | 19 (18.8) | 6 (5.9) | 13 (12.9) | 12 (11.9) | 15 (14.9) | 36 (35.6) |
| Gathering daily necessities | d620 (d6201) | 26 (25.7) | 15 (14.9) | 11 (10.9) | 16 (15.8) | 17 (16.8) | 16 (15.8) |
| Preparing meals | d630 | 28 (27.7) | 14 (13.9) | 16 (15.8) | 10 (9.9) | 17 (16.8) | 16 (15.8) |
| Interpersonal relationships | |||||||
| Intimate relationship (spouse) | d770 (d7701) | 9 (9.8) | 12 (13.0) | 14 (15.2) | 14 (15.2) | 11 (12.0) | 32 (34.8) |
| Family relationships (parent child) | d760 (d7600) | 12 (18.2) | 14 (21.2) | 12 (18.2) | 10 (15.2) | 8 (12.1) | 10 (15.2) |
| Informal social relationship with (friends) | d750 (d7500) | 21 (20.8) | 16 (15.8) | 18 (17.8) | 16 (15.8) | 15 (14.9) | 15 (14.9) |
| Formal relationships (persons with authority) | d740 (d7400) | 40 (45.5) | 11 (12.5) | 5 (5.7) | 4 (4.5) | 12 (13.6) | 16 (18.2) |
| Work | |||||||
| Acquiring, keeping terminating job | d845 | 15 (15.0) | 6 (6.0) | 10 (10.0) | 3 (3.0) | 10 (10.0) | 56 (56.0) |
| Renumerative employment | d850 | 10 (10.0) | 8 (8.0) | 8 (8.0) | 7 (7.0) | 12 (12.0) | 55 (55.0) |
| Non renumerative employment | d855 | 17 (17.2) | 13 (13.1) | 9 (9.1) | 13 (13.1) | 13 (13.1) | 34 (34.3) |
| Community and social activity | |||||||
| Recreation & leisure (hobbies) | d920 (d9204) | 14 (13.9) | 8 (7.9) | 16 (15.8) | 6 (5.9) | 14 (13.9) | 43 (42.6) |
| Recreation & leisure (sport) | d920 (d9201) | 5 (5.0) | 6 (5.9) | 4 (4.0) | 8 (7.9) | 11 (10.9) | 67 (66.3) |
| Recreation & leisure (socializing) | d920 (d9205) | 12 (11.9) | 7 (6.9) | 16 (15.8) | 15 (14.9) | 20 (19.8) | 31 (30.7) |
| Religion & spirituality (organized religion) | d930 (d9300) | 22 (50.0) | 7 (15.9) | 2 (4.5) | 6 (13.6) | 2 (4.5) | 5 (11.4) |
| Religion & spirituality (spirituality) | d930 (d9301) | 23 (48.9) | 9 (19.1) | 1 (2.1) | 6 (12.8) | 2 (4.3) | 6 (12.8) |
| ICF: International Classification of Functioning, Disability and Health. | |||||||
| Table VII. Frequency of participants reporting the impact of multiple sclerosis on health areas for corresponding ICF categories for “environmental factors” | |||||||
| ICF Code | No impact | Minimal impact | Mild impact | Moderate impact | Severe impact | Extreme impact | |
| 0% | 1–4% | 5–24% | 25–49% | 50–95% | 96–100% | ||
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | ||
| Social security & health | |||||||
| Social security systems and policies | e570 | 41 (40.6) | 9 (8.9) | 13 (12.9) | 9 (8.9) | 10 (9.9) | 19 (18.8) |
| Health services, systems & policies | e580 | 36 (36.0) | 5 (5.0) | 9 (9.0) | 15 (15.0) | 15 (15.0) | 20 (20.0) |
| Attitudes | |||||||
| Attitudes of extended family members (and friends) | e415, (e420) | 28 (27.7) | 17 (16.8) | 9 (8.9) | 15 (14.9) | 14 (13.9) | 18 (17.8) |
| Attitudes of healthcare professionals | e450 | 33 (32.7) | 20 (19.8) | 15 (14.9) | 12 (11.9) | 9 (8.9) | 12 (11.9) |
| Attitudes of persons in positions of authority | e430 | 44 (43.6) | 21 (20.8) | 17 (16.8) | 11 (10.9) | 6 (5.9) | 2 (2.0) |
| Societal attitudes | e460 | 56 (55.4) | 14 (13.9) | 8 (7.9) | 7 (6.9) | 9 (8.9) | 7 (6.9) |
| Products and technology | 31 (30.7) | 15 (14.9) | 12 (11.9) | 15 (14.9) | 9 (8.9) | 19 (18.8) | |
| Personal use daily living | e115 | 46 (45.5) | 13 (12.9) | 10 (9.9) | 11 (10.9) | 10 (9.9) | 11 (10.9) |
| Products and technology for Personal indoor /outdoor mobility | e120, (e1200) | 22 (21.8) | 8 (7.9) | 9 (8.9) | 18 (17.8) | 11 (10.9) | 33 (32.7) |
| Products and technology for personal transportation | e120, (e1201) | 50 (51.0) | 13 (13.3) | 8 (8.2) | 8 (8.2) | 7 (7.1) | 12 (12.2) |
| Products for technology for employment | e135, (e1350) | 34 (34.7) | 17 (17.3) | 9 (9.2) | 9 (9.2) | 12 (12.2) | 17 (17.3) |
| ICF: International Classification of Functioning, Disability and Health. | |||||||
Discussion
This study used “linkage rules” to link problems reported by persons with MS living in the community with the individual categories and components of ICF (body function, body structure, activities and participation and environmental factors). This linkage can identify potentially important areas in MS care, and improve our understanding of the participants’ perspective of the impact of MS in relevant areas of health described in the corresponding ICF categories. This can facilitate communication, assessment and management of these persons across settings and interventions (20).
The linkage of problems with the ICF component “body function” identified 10 categories in the mental and orientation function-energy and drive, emotional function, attention and memory. These have been previously reported in MS population (21, 22). The categories from neuromuscular and movement functions (gait, muscle tone, power and endurance) are similar to other reports (23, 24). The issues with continence, fatigue, sexuality and pain are consistent with other series (21, 25–27). Digestive (defecation) function reported by 89 participants was higher than the 70% reported for persons with MS in a recent review (28).
The categories linked with body structures refer to the long-term effects of impairments on movement-related body structures, similar to those reported for neurological patients in post-acute rehabilitation facilities (29).
MS affects all aspects of life and therefore “activities and participation” had a large number of categories represented. These include: mobility, learning and applying knowledge, domestic life, inter-personal, family and intimate relations. These areas are similar to those reported in patients with chronic conditions (stroke, diabetes, arthritis) and mental health conditions (depression) (10). Furthermore, major life areas (economic self-sufficiency, remunerative employment) were in keeping with other studies (30). Climate was an important category identified by the participants with MS. Other environmental categories linked, such as products for personal consumption (medicines), products of technology for use in daily living and for indoor/outdoor mobility, transportation and access to health services, were also reported for patients with chronic conditions (10). The limited access to healthcare services and systems was similar to that reported for patients in the acute hospital (11).
The participant report of impact of MS in the health areas described in the corresponding ICF categories for the 2 components: activities and participation and environmental factors, were as expected. The study population included active “working age” persons in the community, mostly living with family, and driving. The categories in “activities and participation” such as mobility (especially for longer distances), public transport, interpersonal relationships, home and community activities were relevant and similar to the non-MS population. In the environment list the participants reported impact of MS in health areas for corresponding ICF categories for climate, products for personal use and mobility, work, attitudes of friends and access to social security and health services, similar to those reported by neurological patients in acute hospital (11).
Environmental factors can place important restrictions on the degree to which people with MS can participate in the community. Their impact can be greater than the underlying organ system impairments in determining limitation in activity and restriction in participation. The understanding of the environmental factors from the MS participants’ perspective can help assess the barriers and facilitators as perceived by the individual. Adaptation and modification of the environment could then eliminate these barriers and improve participation (9).
Our study has some potential limitations. This is a cross-sectional survey and does not provide longitudinal information. The participants have strict inclusion criteria and are listed in a database of people with MS held at the RMH and who agreed to participate in research projects. The collection of self-report data from patients with cognitive problems, especially those with EDSS scores between 6.5 and 7.5 is challenging. However, we considered it important to include these persons, who may have very different problems and symptom experience than those less severely affected. In an attempt to reduce recall bias, all questions were limited in the main to the current situation. Medical records were used only to confirm participant report and no additional information was obtained. Wherever possible carers were invited to validate reports, however they were not always available. This method of information gathering has potential information bias. We were not able to identify and link problems with ICF categories not listed by the participants. We did not use the WHO qualifiers scale (0–4) as mentioned nor report concurrent co-morbidities, which may contribute to problems in function. The participant report is subject to interviewers’ interpretation; however, ICF categories linked were consistent with medical information available for participants. This consistency can therefore be interpreted as cross-validation of the results. The generalizability and validity of these findings need to be established in future studies.
The aim of this study was to describe the commonly reported problems in MS using the ICF to lay an empirical foundation from the Australian perspective to develop an ICF Core set for MS. This would potentially indicate areas of functional impairment, assessment and management of these persons and facilitate communication in MS care. It can also provide a broader comprehensive framework across patients, settings and interventions that contribute to research in rehabilitation practice (20). Environmental factors identified in this study need further evaluation. The results of this study represent a first step in the use and implementation of the ICF in patients with MS. Based on the experience accumulated from the ICF Core sets developed so far, an important next step would be the development of the ICF Core set for MS from a broader international perspective.
Acknowledgements
We thank all participants with MS and their carers, T. Hale for consensus and linkage, L. Spooner and C. Peros for interviews, T. McPhail for data entry, M. Tanner for assistance with RMH database and Professor T. Kilpatrick for providing access to the MS RMH database. The above-mentioned persons were informed and approve of this acknowledgement.
References
1. Atlas: country resources for neurological disorders. Results of a collaborative study of World Health Organization and World Federation of Neurology. Programme for Neurological Diseases and Neurosciences Department of Mental Health and Substance abuse. World Health Organization; Geneva; 2004. Available from: http://www.who.int/mental_health/neurology/neurology_atlas_review_references.pdf (accessed 27/6/2006).
2. MS Australia. Available from: http://www.msaustralia.org.au (accessed 27/6/06).
3. Dombovy ML. Multiple sclerosis and Parkinsons Disease Rehabilitation. In: Lazar R, ed. Principles of neurological rehabilitation. New York: McGraw-Hill; 1998, p. 173–197.
4. Kraft GH, Cui JY. Multiple sclerosis. In: DeLisa JA, Gans BM, Walsh NE, eds. Physical medicine and rehabilitation: principles and practice, fourth edition. Philadelphia: Lippincott Williams & Wilkins; 2005; 2, p. 1753–1769.
5. Kraft GH. Rehabilitation still the only way to improve function in multiple sclerosis. Lancet 1999; 354: 2016–2017.
6. Freeman JA, Langdon DW, Hobart JC, Thompson AJ. Inpatient rehabilitation in multiple sclerosis: do the benefits carry over into the community? Neurology 1999; 52: 50–56.
7. Patti F, Ciancio MR, Cacopardo M, Reggio E, Fiorilla T, Palermo F, et al. Effects of a short outpatient rehabilitation treatment on disability of multiple sclerosis patients – a randomised controlled trial. J Neurol 2003; 250: 861–866.
8. World Health Organization. International Classification of Functioning, Disability, and Health (ICF). Geneva: WHO; 2001.
9. Whiteneck GC, Harrison-Felix CL, Mellick DC, Brooks CA, Charlifue SB, Gerhart KA. Quantifying environmental factors: a measure of physical, attitudinal service, productivity and policy barriers. Arch Phys Med Rehabil 2004; 85: 1324–1336.
10. Ewert T, Fuessl M, Cieza A, Anderson C, Chatterji S, Kostanjsek N, et al. Identification of the most common patient problems in patients with chronic conditions using the ICF checklist. J Rehabil Med 2004; 36 (suppl 44): 22–29.
11. Grill E, Huber EO, Stucki G, Herceg M, Fialka-Moser V, Quittan M. Identification of relevant ICF categories by patients in the acute hospital. Disabil Rehabil 2005; 27: 447–458.
12. Cieza A, Geyh S, Chatterji S, Kostanjsek N, Ustun B, Stucki G. ICF Linking rules: an update based on lessons learned. J Rehabil Med 2005; 37: 212–218.
13. Geyh S, Cieza A, Schouten J, Dickson H, Frommelt P, Omar Z, et al. ICF Core sets for Stroke. J Rehabil Med 2004; 36 (suppl 44): 135–141.
14. Poser CM, Paty DW, Scheinberg L, McDonald WI, Davis FA, Ebers GC, et al. New diagnostic criteria for multiple sclerosis: guidelines for research protocols. Ann Neurol 1983; 3: 227–231
15. Paty DW, Oger JJ, Kastrukoff LF, Hashimoto SA, Hooge JP, Eisen AA, et al. MRI in the diagnosis of MS: a prospective study with comparison of clinical evaluation, evoked potentials, oligoclonal banding and CT neurology. Neurology 1988; 38: 180–185.
16. Kurtzke JF. Rating neurological impairment in multiple sclerosis: an Expanded Disability Status Scale (EDSS). Neurology 1983; 33: 1444–1452.
17. The World Health Organization. ICF Checklist Version 2.1a, Clinical Form for International Classification of functioning, Disability and Health: ICF. Geneva: WHO; 2001. Available from: http://www3.who.int/icf/icftemplate.cfm?myurl = checklist.html&mytitle = ICF%20Checklist (accessed 26/06/06).
18. Scheuringer M, Grill E, Boldt C, Mittrach R, Mullner P, Stucki G. Systematic review of measures and their concepts used in published studies focusing on rehabilitation in the acute hospital and in early post acute rehabilitation facilities. Disabil Rehabil 2005; 27: 419–429.
19. Weigl M, Cieza A, Harder M, Geyh S. Linking osteoarthritis specific health status measures to the International Classification of Functioning, Disability and Health. Osteoarthritis Cartilage 2003; 11: 519–523.
20. Stucki G. International Classification of Functioning, Disability and Health (ICF). A promising framework and classification for rehabilitation medicine. Am J Phys Med Rehabil 2005; 84: 733–740.
21. MacAllister WS, Krupp LB. Multiple sclerosis related fatigue. Phys Med Rehabil Clin N Am 2005; 16: 483–502.
22. Fischer JS. Cognitive impairment in multiple sclerosis. In: Cook SD, ed. Handbook of multiple sclerosis. Third edition. New York: Marcel Dekker; 2001, p. 233–255.
23. Reitberg MB, Brooks D, Uitdehaag BMJ, Kwakkel G. Exercise therapy for multiple sclerosis. Cochrane Database Syst Rev 2005; 25: CD003980.
24. Brown TR, Kraft GH. Exercise and rehabilitation for individuals with multiple sclerosis. Phys Med Rehabil Clin N Am 2005; 16: 513–556.
25. Nicholas RS, Friede T, Hollis S, Young CA. Anticholinergics for urinary symptoms in multiple sclerosis. Cochrane Database Syst Rev 2003; 22: CD004193.
26. Borello-France D, Leng W, O’Leary M, Xavier M, Erickson J, Chancellor MB, et al. Bladder and sexual function among women with multiple sclerosis. Multiple Sclerosis 2004; 10: 455–461.
27. Ehde DM, Osborne TL, Jensen MP. Chronic pain in persons with multiple sclerosis. Phys Med Rehabil Clin N Am 2005; 16: 503–512.
28. Coggrave M, Wiesel PH, Norton C, Brazelli M. Management of faecal incontinence and constipation in adults with central neurological diseases. Cochrane Database Syst Rev 2006; 19: CD002115.
29. Stier-Jarmer M, Grill E, Ewert T, Bartholomeyczik S, Finger M, Mokrusch T, et al. ICF Core set for patients with neurological conditions in early post-acute rehabilitation facilities. Disabil Rehabil 2005; 27: 389–395.
30. Johnson KL, Fraser RT. Mitigating the impact of multiple sclerosis on employment. Phys Med Rehabil Clin N Am 2005; 16: 771–783.

