
Physical Medicine and Rehabilitation, University Hospital of Ghent, Ghent, Belgium
Background: Spinal arachnoid cysts are rare entities, which are composed of a duplication in the arachnoid membrane and resultant cerebrospinal fluid collection, which may present with a progressive myelopathy. The most common symptoms caused by spinal cord compression are paraesthesia, neuropathic pain, paresis and gait ataxia.
Clinical cases: We report here 2 cases from different perspectives of a spinal arachnoid cysts in spinal cord injury. The first case was the occurrence of a spinal cord injury due to compression of a spinal arachnoid cysts causing myelopathy. The second case is a patient who had a traumatic paraplegia for which stabilizing surgery was required and who subsequently developed a spinal arachnoid cysts with neuropathic pain. Both cases required surgery with immediate improvement. However, after a few months both patients needed a revision due to recurrence.
Conclusion: Spinal arachnoid cysts may present with a heterogeneous clinical picture. If cysts are not clinically apparent, a conservative treatment with careful observation can be a justifiable option. In patients with progressive symptoms, surgery is the gold standard of care. However, the literature describes the need for revision surgery in only 12.5% of cases. Regular follow-up is necessary because both of the patients reported here needed revision surgery.
Key words: arachnoid cyst; spinal cord injuries; spinal cord compression
Accepted Jun 21, 2021; Published Aug 26, 2021
JRM-CC 2021; 4: jrmcc00066
Correspondense address: Katrien Raes, From the Physical Medicine and Rehabilitation, University Hospital of Ghent, Ghent, Belgium. E-mail: katrien_raes@hotmail.com
Doi: 10.2340/20030711-1000066
Spinal cysts are cerebrospinal fluid pockets that may compress the spinal cord. They may present with different symptoms; for example, sensory disorders, pain, loss of strength and difficulty walking. We report here 2 patients with a spinal cord injury with spinal arachnoid cysts. In the case of patients with worsening symptoms, surgery is the gold standard of care. Regular follow-up is necessary; and both patients reported here needed revision surgery.
Spinal arachnoid cysts (SAC) are rare entities that are composed of a duplication of the arachnoid membrane and resultant collection of cerebrospinal fluid (CSF). SAC may present with a progressive myelopathy if they compress the spinal cord.
SAC are classified into primary (congenital or idiopathic) or secondary (acquired). Acquired SAC are the most frequent (1–3). The most common presenting symptoms are paraesthesia, neuropathic pain, paresis and gait ataxia due to spinal cord compression (2).
We report here 2 cases of SAC from different perspectives in patients with a spinal cord injury. The first case is the occurrence of a spinal cord injury (paraplegia) due to compression of a SAC causing a myelopathy. The second case is a patient with a traumatic paraplegia who subsequently developed a SAC with neuropathic pain.
Case 1
A 38-year-old woman presented with walking difficulties since 3 months. She had a history of systemic lupus. Eight years previously she had been involved in a traffic accident, with a compression fracture at vertebra L1, for which a posterior fixation Th12–L2 was performed, with the removal of the material 1 year later. Imaging of the lumbar spine was performed, showing the known fracture at L1. Clinical examination revealed a progressive loss of strength, hyperreflexia, absent vibration in the lower limbs and sensory disturbances in the right leg. The patient had a positieve sign of Babinski. The patient walked broadly and had mild urinary incontinence. Examination revealed the presence of paraplegia American Spinal Injury Association (ASIA) Impairment Scale (AIS) grade D incomplete with neurological level Th9 left and Th11 right (4). An urgent magnetic resonance imaging (MRI)(Fig. 1) of the full spine showed an extramedullary, intradural subarachnoid cyst from Th2 to Th7 with compression on the spinal cord. Urgent surgery was performed with marsupialization of the thoracic cyst and laminectomy at Th7. Postoperatively, there was positive progress with recuperation. One month later, the patient presented with deterioration and recurrence of symptoms. Urgent MRI revealed an increase in the size of the thoracic cyst. This required a second operation with the placement of a cysto-peritoneal shunt for drainage of the cyst. The patient required a valve replacement due to post-operative orthostatic headache. Subsequent positive evolution with additional initiation of multidisciplinary rehabilitation.
Eight months later, there was again a deterioration with evolution to AIS grade D incomplete, neurological level Th4. Imaging showed an increase in the known subarachnoid cyst up to Th2 level and appearance of a myelopathy level Th4 to Th7. Surgery was performed to remove the cyst at level Th2, together with a laminectomy at level Th1 to Th3. Since then, there is a favourable follow-up.
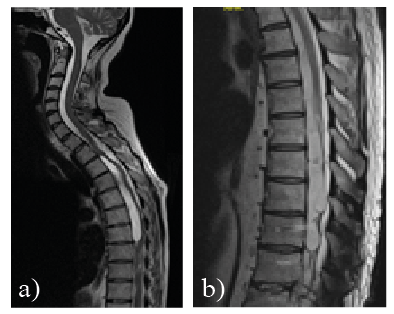
Fig. 1. Magnetic resonance imaging of a) patient 1 and b) patient 2
Case 2
A 45-year-old man had a high-intensity traffic accident causing fracture luxation at vertebra Th12. Stabilization, with a posterior lumbar interbody fusion Th10–L2, was required. Clinical examination revealed the presence of a complete paraplegia AIS A with neurological level Th11. One year later, the patient showed symptoms of an ascending sensibility loss, with allodynia up to neurological level Th4 and a mixed nociceptive and neuropathic thoracic back pain. MRI of the thoracic spine revealed the development of an intradural subarachnoid cyst after trauma and post-surgery, with an increase in the liquor space due to a disturbed CSF flow and pressure on the spinal cord Th4 to Th11. A laminectomy was performed at level Th9–Th11 together with a marsupialization of the cyst. There was a persistent pain post-operative for which, 2 months later, a re-intervention was performed with the placement of cysto-peritoneal drain with immediate, but short, improvement. In follow-up, there was only a slight improvement left with incomplete disappearance of the neuropathic pain.
Pathophysiology
Nabors et al. were the first to categorize spinal meningeal cysts on the basis of their anatomical location and tissue of origin following histological assessment (5, 6). The classification describes 3 categories: type 1 lesions being anterior or lateral meningoceles (extradural cysts), type 2 are extradural meningeal cysts containing nerve root fibres and type 3 representing intradural extra-medullar arachnoid cysts which are the subject of the current 2 cases.
The pathophysiological explanation of the formation of arachnoid cysts is unknown; thus various theories have been proposed. The leading theory is that SAC arise from a diverticula or dissection in the septum posticum; a thin fibrous membrane joining the arachnoid and pia along the posterior line of the spinal cord (6). However, reports of ventral cysts in the spinal cord suggest that there could be another origin. For example, incarceration of arachnoid granulations may produce CSF that become entrapped in arachnoid diverticula. These sequestered pockets of fluid lead to further disruption of normal CSF flow and are thus capable of expanding or producing associated arachnoid cysts along the path of least resistance. SAC give rise to compression of the spinal cord secondary to the complex CSF flow within the spinal canal (2, 7). Cystic enlargement, secondary to fluctuations in CSF pressure (Valsalva manoeuvre) has been explained by a 1-way ball-valve effect at the cyst neck (2, 8).
SAC are classified into primary (congenital or idiopathic) or secondary (acquired). Acquired SAC are more common and can be the result of a trauma, such as a traumatic spinal cord injury, postsurgical arachnoiditis, meningeal infection, haemorrhage, and other insults that cause inflammation and subarachnoid adhesions (1–3).
Clinical presentation
Most SAC are located in the thoracic region (80%) (3, 6, 9). They may be solitary or multiple. SAC may be asymptomatic (especially congenital cysts), but as they grow, they may present with a progressive myelopathy and give signs of an upper motor neurone disease. Paraesthesia (76%), neuropathic pain (76%), paresis (67%) and gait ataxia (53%) are the most common presenting complaints (2, 10). Hyperreflexia, hyper- or hypotonia, bowel- and bladder dysfunction may also occur. Anterior cysts are more likely to cause weakness and myelopathy, whereas thoracic cysts occur more commonly with neuropathic pain and numbness (2).
Diagnosis
The clinical presentation suggests an upper motor neurone syndrome for which additional imaging is required. The diagnosis of SAC is made by spinal cord imaging. The gold standard is MRI (3, 6). This shows a spinal extramedullary space-occupying mass that consists of a CSF collection. T1- and T2-weighted signals of arachnoid cyst are identical to those of CSF. There is no enhancement with gadolinium. If possible, a MRI with CISS-3D sequences should be performed, which allow high-resolution display of the subarachnoid space and the detection of septae, trabeculae, and intradural cystoid formations in a more precise dimension compared with T2w imaging (6). MRI flow study or CT/MRI myelography are other options (3). Myelography should be reserved for unclear cases to show or exclude communicating sites of the cyst with the subarachnoid space or eventually, in case of consideration of re-surgery due to insufficient shrinkage, when MRI imaging appears insufficient (3).
SAC may be progressive, increasing slowly over time and elongating over multiple levels. A syrinx may be associated with SAC (2, 6).
Therapy
The mean duration of symptoms before therapy is started, is 12–15 months (10).There are several treatment options for SAC. If the cysts are not clinically apparent, a conservative treatment with careful observation could be a justifiable option, especially for children or high-risk patients (3, 6, 9).
The role of acetazolamide (AZM), a carbonic anhydrase inhibitor known to reduce CSF production, is uncertain (7). Symptomatic SAC may be related to the elevated fluid pressure within the cyst on surrounding structures, thus reducing the amount of fluid in the cyst or surrounding CSF may hold promise. This might mimic surgical decompression, and therefore the AZM challenge could serve as a decision-making tool to recommend surgery in those patients whose symptoms improve during AZM therapy (7).
Surgery is the gold standard of treatment (6, 9, 10). Surgery should be considered in patients with progressive worsening of symptoms or recurrence (8). Surgical marsupialization with or without laminectomy is the most commonly used technique (2). Other possibilities are cyst fenestration, resection or the placement of a cysto-peritoneal drain (2, 6).
Following surgery, 60–70% of the patients experience improvement. Gait disturbance and motor weakness were most likely to improve (2, 6). Motor weakness has the highest response rate (71%) and pain the least (50%).
Revision surgery was indicated in 12.5% of cases. Long-term follow-up shows no difference in quality of life between the different surgical techniques (6).
Both of the current cases underwent marsupialization of the arachnoid cyst with laminectomy and felt immediate improvement. However, they both needed revision surgery with the placement of a cysto-peritoneal drain.
SAC are rare lesions that may present with a constellation of neurological symptoms: paraesthesia, neuropathic pain, paresis and gait disturbances, just like a (progressive) spinal cord injury due to compression of the spinal cord. SAC may also be acquired, as the result of a traumatic spinal cord injury. The pathogenesis remains a matter of debate. If cysts are not clinically apparent, conservative treatment with careful observation could be a justifiable option. However, in patients with progressive or recurrent symptoms, surgery is the gold standard of treatment.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize