
1Physiotherapy, HK Physio Limited, Sidmouth, UK
2Medical Acupuncture, Dr Max Forrester Acupuncture, Taunton, UK
Phantom limb pain is clinically defined as the perception of pain or discomfort in a limb that no longer exists. Most amputees will experience phantom limb pain, which is associated with a low health-related quality of life. Phantom limb pain represents an important challenge in finding an effective therapy. The scientific evidence for best practice is weak, and is characterized by various clinical reports describing the pragmatic use of drugs and interventional techniques. Recent approaches to restore the sensory motor input have shown promise. One such technique is electroacupuncture. We report here a case study of a male in his 30s who sustained severe injuries, including a high transfemoral amputation, as a result of being hit by a car. An electroacupuncture treatment protocol was used. Over the course of 3 months, electroacupuncture alleviated the patient’s phantom limb pain, minimized his use of drugs, and improved his sleep and quality of life. The effect of electroacupuncture treatment lasted for 3–4 months, and successful top-up treatment maintained his pain relief. The results are in line with a study comparing massage and electroacupuncture in patients with spinal cord injury with neurogenic pain; a limited number of patients treated with electroacupuncture were significantly alleviated of their pain for months. This case report suggests that electroacupuncture may be useful in patients with phantom limb pain.
Key words: electroacupuncture; phantom limb pain; treatment.
Accepted May 10, 2021; Published May 31, 2021.
JRM-CC 2021; 4: jrm00061
Correspondence address: Holly Margaret King, Physiotherapy, HK Physio Limited, Sidmouth, EX10 0BU, UK. E-mail: holly@hkphysioltd.co.uk
Doi: 10.2340/20030711-1000063
Since phantom limb pain was first described by the French military surgeon Ambroise Pare in the 16th century, the number of studies has increased every year. Although many hypotheses have been proposed regarding the mechanisms of pain and many treatments approaches tried, there is a lack of successful treatments to induce long-term pain relief, improve sleep and quality of life in patients with phantom limb pain. A novel treatment approach used in patients with spinal cord injury pain is electroacupuncture. This case report used a long-term electroacupuncture protocol in a patient with phantom limb pain.
For decades phantom limb pain (PLP) has confounded researchers and practitioners. PLP is a debilitating and draining condition that significantly hinders amputees’ sleep (1), quality of life, and rehabilitation outcomes. Amputees experiencing moderate to severe PLP frequently report that post-amputation pain has a greater impact on their lives than the amputation of the limb itself (2, 3). In the same way, patients with spinal cord injury (SCI) may experience neurogenic pain (4). PLP was first described by the French military surgeon Ambroise Pare in the 16th century (5) and is a painful sensation felt in part of the body that has been removed (6, 7). PLP is extremely prevalent in amputees; a study in 2005 recorded 60–80% of amputees suffering from PLP (8), and in a subsequent study in 2020 as 67–87% of amputees (9). Clinicians and patients who do not experience PLP may find it difficult to understand the description of pain in PLP, and therefore may be less empathetic towards patients who experience PLP (10). Large-scale surveys of amputees highlight the ineffectiveness of treatments for PLP (11), and the detrimental side-effects of pharmaceuticals (12, 13), which leave the majority of patients with PLP with insufficient pain relief (14). Recently approaches to restore the sensory motor input have shown promise (15). A study of pain in SCI has highlighted the positive effects of non-pharmacological treatments for neurogenic pain to not only alleviate pain but also improve mood and sleep (16).
The International Association for the Study of Pain (IASP) (17) defines post-amputation pain as “PLP: any noxious sensory phenomenon in the missing body part that develops after surgical amputation of a limb. Chronic stump pain: localised to the site of the amputation, often neuropathic and increased in patients with severe pre-amputation pain”. However, these definitions do not cover the complex nature and origin of the pain perceived by an amputee. Amputees will present with the same description and pattern of pain in the phantom limb; however, the underlying mechanisms of pain have been suggested to differ from neuropathic, neuromata and nociceptive (18).
Structural and biomechanical changes take place following the transection of nerve fibres, including upregulation of sodium channels, activation of mitogen-activated protein kinases, and altered gene expression, leading to hyperexcitability and spontaneous discharge (19). Local firing of the afferent nerve fibres in the dorsal root ganglia (20) can create nociceptive signalling and cross-excite neighbouring neurones (21).
It has been proposed that factors in both the peripheral and central nervous system play major roles in triggering the development and maintenance of pain associated with extremity amputations (22). Different pathogenic models have been used to explain PLP, including the neuroma model and other peripheral origin models, the neuromatrix model, the cortical remapping model, the stochastic entanglement model and, finally, models based on proprioceptive memories (23). We hypothesize that neuropathic PLP chronicity may be prevented by eliminating the peripheral nociceptive stimuli. This case report describes the successful alleviation of PLP, following a traumatic transfemoral amputation, with an electroacupuncture (EA) protocol.
The patient was a fit and active man in his 30s, when he was hit by a car, sustaining catastrophic injuries to his left side resulting in a high transfemoral amputation (Table I). He experienced poorly managed PLP, despite pharmacological treatment and conservative pain management strategies. He reported stabbing pain, fizzing and dull ache in his left phantom foot, and cramping and aching in his phantom limb and toes. He rated his PLP pain on average as 7/10 on a Visual Analogue Scale (VAS) and at its worst as 9/10. His sleep pattern had become very poor due to PLP, he struggled to get to sleep at night, often not settling until the early hours of the morning, and he slept for no more than 2 h at a time.
Table II. Treatment
On discharge from hospital he was prescribed 900 mg gabapentin 3 times a day, and zopiclone 3.75 mg at night, as required. He experienced minimal pain relief and considerable side effects from the pharmacological medication, including loss of concentration, alertness and increased fatigue. He had tried graded motor imagery, education and sleep strategies during admission to private rehabilitation (see Table II for details of treatment). His Brief Pain Inventory (BPI) score (which reviews all pain: musculoskeletal and neurogenic) reduced from 46 to 35 during admission, although he reported no discernible improvement in his PLP.
“PLP is constant every night, disturbing my sleep and is unbearable. The medication and treatment I have had do not make any difference”
Table II. Treatment
Treatment
Seven months after the accident, the author HK began working with the patient as his specialist amputee physiotherapist. The patient had extensive keloid and grossly adhered scarring in his residual limb, but no evidence of neural tethering, sensitized neuromata formation or nerve entrapment. His residual sciatic nerve was mobile, and he had a negative tap test.
The patient consented to EA treatment, despite initially being very sceptical. His starting pain was 7–9/10 on VAS and BPI 35.
Treatment started immediately. Points were chosen from a Western medical perspective and placed in areas with pain and in strong general acupuncture points: 8 needles in central lumbar paraspinals between levels L2 and L5, to a depth of 40 mm, with 2 channels (Fig. 1), and 2 needles in sensitized points in the residual limb, to a depth of 40 mm, with 1 channel (Fig. 2) using a Seirin L-Type acupuncture needle with guide tube 0.25 × 60 mm and machine AS SUPER 4 digital (Schwa-medico, Germany), Programme 20. The intensity was high (2.0–3.0 mAmp controlled by the patient) giving a non-painful paraesthesia. Each session lasted 40 min (as there is a positive correlation between high-dose acupuncture treatment and positive outcomes) (24) once a week for 6 weeks, and then reducing to fortnightly for 6 weeks. He reported no adverse effects from EA treatment.
Fig. 1. Eight needles in central lumbar paraspinals between L2 and L4, to a depth of 40 mm, with 2 channels.
Fig. 2. Two needles in sensitized points in the residual to a depth of 40 mm, with 1 channel.
Outcomes
After the first treatment the patient noticed a significant reduction in his phantom pain intensity and frequency (reported as 6/10 on the VAS) and slept a full 4 h straight that night for the first time since the accident. Following the first few treatments he reported:
“I have been getting some better sleep and I forgot to take my meds because I was feeling better”.
After 4 sessions the patient was able to reduce his prescription of gabapentin from 900 to 800 mg 3 times a day and stop his sedative use. He did not notice any increase in his pain or side-effects from treatment. He consistently got better sleep and was no longer disturbed by the PLP.
After 6 sessions he was able to reduce the gabapentin to 600 mg 3 times a day. After 8 sessions he was taking 400 mg gabapentin twice a day and his PLP had reduced to 5/10 on the VAS.
Over the course of 3 months he had 9 sessions of EA. The EA was able to provide up to 5 days of pain relief after a treatment and the PLP that he experienced was less intense (4–6/10 on the VAS) and he was able to reduce his prescription of gabapentin to 400 mg twice a day.
“I feel better in myself with less medication and felt less spaced-out”
Alongside the EA, successful scar tissue and myofascial release massage also improved his hip contracture and he achieved 5° of active hip extension, which reduced his musculoskeletal and residual limb pain from 9/10 to 4/10 on the VAS.
At 12 months, with periodic top ups of the EA protocol every 4–5 weeks, and weekly physiotherapy intervention (including lumbopelvic-hip control, walking gait education and musculoskeletal treatment for back pain, and residual limb scar tissue management), the patient reported that his PLP was significantly better. He has been able to stop all his medication (Fig. 3) and his PLP now occurs only 1 night a week and for no more than 1 h (Fig. 4) and, at worst, his PLP is 5–6/10 on the VAS (Fig. 5). His BPI score is now 18. He is able to sleep 7–8 h a night and is only woken once and not from PLP (Fig. 6).
“EA is great at managing my PLP. I have been able to stop all my medication and I feel more in control. I still get occasional nights of PLP, but they are so much less frequent and don’t last so long”.
Fig. 3. Gabapentin prescription dosage taken during electroacupuncture (EA) treatment.
Fig. 4. Frequency and duration of phantom limb pain (PLP) during electroacupuncture (EA) treatment.
Fig. 5. Visual analogue scale (VAS) pain scores during electroacupuncture (EA) treatment.
Fig. 6. Sleep pattern during electroacupuncture (EA) treatment.
This case study examined the use of an EA protocol for the treatment of PLP, without the presence of sensitized neuromata or nerve entrapment.
PLP is the most common and debilitating problem experienced by amputees. Pharmacological treatments are strongly associated with negative side-effects and are often ineffective (13). Other non-pharmacological conservative therapies (e.g. graded motor imagery, mirror therapy, hypnosis) have limited evidence to support the potential benefits, and for electromagnetically shielding liners, the evidence is conflicting (24). A reduction in peripheral input (even when contralateral) through local anaesthetic reduces PLP (25).
Acupuncture is not widely used as a treatment tool in PLP, with only 1% of amputees reporting having used it (26). EA has been found to be effective for treating a variety of chronic pain conditions, including SCI pain (4), but little quality evidence is available on the use of EA for PLP (27).
A systematic review identified 26 case studies that used acupuncture treatment for PLP, and, of those, only 3 used EA as part of the treatment (28). A further data review found a further 2 case studies (29). In all 5 studies EA was used as an adjunct to MA and the treatment protocols and needling points were inconsistent across participants (30, 31, 32, 33), providing no repeatable methodology. In a study to find consensus on the acupuncture protocol for PLP no consensus was met on whether to use EA, the only consensus was made on finding de-qi (34). It is unclear from these papers what the optimal acupuncture treatment is for PLP, but it is noted that EA produced the greatest reduction in intensity of phantom pain compared with MA (30).
EA is defined as the passage of a pulsed electric current through the body tissues via 1 (or more) pairs of acupuncture needles for therapeutic purposes (35) and has been widely used since the late 1970s. A recent study employing electrical stimulation of acupoints compared with MA and sham control produced superior results (36). EA effectively treats neuropathic pain (37), and more effectively at 2–10 Hz than at 100 Hz (36). As concluded in a SCI study using EA at high frequency (80 Hz) (4). There is a positive correlation with high-dose acupuncture treatment and positive outcomes (24); therefore the author used extended 40-min treatment sessions.
Theories associated with central cortical reorganization as a result of the loss of input to the cortical zone of the amputation, maybe exacerbated by persistent nociceptive input. The primary site of injury in peripheral nerves, dorsal root ganglia and spinal cord is more likely to be the primary cause of pain in the early period post-amputation. These could be the sites of action for EA in PLP (39, 40).
This case report is important, as it shows, for the first time, that an easily reproducible EA protocol was effective in reducing PLP in an amputee, as shown by a significant decrease in all pain scores. Healthcare professionals working with amputees should consider EA as a therapeutic option for PLP.
EA was used successfully in this case for the alleviation of PLP, enabling the amputee to wean off pharmaceuticals, improve their sleep and quality of life. This novel and easily reproducible EA protocol can be used with lower- and upper-limb amputees. EA is a safe (41, 42) treatment modality, which merits consideration for use in amputees with PLP.
The authors have no conflict of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize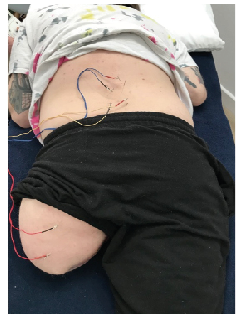 Click to show fullsize
Click to show fullsize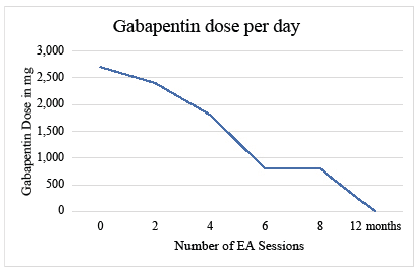 Click to show fullsize
Click to show fullsize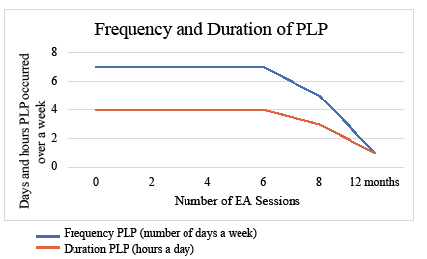 Click to show fullsize
Click to show fullsize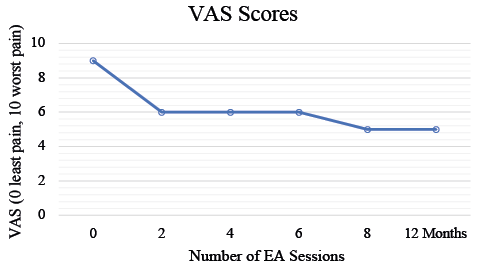 Click to show fullsize
Click to show fullsize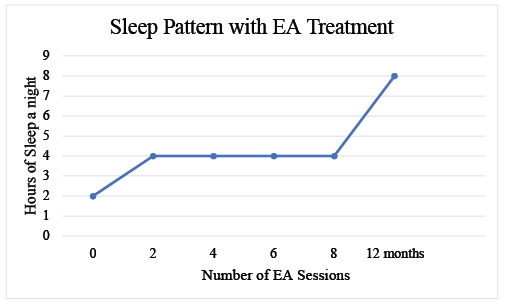 Click to show fullsize
Click to show fullsize