
1Radboud University Medical Centre, Donders Institute for Brain, Cognition and Behaviour, Department of Rehabilitation.
2Sint Maartenskliniek, Department of Rehabilitation, Nijmegen, The Netherlands
3Research Department, Sint Maartenskliniek, Nijmegen, The Netherlands
4Department of Orthopaedics, Sint Maartenskliniek, Nijmegen, The Netherlands
Objective: Toe walking due to progressive shortening of the calf muscles is common in people with hereditary spastic paraplegia. Achilles tendon lengthening is a treatment option, but clinicians are often hesitant to use this procedure, as it may result in weakening of the calf muscles and, subsequently, in reduced ankle power and knee instability during the stance phase of gait. We report here a case report supporting that these negative side-effects can be avoided in well-selected people with hereditary spastic paraplegia.
Method: Bilateral Achilles tendon lengthening, combined with bilateral tenotomy of the tibialis posterior and toe flexors, was performed in a 29-year-old woman with uncomplicated hereditary spastic paraplegia who experienced progressive gait instability due to shortening of the soleus and gastrocnemius muscles (resulting in irreducible pes equinus).
Results: Bilateral Achilles tendon lengthening resulted in improvement in both subjective and objective outcomes. Self-selected gait speed improved from 0.75 m/s before surgery to 1.07 m/s after surgery (p < 0.001). Knee instability during the stance phase did not occur post-surgery. The ankle moment trajectories normalized after surgery, while peak ankle powers increased.
Conclusion: Correction of bilateral irreducible pes equinus by Achilles tendon lengthening may improve gait capacity in well-selected subjects with hereditary spastic paraplegia.
Key words: hereditary spastic paraplegia; gait; surgery; Achilles tendon lengthening; pes equinus.
Accepted Mar 30, 2021; Published Maj 6, 2021
Jrm-CC 2021; 4: jrmcc00058
Correspondence address: Jorik Nonnekes, Radboud University Medical Centre, Donders Institute for Brain, Cognition and Behaviour, Department of Rehabilitation, PO Box 9101, 6500 HB Nijmegen, The Netherlands. E-mail: jorik.nonnekes@radboudumc
Doi: 10.2340/20030711-1000059
Toe walking due to shortening of the calf muscles is common in people with hereditary spastic paraplegia. This case report supports that lengthening of the calf muscles (Achilles tendon lengthening) may improve gait in well-selected people with hereditary spastic paraplegia.
Hereditary spastic paraplegia (HSP) is a diverse group of inherited disorders that, in its uncomplicated form, is typically characterized by progressive spasticity, muscle weakness and reduced proprioception of the legs (1). Gait and balance impairments are reported as most disabling by people with uncomplicated HSP, resulting in falls and fall-related injuries (2).
”Toe walking”, a gait pattern characterized by the absence of heel-to-floor contact, is very common in individuals with HSP and is related to spasticity and/or progressive shortening of the calf muscles, resulting in reducible (dynamic) or irreducible (rigid) pes equinus. Pes equinus may coincide with either excessive knee flexion or (excessive) knee extension during the midstance phase of gait, but, either way, toe walking impacts on gait capacity in a negative manner due to a reduced base of support and loss of gait efficiency.
In the case of irreducible pes equinus, in particular, an important treatment option is to surgically lengthen the Achilles tendon to compensate for the shortened calf muscles, with the aim of restoring a plantigrade position of the foot during standing and walking and improving gait efficiency (3). In clinical practice, however, many clinicians are hesitant to perform Achilles tendon lengthening, as this procedure may reduce the strength of the calf muscles. This fear of ”making things worse” is particularly strong in the case of bilateral pes equinus, such as commonly observed in people with HSP. Weakening the calf muscles may result in reduced ankle power and gait propulsion and, combined with increased ankle dorsiflexion range, lead to increased knee flexion during the stance phase of gait.
We report here a case of a 29-year-old woman with HSP who had good calf muscle strength, in whom bilateral Achilles tendon lengthening for bilateral irreducible pes equinus significantly improved gait capacity, as shown by detailed clinical gait analysis before and one year after surgery.
We report here a case of a 29-year old woman with an uncomplicated form of HSP (due to a heterogeneous ATL1 missense mutation, SPG3A) who provided written informed consent to use of her medical data for publication. Over several years, she gradually developed bilateral calf muscle shortening, despite repeated bilateral intramuscular injections of botulinum toxin into the gastrocnemius, soleus, and tibialis posterior (total dose per treatment: 1,500 U Dysport®), combined with self-administered daily stretching exercises. Shortening of the soleus and gastrocnemius muscles resulted in bilateral irreducible pes equinus (i.e. maximal passive ankle dorsiflexion up to 25° and 10° plantarflexion on the right and left side, respectively (with the knees either flexed or extended)). Calf muscle hypertonia was difficult to examine bilaterally due to the severe contractures, but was estimated to be relatively low. The tibialis posterior and toe flexor muscles were, however, clearly hypertonic bilaterally (modified Ashworth scale 2–3/5). On both sides, the ankle plantarflexors and knee extensors showed good voluntary strength (Medical Research Council Scale 5/5), while active recruitment of the ankle dorsiflexors was weak (Medical Research Council Scale 2/5). Motor selectivity of both legs was good.
Due to progressive calf muscle contractures, the patient reported increasing gait instability and decreasing gait efficiency and endurance. To correct the irreducible pes equinus and dynamic toe flexion, bilateral Achilles tendon lengthening was performed (a percutaneous lengthening, using 3 stab incisions technique and manually pushing the foot in dorsiflexion until sufficient lengthening was achieved), combined with bilateral tenotomy of the tibialis posterior and toe flexors (digits 2–5). Post-surgery, she received weight-bearing serial casting for the lower legs for a period of 6 weeks.
3D instrumented gait analysis was performed prior to surgery and repeated one year after surgery, consisting of video-recordings and 3D-kinematic (Vicon Motion Systems, Vicon Motion Systems, Oxford, UK) and kinetic (AMTI Custom 6 axis composite platform, USA) measurements of gait pattern. After collection of anthropometric data, 16 markers were attached to the skin of the lower extremities according to the modified Helen Hayes model (4). Lower extremity joint kinematics and kinetics were calculated using the Vicon Clinical Manager. Hip, knee and ankle range of motion were defined, as well as joint moments-of-force and joint power. Based on the heel and metatarsal-II markers, spatiotemporal gait parameters were calculated. Differences between pre- and post-surgical spatiotemporal parameters were tested using Mann–Whitney U tests.
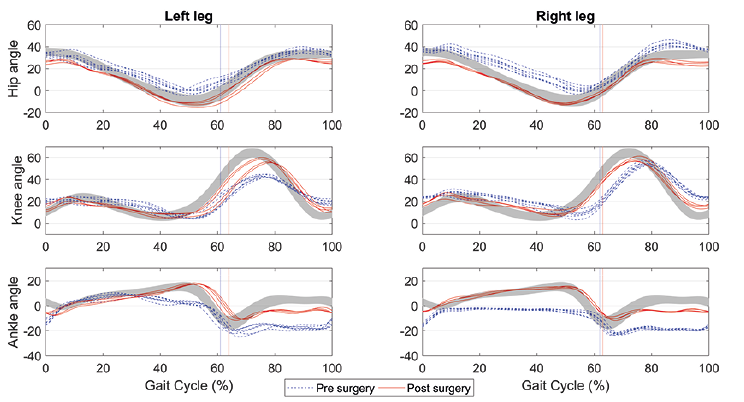
Before surgery, as shown in Video 1 and Fig. 1 (kinematic data), the patient’s gait pattern was characterized by a bilateral absence of heel contact during the stance phase of gait (with permanent ankle plantarflexion on the right side) and bilaterally increased knee and hip flexion (most pronounced on the right side). Video 1 also shows lumbar lordosis and an abundance of balance correcting trunk and arm movements. During the swing phase, permanent ankle plantarflexion and compensatory increased hip flexion (most pronounced on the right side) were observed.
Fig. 1. Hip, knee and ankle angle during various gait cycles.
One-year post surgery, the patient felt much more stable when standing and walking than before surgery. She spontaneously reported experiencing more energy and being able to walk much longer distances (she was able to complete a 4-km mountain trail and to resume her former occupation as a ”walking coach”). Passive ankle dorsiflexion had increased to 20° on both sides (with the knees flexed and extended), while calf muscle tone had become completely normal. Although initially weakened (Medical Research Council Scale 3/5), the strength of her ankle plantarflexors was bilaterally restored one year after surgery, while active recruitment of the ankle dorsiflexors had improved compared with pre-surgery (Medical Research Council Scale 3/5).
During the stance phase of gait, video recordings (Video 2) and kinematic data (Fig. 1) showed a plantigrade foot position, with an ankle plantarflexion movement at the end of the stance phase, a normalization of hip and knee angles, a reduction in lumbar lordosis and less balance-correcting trunk and arm movements. Knee stability was good on both sides. During the swing phase, reduced ankle plantarflexion angles, increase in knee flexion angles (most pronounced on the left side) and reduced (compensatory) hip flexion angles (most pronounced on the right side) were observed.
The patient’s self-selected gait speed improved from 0.75 m/s before surgery to 1.07 m/s after surgery (p < 0.001). In addition, the step length of both legs had increased and become more symmetrical (Table I). Fig. 2 and Fig. 3 show the (changes in) joint moments-of-force and joint power. The ankle moment trajectories had normalized after surgery, while peak ankle powers had, on average, increased from 1.5 W/kg (left side) and 1.0 W/kg (right side) to 3.0 W/kg and 2.5 W/kg, respectively, reflecting a clear improvement in push-off power bilaterally.
Table I. Median (and ranges) of spatiotemporal gait parameters
Fig. 2. Hip, knee and ankle moments-of-force during various gait cycles.
Fig. 3. Hip, knee and ankle power during various gait cycles.
This case study has several implications. First, it illustrates that correction of bilateral irreducible pes equinus by Achilles tendon lengthening may improve gait capacity in well-selected subjects with HSP. Improved gait capacity in this case was evidenced by a combination of subjective and objective outcomes, of which a 43% increase in self-selected gait speed and a clear improvement in walking distance were most impressive.
Clinicians are often hesitant to perform (bilateral) Achilles tendon lengthening in patients with spastic paraparesis due to the risk of knee instability and loss of push-off power. The current case shows that these negative side-effects can be avoided in well-selected subjects, even when combined with the tenotomy of assistive ankle plantarflexors (tibialis posterior, long toe flexors). It is likely that the initially preserved calf and quadriceps strength, combined with good motor selectivity on both sides, provided a sound basis for bilateral surgical correction of rigid pes equinus. Remarkably and unexpectedly, this case study illustrates that Achilles tendon lengthening may (nearly) normalize ankle-moment trajectories and enhance peak ankle power, thereby improving gait propulsion and increasing stride length, gait speed, and walking distance. These observations argue against the notion that calf muscle weakness is an inevitable consequence of Achilles tendon lengthening resulting in loss of push-off power after surgery. Interestingly, we have observed a similar result, of improved peak ankle power, after bilateral botulinum toxin treatment for hypertonic calf muscles in people with uncomplicated HSP (unpublished observation). Contracted and hypertonic calf muscles may prevent people with HSP fully utilizing their available calf muscle strength during push-off. Improved push-off most likely explains the increased knee flexion during (pre-)swing, facilitating foot clearance. Foot clearance also improved because of better recruitment of ankle dorsiflexors and smaller ankle plantarflexion angles, thereby reducing the need for a compensatory increase in hip flexion.
From a biomechanical point of view, this case report highlights the importance of adequate ankle strategies. To control the position and movement of the centre of body mass during standing and walking, humans have 3 basic strategies: (i) generating moments around the ankle joints (“ankle strategy”); (ii) rotating body segments around the centre of mass, for instance by flexing the trunk and swinging the arms (“hip strategy”); and (iii) adjusting foot placement (“stepping strategy”) (5). Bilateral rigid pes equinus makes it difficult, or even impossible, to maintain normal foot contact with the floor, resulting in a reduced base of support. A normal base of support is a prerequisite for effective ankle strategies.Thus, compensatory hip strategies (e.g. trunk and arm movements), or foot placement adjustments are needed (the stepping pattern may become wider and less regular). The knees and hips often become more flexed to avoid knee hyperextension and to keep the centre of body mass above the area of foot contact. This strategy also lowers the centre of body mass for more postural stability. Through adequate ankle-foot surgery, plantigrade foot position can be restored and, thus, a normal base of support and the ability to apply ankle strategies. This case illustrates that such distal surgical correction decreases the need for energy-consuming compensatory proximal trunk and arm movements, reduces lumbar lordosis, normalizes knee and hip kinematics, and reduces the need for foot placement adjustments (i.e. allows a less variable gait width). Future studies should further underpin these assumptions by applying measures of dynamic postural stability and energy consumption during gait. They should also try to identify positive and negative outcome predictors of (bilateral) Achilles tendon lengthening in people with HSP.
JN and AG are members of the European Reference Network for Rare Neurological Diseases- Project ID No 739510.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize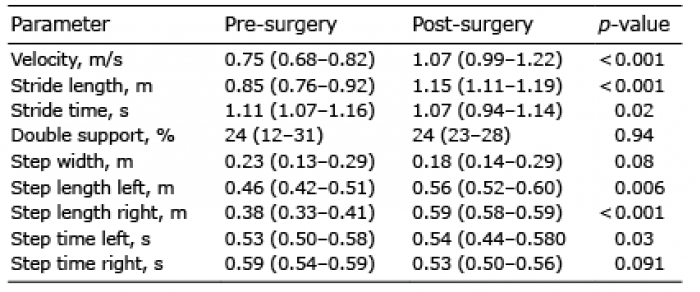 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize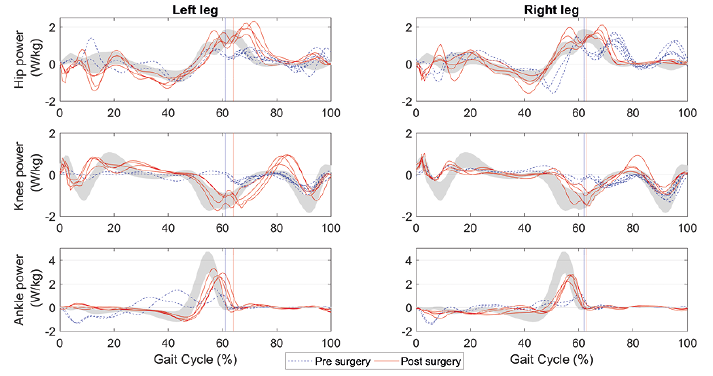 Click to show fullsize
Click to show fullsize