
1Department of Physical and Medical Rehabilitation, Centre hospitalier universitaire (CHU), Brest, France
2Department of Radiology, Hopital Inter Armée, Brest, France
3Laboratory of Medical Information Processing, LaTIM INSERM- Institut National de la santé et de la recherche médicale -UMR1101, Brest, France
4University of Western Brittany – UBO (université de Bretagne occidentale), Brest, France
5Department of Pediatric Physical and Medical Rehabilitation, Fondation ILDYS, Brest, France
6Department of Pediatric Surgery, CHU Brest, Brest, France
7Department of Pediatrics, CHU Brest, Brest, France
8Department of Radiology, CHU Brest, Brest, France
The consequences and optimal treatment of quadriceps fibrosis following intramuscular quinine injection during childhood remain unclear. We report here a case of a 17-year-old girl who experienced unilateral quadriceps fibrosis following intramuscular injection of quinine as a baby. This case report describes the evolution of the condition during the child’s growth, the long-term impact of early fibrosis on range of motion, muscle volumes, strength, gait, and activities of daily living. Rehabilitation involved orthoses and physiotherapy from the age of 6 years, when her knee flexion was reduced to 90°. A Judet quadricepsplasty was performed at 12 years because of continued loss of knee range with consequences for gait. At 16 years, knee range was satisfactory and gait variables were normalized. Functional evaluations and quality of life scales showed excellent recovery. Isometric strength of the involved quadriceps remained lower than the expected age-matched strength. Magnetic resonance imaging identified amyotrophy of the quadriceps, specifically the vastus intermedius. Despite being a focal impairment, quadriceps fibrosis had wider consequences within the involved limb, the uninvolved limb and functioning. This case report illustrates how children with quadriceps fibrosis can have a good prognosis, with excellent functional results at the end of the growth period, following early and appropriate management.
Key words: quadriceps fibrosis; paediatric intramuscular injection; gait analysis; strength rehabilitation; magnetic resonance imaging; activities of daily living.
Accepted Feb 26, 2021; Published. May 10, 2021
JRM-CC: 2021; 4: jrmcc00059
Correspondence address: Jessica Luthringer, Service MPR Hôpital Morvan, 5 avenue Maréchal Foch, 29200 Brest, France. E-mail: Jessica.luthringer@chu-brest.fr
Doi: 10.2340/20030711-1000054
Children with malaria may be treated by a quinine injection into their quadriceps (thigh muscle). Unfortunately, this can cause fibrosis (scarring) inside the muscle. Fibrosis can prevent muscle growth, cause weakness and limit knee movement. The progression of the condition during growth is poorly documented and the best treatment methods are not known. We describe the case of a girl with quadriceps fibrosis. We explain the problems she had from the age of 6 to 17 years, and the treatment that she received. At the age of 6, she began rehabilitation, involving splints and physiotherapy. At the age of 12, she had surgery to lengthen her quadriceps and help her to bend her knee. By the time she was 16, her leg was much stronger, she had sufficient knee movement, and she could walk normally. Early and continued rehabilitation combined with surgery lead to successful results.
Intramuscular quadricipital injection (IMQ) of vaccines or antibiotics is still common in children in African and Western countries because the technique is simple and requires little equipment or follow-up. It has, however, been associated with a high rate of orthopaedic complications, such as quadriceps fibrosis (QF) (1, 2). QF has been associated with intramuscular quinine injection (in children who received 2 injections) in 81% of cases (2), and is believed to be caused by the acid and hypertonic nature of the quinine preparations, which leads to vascular necrosis (3).
QF results in a painless limitation of knee flexion (1, 3) and decreased muscle volume (4). Despite the potentially severe functional consequences of this pathology, few studies have evaluated the long-term outcomes of QF, and there are few guidelines regarding rehabilitation or surgery. Some studies have reported improvements in range of motion with surgical procedures, but the level of evidence remains poor (2, 5, 6).
Data regarding the long-term evolution of children with QF are needed to better understand this pathology and its consequences. To develop optimal treatment strategies for these children (rehabilitation and surgical procedures), data are specifically needed about changes in strength and range of motion (ROM), and the impact on gait and activities of daily living (ADL). To this end, we report here the surgical and rehabilitative management of a girl with QF, from the ages of 6 to 16 years, who had received IMQ quinine at 3 months. We report on the evolution of the QF during her growth, and the long-term impact of early QF on her ROM, muscle volume, strength, gait, and ADL, and use these data to discuss appropriate rehabilitation follow-up for these patients.
Before surgery
The child was born in Bamako, Mali, in 2003. The pregnancy and birth history were unremarkable. At 3 months of age, she received IMQ quinine injections in her right thigh. She arrived in France at the age of 3.5 months, and at 6 years, she was diagnosed with asymmetrical knee flexion and right thigh amyotrophy: her maximum right knee flexion was 90° (Fig. 1). Strength of all lower limb muscular group appeared similar on both sides, with a rating of 5/5 on the Medical Research Council scale (MRC).
From the age of 6 years, she attended twice weekly outpatient physiotherapy sessions that focused on passive stretching, and at the age of 8 years, she was also enrolled in an intensive, passive stretching, inpatient rehabilitation programme during the school holidays. After the first of these inpatient sessions, she began to wear an orthosis at night and at rest, which passively held her right knee in a position of maximum flexion (110°). Knee ROM remained stable until she was 9 years old (90°) and MRC rating was 5/5. At this time, her first 3D gait analysis revealed a slight, but non-significant, decrease in peak right knee flexion during the swing phase. At this time, other kinematic, kinetic and spatiotemporal variables were within normal ranges (Fig. 2).
Fig. 1 Timeline: rehabilitation support and surgical management throughout the growth.
Fig. 2. Knee kinematics (gait analysis). Knee kinematics of the involved limb at 10, 12 and 14 years of age. Gait deterioration at 12 years indicated the need for surgery to improve knee flexion during swing phase (peeak reduced to 40˚). Gait normalized at 2 years post-surgery (peak 60˚)
Surgery
From the age of 10 years, the subject’s right knee ROM values began deteriorating, and by 12 years of age, knee flexion had reduced to 60°; she also reported difficulties climbing stairs, passing obstacles and participating in athletics training. Isometric strength testing (Table I) using a hand-held dynamometer (7) revealed decreased strength in her right thigh compared with the left (uninvolved). The involved/uninvolved strength ratios were 0.59 (extensors) and 0.45 (flexors). Ankle dorsiflexor and plantar flexor strengths were symmetrical in both limbs.
Table I. Mean strength (Newtons) (3 trials) Table showing the mean strength ratio of the involved lower limb compared to the uninvolved limb as a reference. Assessed using a hand-held dynamometer and following the protocol by EEK et al.
An MRI scan revealed a medial-distal impairment of the vastus intermedius (VI), associated with fatty infiltration and atrophy of the anterior compartment (Table II) (8, 9) in her right leg compared with the left leg. Muscle fat quantification using the DIXON sequence revealed an increased fat fraction in the distal third of the VI (20%) compared with the uninvolved limb (3%) (Fig. 3) (10). Posterior compartment volumes were symmetrical in both limbs (10). 3D gait analysis revealed a lack of right knee flexion during the swing phase (peak flexion: 40°), decreased ankle plantar flexion at the end of the stance phase and the beginning of swing phase, and a decrease in gait speed, compared with the previous assessment at 10 years (Fig. 2).
Table II. Muscular volumes: Table showing the muscular volumes of the legs. The volumes were calculated by fusing MRI images (2 upper and lower parts) then application of the same fusion parameters on the segmentations of each muscle group previously determined by manual cross-sectional area (using ITK SNAP software, ETHRIVE sequence) (9, 10). The anterior compartment included Vastus intermedius, Vastus medialis, Vastus lateralis, Rectus femoris and Sartorius. The posterior compartment included Gracilis, Semimembranosus, Semitendinosus, Adductors, Gluteus maximus, Gluteus medius, Gluteus minimus and Biceps femoris.
Fig. 3. Graph showing the fatty infiltration of leg muscle, expressed as a percentage of the total volume, for the vastus intermedius at 12 years of age, before the Judet quadricepsplasty. The data were assessed by a DIXON sequence using MRI images taken different levels.
This deterioration indicated surgical treatment, and so, at 12 years of age, she underwent a Judet quadricepsplasty, which included complete external detachment of the vastus lateralis (VL) and VI from the femoral diaphysis, and partial proximal detachment of the VL. Rectus femoris tenotomy was not performed because adequate flexion was obtained (120°). Postoperatively her leg was immobilized for 4 weeks in 100° knee flexion and 10° hip extension. When the cast was removed, her knee flexion reached 110°.
After surgery
Knee ROM remained stable from the age of 12 years to the final evaluation at 16 years.
The involved/uninvolved knee flexor strength ratio progressed to 0.73 at 14 years and remained the same at 16 years (Table I). Knee extensor strength ratio increased to 0.62 at 14 years and 0.79 at 16 years.
Involved/uninvolved VL volume ratio (Table II) reduced post-operatively and remained lower at 16 years compared with the pre-surgical assessment. Accordingly, anterior compartment volume ratio reduced post-operatively (0.49 at 14 years) (Fig. 4), but increased to preoperative levels by the age of 16 years (0.62) due to an increase in VI volume (Table II).
At 16 years, EOS imaging revealed no structural changes in the knee, and symmetrical femur length (Table III). 3D gait analysis showed gait variables were within normal ranges. Functional evaluations (Knee injury and osteoarthritis outcome (KOOS CHILD): 91.7; activity of daily living (ADL): 96, Sport and play: 85) and quality of life scales (Pediatric quality of life inventory (PedsQL): Physical score: 84.4, Psychosocial score 87.5/Functionnal evaluations using self-administred scales (Mesure des habitudes de vie scale (M-HAVIE)) 10/10 on all items) showed normal values.
Fig. 4. A 3-dimensional illustration of the thighs of the child aged 14, 2 years post Judet quadricepsplasty. Each thigt muscle volume was assessed with MRI using an E-THRIVE sequence by manual segmentation of cross sectional area of each slice 9, 10 and showed atrophy of the whole anterior compartment, and more specifically of the Vastus intermedius. a) 3 dimensional reconstructions of thigh muscles based on manual segmentation completed with voxel remesh technique. b) MRI Axial section of the distal third of both thighs. c) 3 dimensional reconstructions: axial section. Vastus intermedius is colored in red on each figure and surrounded with a dotted line.
Table III. Femur length between the ages of 12 and 16 measured using EOS imaging
Other information
From the ages of 10 to 16 years, the patient regularly reported back pain and was diagnosed with, and treated for, mild scoliosis. She also described pain in her right knee, although further investigations did not indicate swelling, ligament damage or any radiological abnormalities.
This case study presents how appropriate rehabilitation and surgical management improved knee function, as well as activities, participation and quality of life in a girl with QF.
Magnetic resonance imaging (MRI) revealed the localized involvement of the VI, with significant atrophy and fatty infiltration at the site of the original quinine injection. Other effects included atrophy of the whole quadriceps, which limited ROM, strength and ADL, and caused painful orthopaedic sequelae throughout growth. The specific involvement of a single muscle (VI), may explain the lack of an effect on bone growth, in contrast to other childhood pathologies, such as cerebral palsy, or brachial plexus birth palsy, which often involve several muscles and lead to shortening of the involved limb.
In light of these results, we suggest that evaluations of QF should focus not only on ROM, but also on strength, gait, growth and the consequences on ADL. Evaluations should also be quantitative; in particular, a dynamometer should be used to measure strength (7). When the child was 6 years old, the MRC indicated normal strength, while this was unlikely, given the atrophy that was already present and the loss of strength found later using a dynamometer (7).
This case report illustrates how children with QF can have a good prognosis, with excellent functional results at the end of the growth period, following early and appropriate management.
The child had a good functional recovery, satisfactory ROM in her involved leg, and normal gait. In our opinion, the key elements of her successful management were the rehabilitation throughout her growth, as well as the use of both orthoses and quadriceps release surgery when first indicated. It is important that the type of surgery is adapted to the severity and location of the fibrosis. In this case, the Judet quadricepsplasty led to a good outcome. This intervention is well suited to patients with localized fibrosis on MRI; however, it might be insufficient for extensive fibrosis. In that case, quadriceps lengthening may be required (either in association with, or instead of quadricepsplasty), although this carries the risk of a loss of active knee extension (5, 6). High-quality studies are necessary to confirm or refine these findings.
The child’s mean torque values were lower than the range expected for healthy, age-matched children in all lower limb muscle groups, both before and after surgery (7), despite the increased strength and harmonization between the involved and uninvolved limbs (Table IV). The difference was greatest after surgery at 14 years of age. We hypothesize that this was initially caused by the low level of physical activity before the surgery, and subsequently by the post-operative immobilization. Isometric strength testing showed that strength increased proportionately more on the involved than the uninvolved side, and that the asymmetry between involved/non-involved torque reduced between the involved and uninvolved sides by the age of 16 years (4 years post-surgery) (Table I). Similarly, MRI revealed that the quadriceps volume had increased, including the VI (Table II). These results show that muscle strengthening can have a positive impact on children with QF and that children can benefit from long-term rehabilitation throughout their growth and even several years post-surgery. Future research should investigate the use of an intensive, pre-surgery quadriceps strengthening programme.
Despite originating from a localized impairment, the consequences of vastus intermedius fibrosis were wide-ranging: the reduced strength and ROM limited gait and impaired activity. The outcomes of this case study, however, are encouraging. They show that surgery and intensive rehabilitation throughout the growth increased ROM, and improved gait and function, despite the occurrence of this pathology in early infancy. For children with QF, we conclude that long-term rehabilitation support is necessary and should focus not only on stretching, but also on specific muscle strengthening.
Table IV. Mean torque (Newtons) (3 trials). Table showing the mean torque of healthy children: weight-related (first range) and age and sex related (second range) Strength assessment using a hand-held dynamometer (EEK and al. protocol) and normalized to the lever arm length. Only the values for the knee flexors of the uninvolved limb are within normal ranges for weight related torque. Age and sex related torque is below normal ranges for all muscle groups.
The authors have no conflicts of interest to declare


 Click to show fullsize
Click to show fullsize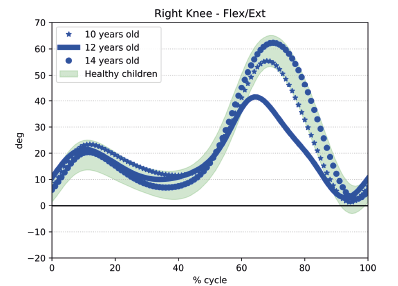 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize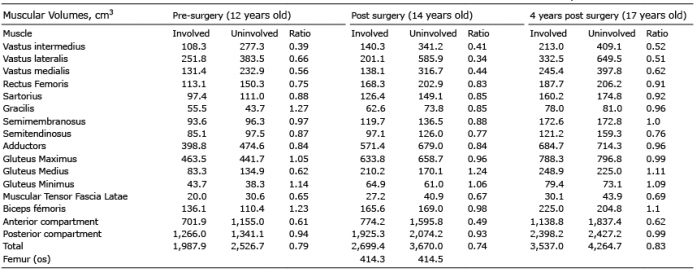 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize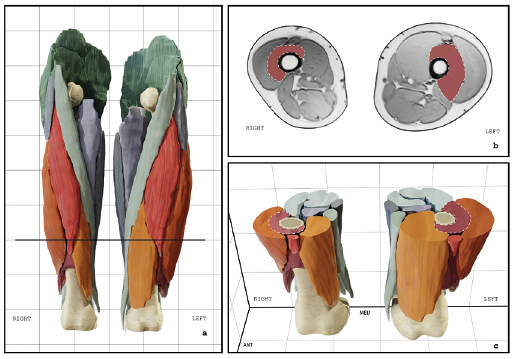 Click to show fullsize
Click to show fullsize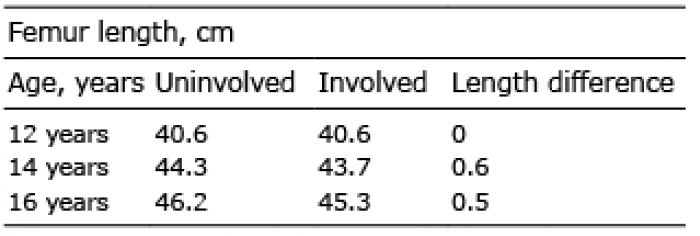 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize