
1Department of Rehabilitation, Fujita Health University Hospital, Aichi, Japan
2Faculty of Rehabilitation, Fujita Health University School of Health Sciences, Aichi, Japan
3Department of Rehabilitation Medicine I, Fujita Health University School of Medicine, Aichi, Japan
4Department of Nursing, Fujita Health University Hospital, Aichi, Japan
5Department of Neurosurgery, Fujita Health University School of Medicine, Toyoake, Aichi, Japan
*These authors contributed equally to this work.
Objective: To elucidate the characteristics of recovery progression during long-term rehabilitation after moderate-to-severe traumatic brain injury.
Methods: Longitudinal changes in consciousness, swallowing disorders, activities of daily living, and psychological and behavioural status were studied in 7 patients with moderate- to-severe traumatic brain injury, using scores of the National Agency for Automotive Safety & Victim’s Aid (NASVA score), Glasgow Coma Scale (GCS), Dysphagia Severity Scale (DSS), Eating Status Scale (ESS), Functional Independence Measure (FIM), Cognitive-related Behavioural Assessment (CBA), and Neuropsychiatric Inventory (NPI). Scores were collected every month until discharge (median 359 days after injury), or until the study end date for those patients who remained hospitalized (432 days).
Results: Patients were qualitatively classified into those who improved well in the early phase, in terms of consciousness, swallowing, and activities of daily living, and those with less or delayed improvement. Psychological and behavioural difficulties appeared to remain less improved than the other functions for longer periods in many patients. Statistical comparisons that included all 7 patients revealed a significant improvement in NASVA score, GCS, DSS, and ESS, but not in FIM, CBA, and NPI at discharge/at the last measurement compared with scores at admission.
Conclusion: Swallowing function is more responsive to long-term rehabilitation in patients with moderate-to-severe traumatic brain injury, while neuropsychiatric and behavioural difficulties tend to persist for longer periods.
Key words: traumatic brain injury; disorder of consciousness; rehabilitation; functional recovery; swallowing disorder; cognitive deficit, neuropsychiatric symptom.
Inpatient rehabilitation programmes have been shown to encourage functional recovery in patients with consciousness disturbance after traumatic brain injury (TBI). However, it remains unclear how physical and cognitive functions, including the swallowing function and neuropsychiatric symptoms, change during long-term inpatient rehabilitation. The present study retrospectively investigated longitudinal changes in these functions in 7 moderate-to-severe TBI patients. Patients were qualitatively classified into two groups comprising those who showed improvement in consciousness, swallowing, and activities of daily living in the early phase, and those who showed less or delayed improvements. Psychological and behavioural difficulties remained less improved than the other functions for longer periods in many patients. Statistical comparisons of all the patients revealed a significant improvement only in consciousness and swallowing function. This case series demonstrates that the swallowing function is more responsive to long-term rehabilitation, while neuropsychiatric and behavioural problems tend to persist for longer periods.
Accepted Dec 8, 2020; Published Jan 12, 2021
JRM-CC 2021; 4: jrmcc00045
Correspondence address: Yohei Otaka, Department of Rehabilitation Medicine I, Fujita Health University School of Medicine, 1-98 Dengakugakubo, Kutsukake-cho, Toyoake, Aichi 470-1192, Japan. E-mail: otaka119@mac.com
Doi: 10.2340/20030711-1000047
Traumatic brain injury (TBI) can cause disorders of consciousness (DOC), which may present as coma, vegetative state, or minimally conscious state (1, 2). From 2014 to 2018, there were 184,631 cases of TBI in Japan, approximately 90% of which (170,666 patients) required hospitalization after the injury (3).
Retrospective studies have shown that patients with TBI with severe DOC (i.e. persistent vegetative state) generally have a poor prognosis, such that only 8.2% of patients in a vegetative state recover from that conscious state after one year (4). During a 5-year follow-up period of 110 patients in a vegetative state, 73% died, while only approximately 10% recovered partially from DOC. Among the patients who recovered, only 3 could communicate, 2 of whom were not independent in their activities of daily living (5). The probability of recovering from a vegetative state or minimally conscious state, and regaining functional improvement, typically correlates inversely with the duration of DOC after injury (6).
However, early-onset rehabilitation programmes encourage functional recovery, even in patients with moderate-to-severe TBI (7, 8). A systematic protocol incorporating traditional therapies (occupational, physical, and speech), pharmaceuticals, median nerve stimulation, and nutraceuticals (termed an “advanced care protocol”) can improve disability and enhance recovery of physical, cognitive, and social activities, in patients with severe TBI (9). An interdisciplinary inpatient rehabilitation approach has been widely applied in the management of patients with severe TBI. This approach focuses on issues such as retraining in activities of daily living and cognitive and behavioural therapies (10).
Despite increasing evidence that an interdisciplinary inpatient rehabilitation approach can be beneficial for patients with moderate-to-severe TBI, provision of such treatment is limited. For instance, a cohort study investigating 163 patients showed that the median duration of sub-acute (inpatient) rehabilitation was 36 or 59 days, including the post-acute phase during the first year post-injury (11). Another study showed that the mean duration of inpatient rehabilitation was 41 days among 1,730 patients with TBI (12). A study examining the benefits of long-term inpatient rehabilitation, in which a mean of 409 days of post-injury rehabilitation was provided, showed the effects on reducing the level of dependency and enhancing the likelihood of a return to community living (13). However, it remains unclear how each of the physical and cognitive functions, including swallowing function and neuropsychiatric symptoms, changes during long-term inpatient rehabilitation.
The aim of the current retrospective study was to evaluate a case series regarding long-term longitudinal changes in consciousness, swallowing disorders, activities of daily living, behavioural problems related to cognitive impairments, and neuropsychiatric symptoms, in order to elucidate the characteristics of recovery progression during long-term inpatient rehabilitation. Clinical data were collected from 7 patients with moderate-to-severe TBI, who were assessed every month from the time of admission until discharge or until the end of the study for those patients who remained hospitalized. Time-course changes in each function were tracked, and scores at admission were compared with the latest scores, in order to evaluate potential differences in the recovery progress among these functions.
Setting
The study was conducted at the Care Center for Consciousness Recovery in Fujita Health University Hospital. This is a unique centre in Japan, which was established in 2018, in which intensive inpatient rehabilitation and medical treatments can be provided for up to 3 years for patients with TBI, including those with prolonged DOC. Part of the centre was supported by the National Agency for Automotive Safety and Victim’s Aid (NASVA).
Patients
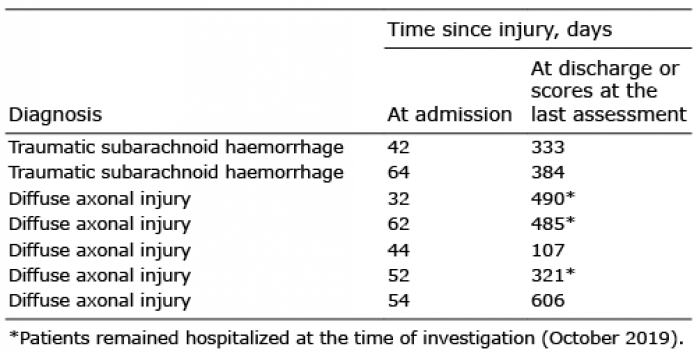
This retrospective study enrolled 7 patients with TBI who were admitted to the Care Center for Consciousness Recovery from April 2018 to April 2019 (Table I). Inclusion criteria were: patients with moderate-to-severe TBI after a car accident (scores 3–12 on the Glasgow Coma Scale (GCS) (14)); admitted to the intensive care unit (ICU) in the university hospital within 30 days after injury; and then admitted to the Care Center for Consciousness Recovery after completion of critical care; requiring assistance all the time in all activities of daily living. All patients were transported to the ICU after car accidents and then admitted to the consciousness recovery centre after completion of critical care. The study protocol was approved by the ethics committee at Fujita Health University (approval number HM19-255) and was conducted in accordance with the principles of the Declaration of Helsinki. Data collection was conducted after receiving informed consent from the legal guardian of each patient.
Table I. Patients’ characteristics
Inpatient rehabilitation and medical treatments
While staying at the centre, all patients were managed with a systematic treatment protocol. All patients were given intensive rehabilitation training, including 40 min of physical, occupational, and speech-language therapies, 5 days per week. Training consisted of standing and over-ground walking with a knee-ankle-foot orthosis with full assistance from a therapist. Neck and trunk orthoses and/or body-weight support were also used, depending on the conditions of the cases. Swallowing training consisted of indirect and direct exercises: the former included training for swallowing-related subfunctions without using foods or liquids (e.g. shaker exercise, tongue-base retraction exercise); while the latter involved direct swallowing training using actual foods and/or liquids. Every day, when not undergoing therapy, the patients were given the opportunity to sit in an upright position in bed or a wheelchair, supported by a nurse. In addition, visual (e.g. entertaining TV shows) and auditory stimuli (e.g. sounds of chewing before meals) were given to patients during the daytime in order to spontaneously stimulate physical and cognitive activities. A single nurse delivered care to a given patient throughout their period of hospitalization (i.e. primary nursing system).
All patients were prescribed medications to accelerate recovery from impaired consciousness (levodopa, amantadine hydrochloride) and/or to control muscle tone (clonazepam, baclofen). In addition, dorsal column stimulation and phenol nerve block injection to the adductor longus muscle were given to one patient (case 4) in an attempt to improve the DOC and reduce spasticity, respectively.
Study design and assessments
Level of consciousness was evaluated, as well as physical and cognitive functions, using the records collected every month from admission until discharge in 4 of the 7 patients (cases 1, 2, 5 and 7). For the other 3 patients who were still hospitalized (cases 3, 4 and 6), recorded data were collected until the time of the investigation (October 2019). Level of consciousness, swallowing disorders, activities of daily living, and cognitive functions were assessed using the scores of the NASVA score and the GCS, Dysphagia Severity Scale (DSS) and Eating Status Scale (ESS), Functional Independence Measure (FIM), Cognitive-related Behavioural Assessment (CBA), and Neuropsychiatric Inventory (NPI), respectively.
The NASVA score was developed to assess the level of consciousness of victims of TBI after a vehicle collision (15) (Table SI1). It consists of a 6-item subscale regarding motor response, ingestion, faecal/urinary function, visual recognition, vocalization/utterance, and response to call/oral command; each is scored on 5 levels (0 = very mild; 5 = mild; 7 = moderate; 9 = severe; 10=very severe). An increase in the total score, which ranges from 0 to 60, is indicative of deterioration in the state of consciousness. In our hospital, patients with more than 30 points are eligible for hospitalization in the consciousness recovery centre and are discharged when the score drops to below 20 points.
The GCS is a structured method for assessing level of consciousness, which is widely used worldwide. The essence of the GCS is to independently assess the responses of 3 functional domains; eye opening (E), motor response (M) and verbal activity (V). In a person who is fully conscious, alert, and oriented, the GCS will be E4 M6 V5 (score 15 points), and a reduction in the score is indicative of deterioration in the state of consciousness. The minimum score of E1 M1 V1 (3 points) is given to a subject who has no eye opening (E1), no motor response (M1), and no verbal response (V1) to any kind of stimuli (16). GCS has been proven to have substantial inter-rater reliability, especially in methodologically good and fair studies (17).
The DSS and ESS are the assessment batteries for swallowing disorders. DSS is a 7-point comprehensive ordinal scale for assessing the severity of dysphagia (18) (Table SII1). The score is generally given based on instrumental evaluations, such as videoendoscopic or videofluoroscopic evaluation of swallowing. ESS is a 5-point ordinal scale for assessing the severity of eating dysfunction (1 = tube feeding only; 2 = oral < tube; 3 = oral > tube; 4 = modified oral feeding; and 5 = oral feeding, (19)).
The FIM is an established tool for assessing a subject’s ability to carry out activities of daily living. It consists of 18 items related to self-care (6 items), sphincter control (2 items), mobility (3 items), locomotion (2 items), communication (2 items), and social cognition (3 items). Each item is scored on a 7-point scale (1 = complete dependence; 7 = independence). Summing the scores across all items generates a total score that ranges from 18 to 126, with lower scores reflecting greater disability (20, 21). The total FIM score has been shown to have good test-retest reliability, inter-rater reliability, and equivalence reliability (22).
The CBA was developed to assess cognitive functions in Japan, using easy and understandable concepts and terms (23). Scoring is based on observation of the patient’s behaviour. It uses a 6-item subscale regarding consciousness, emotion, attention, memory, judgement, and insight into disease with a 5-point scale (1 = very severe; 2 = severe; 3 = moderate; 4 = mild; 5 = good). The total score ranges from 5 to 30, with lower scores reflecting more severe cognitive dysfunction.
The NPI was originally designed to survey neuropsychiatric disorders in patients with dementia. This evaluates 12 neuropsychiatric disturbances: delusions, hallucinations, agitation, dysphoria, anxiety, apathy, irritability, euphoria, disinhibition, aberrant motor behaviour, night-time behaviour disturbances, and appetite and eating abnormalities (24). Each abnormality is rated based on frequency (0 = not at all; 1 = occasionally or less than a week; 4 = very frequently, more than once a day or continuously) and severity (1 = mild; 3 = severe) of symptoms. The total NPI score is the sum of all the individual domain scores, ranging from 0 to 120. Since similar symptoms can be observed after a head injury, the NPI has also been used recently for patients with TBI (25). The NPI has good test-retest and inter-rater reliability (26), and the validity of each item has proven reasonably high (27).
Data analysis
First individual time-course changes were depicted for each assessment score to capture the differences in the recovery progresses among physical and cognitive functions. Scores at admission were then statistically compared with those at discharge or the latest scores, using the Wilcoxon rank-sum test to determine which score showed a significant improvement during hospitalization. Statistical analysis was performed using SPSS version 24 (IBM Corp., Armonk, NY, USA) software. A p-value < 0.05 was considered statistically significant.
Fig. 1 shows the time-course changes for each test battery. Longitudinal assessment reveals that the patients can be qualitatively classified into 2 groups: patients (cases 1, 2, 5 and 7) who showed faster and greater improvements in the level of consciousness (NASVA score and GCS), swallowing disorders (DSS and ESS), and level of independence in activities of daily living (FIM); and the rest of the patients (cases 3, 4 and 6) who showed relatively less or delayed improvements in these batteries. In the latter group of patients, changes in consciousness-related responses were limited to activities such as the appearance of aimless spontaneous movements (cases 3 and 4) and/or spontaneous eye opening (cases 3 and 6) (Table II and Table III). Regarding cognitive functions, most of the patients showed little improvement; 1 (case 7) even had a worse CBA score during the period of hospitalization. Similarly, neuropsychiatric problems (NPI), which can be detected only in patients with a relatively better level of consciousness (cases 1, 2, 5 and 7), did not substantially improve.
Fig. 1. Changes in assessment scores over time. Coloured lines represent changes over time for each individual (horizontal axis: every month after time of admission). Vertical axis: scores for each assessment battery. Left-most circles and the right-most diamonds indicate scores at admission and discharge (or the latest score for patients who were still hospitalized), respectively. NASVA score: National Agency for Automotive Safety and Victim’s Aid score; GCS: Glasgow Coma Scale; DSS: Dysphagia Severity Scale; ESS: Eating Status Scale; FIM: Functional Independence Measure; CBA: Cognitive-related Behavioural Assessment; NPI: Neuropsychiatric Inventory.
Table II. Sub-scores and total scores of the National Agency for Automotive Safety and Victim’s Aid (NASVA score)
Table III. Sub-scores and total scores of the Glasgow Coma Scale (GCS)
In line with the above findings, statistical comparisons of the whole group of patients revealed significant improvements in NASVA score, GCS, DSS, and ESS at the time of discharge or at the time the latest measurements were performed, compared with those at admission (Wilcoxon rank-sum test, Table II, Table III and Table IV). In addition, no significant changes were found in FIM, CBA and NPI during long-term hospitalization.
Table IV. Scores for swallowing disorders, activities of daily living, cognition, and neuropsychiatric problems
This case series investigated the longitudinal changes in physical and cognitive functioning in 7 patients with DOC after moderate-to-severe TBI, in order to elucidate the characteristics of recovery progress during long-term inpatient rehabilitation. Longitudinal observation revealed that the duration of improvement might vary depending on functions as well as on the individuals. Functions such as swallowing showed a greater improvement, while cognitive and neuropsychiatric functioning showed fewer improvements and impairments remained for longer periods.
It has been known that impairment in functional oral intake is quite common in patients with severe TBI. A previous study demonstrated that 61% of 53 patients with severe TBI, with GCS scores between 3 and 8, exhibited abnormal swallowing, such as loss of bolus control, reduced lingual control, or decreased retraction of the base of the tongue (28). Another retrospective cohort study showed that 93% of 173 patients with severe TBI with a median GCS score of 11 had problems with oral intake at admission (29). Consistent with these reports, all the patients enrolled in this study had swallowing dysfunction at admission. The current results further revealed that substantial improvements in swallowing disorder could occur during hospitalization in a majority of patients, including those who show only a marginal change in the level of consciousness (as in cases 3, 4 and 6). These results indicate that swallowing function tends to improve, or the patients become more tolerant of feeding/feeding methods, regardless of the degree of improvement in their level of consciousness. These findings indicate that appropriate care and rehabilitation approaches should be adjusted and provided accordingly and continuously match the changes at a functional level during hospitalization.
Significant improvements in consciousness-related scores occurred during long-term hospitalization. Importantly, all the patients who showed relatively greater and faster improvements in both NASVA score and GCS also exhibited substantial improvements in FIM score (cases 1, 2, 5 and 7). This result is in accordance with that of a previous study, which demonstrated that recovery in the level of consciousness is associated with improvement in the level of independence in activities of daily living (30). However, in this study, improvements in FIM score at the group level were not significant. This is because 3 patients showed only a marginal change in consciousness-related scores, but no significant change in FIM scores (cases 3, 4 and 6). A detailed examination of the breakdown of scores revealed that changes in consciousness-related scores, reflected by features such as an appearance of aimless spontaneous movements (cases 3 and 4) and spontaneous eye-opening (cases 3 and 6), were important changes in the level of consciousness, but too subtle to influence the level of independence in activities of daily living. The existence of a subgroup of patients that showed little improvement in FIM score over a longer period (at least for 10 years after injury) has been reported in a previous cohort study (31).
Regarding cognitive functions, no significant improvements were found in CBA or NPI. Even patients with mild TBI had cognitive deficits, such as impairment of incidental memory as well as immediate memory, and a delayed recall in the acute phase (within 24 h post-injury) (32), which could last one year after the trauma in 10–11% of patients (33). Another study reported that, in patients with severe TBI, a wide range of neuropsychiatric symptoms, such as apathy, irritability, and disinhibition lasted for at least one year (mean 10.6 months) after injury in 42%, 37% and 28% of the 120 patients, respectively (34). Along with previous prognoses reports, the current results indicate that cognitive and neuropsychiatric problems tend to remain for a longer period in patients with moderate-to-severe TBI, and thus a follow-up programme specialized to manage these problems is required.
The patients in the current study had a relatively wide age range, from teenagers to elderly individuals in their 70s. Previous research has shown that, in patients with severe TBI, age is a factor that influences the prognosis of the level of consciousness post-injury (e.g. at the time of 8 years post-injury, (35)). Sveen et al. demonstrated that patients with severe TBI who achieved independence from personal assistance in daily life by 1-year post-injury were younger than those needing daily assistance (11). Therefore, although the present study with a heterogeneous sample may be reasonable for individual investigation, caution should be applied when interpreting the grouped data.
In summary, all 7 patients with moderate-to-severe TBI in this retrospective study showed improvements in swallowing-related assessment scores along with recovery from DOC, despite individual differences in the speed and amount of improvement, but most of them tended to have ongoing impairment in neuropsychiatric and behavioural functioning for longer periods. Although the study number is small, the results indicate that swallowing function might be more responsive to long-term rehabilitation. Further investigations with a larger patient population are needed to draw more definitive conclusions; however, these findings support that inpatient rehabilitation, care programmes, and follow-up programmes should be specifically restructured to take into account the potential cognitive and neuropsychiatric difficulties of patients with TBI.
The authors thank the medical staff of the Care Center for Consciousness Recovery in the Fujita Health University Hospital for their help in data collection.
Funding. This study was partially supported by the National Agency for Automotive Safety and Victims’ Aid (NASVA).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize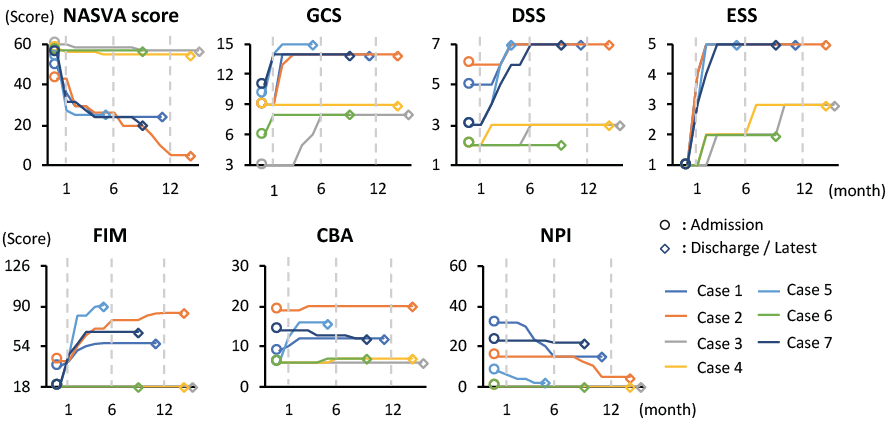 Click to show fullsize
Click to show fullsize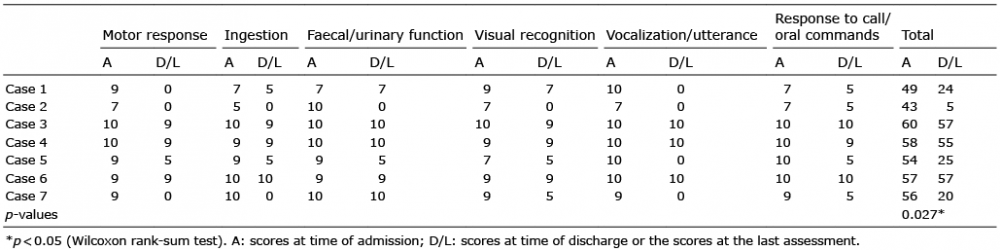 Click to show fullsize
Click to show fullsize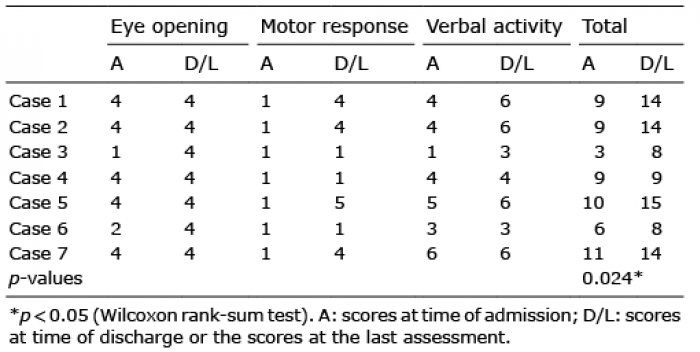 Click to show fullsize
Click to show fullsize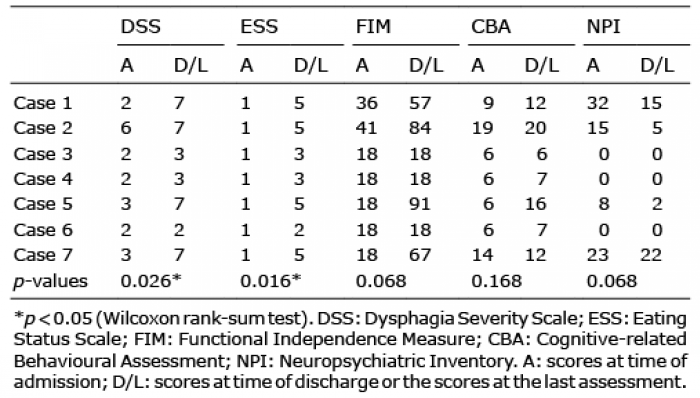 Click to show fullsize
Click to show fullsize