
1Rehabilitation Medicine Department, Tan Tock Seng Hospital, Singapore
2Physiotherapy Department, Tan Tock Seng Hospital, Singapore
Platypnea-orthodeoxia syndrome, characterized by dyspnoea and arterial desaturation while upright, is a rare complication of acute respiratory distress syndrome. We report here 2 patients with COVID-19 pneumonia, who were diagnosed with platypnea-orthodeoxia syndrome during commencement of rehabilitation, 18 and 9 days respectively after admission to the intensive care unit. Both patients presented with normocapnic hypoxaemia. One patient required mechanical ventilation with supplemental oxygen during intensive care, while the other required high-flow nasal oxygen therapy. The manifestations of platypnea-orthodeoxia syndrome were most prominent during physiotherapy, when verticalization was attempted, and hindered further mobilization out of bed, including ambulation. This report describes the clinical manifestations of platypnea-orthodeoxia syndrome and the rehabilitative strategies carried out for these 2 patients. The platypnea-orthodeoxia syndrome in these patients resolved after 65 and 22 days respectively from the day of detection. This report highlights this potentially under-recognized phenomenon, which may be unmasked during rehabilitation of patients with COVID-19 pneumonia. Good functional outcomes were achieved with a combination of verticalization training with supplemental oxygen support, respiratory techniques training and progressive endurance and resistance training, whilst awaiting resolution of the platypnea-orthodeoxia syndrome.
Key words: COVID-19; rehabilitation; case report; platypnea-orthodeoxia syndrome; pneumonia; acute respiratory distress syndrome.
Accepted Oct 28, 2020; Published Nov 20, 2020
Jrm-CC 2020; 3: jrmcc00042
Correspondence address: Shuen-Loong Tham, Rehabilitation Medicine Department, Tan Tock Seng Hospital, 17 Ang Mo Kio Avenue 9, Thye Hua Kwan Hospital, Singapore. E-mail: thamshuenloong@gmail.com
Doi: 10.2340/20030711-1000044
Platypnea-orthodeoxia syndrome can be a rare complication in severe pneumonia. Patients with platypnea-orthodeoxia syndrome experience decreasing oxygen levels when assuming upright positions. This can interfere with walking and other activities that require an upright posture. We report here 2 patients with platypnea-orthodeoxia syndrome in severe COVID-19 pneumonia and describe their journey to recovery whilst undergoing rehabilitation and physical therapy. The various strategies that were helpful included the use of additional oxygen, special breathing tech-niques, as well as reducing the pace of the exercises delivered. By the end of their rehabilitation programmes, the 2 patients were able to walk without the need for additional oxygen. The platypnea-orthodeoxia syndrome resolved after 22 and 65 days from the day of detection.
Coronavirus disease 2019 (COVID-19) has a hetero-geneous presentation, and although many patients have mild disease, a minority of patients can develop severe pulmonary manifestations (1). Dyspnoea and hypoxaemia are common symptoms of severe COVID-19 (1). More than 30% of such patients have viral pneumonias that progress to acute respiratory distress syndrome (ARDS) (1). Chest computed tomography of these patients shows classical findings of ARDS, including multifocal bilateral involvement, with a mixed pattern of ground-glass opacities and consolidation (2). ARDS survivors often experience impaired pulmonary function and exercise tolerance, which are comparable to findings from the previous pandemic of severe acute respiratory syndrome (SARS) (3). Similarly, patients who have recovered from severe COVID-19 ARDS are expected to be at high risk of pulmonary morbidity, which may manifest during post-acute rehabilitation.
Respiratory dysfunction and gas exchange limitation are therefore expected to be pronounced in a subgroup of severe and critical COVID-19 survivors, which may present commonly as persistent dyspnoea or hypoxia at rest or on exertion (4). Platypnea-orthodeoxia syndrome (POS), a rare clinical syndrome characterized by dys-pnoea and arterial desaturation > 5% (or a PaO2 drop of more than 4 mmHg) while in the upright position (5), may be an under-recognized post-acute sequelae in severe COVID-19 ARDS survivors. Despite the publication of standardized guidelines on the rehabilitation of COVID-19 patients, there is no clinical data about the rehabilitative strategies and clinical course of severe COVID-19 patients with POS.
We report here 2 patients with POS related to severe COVID-19 pneumonia, and detail the modifications to the usual physiotherapy approaches that enabled these patients to achieve good functional outcomes on discharge.
Case 1
A 69-year-old male, with a past medical history of gastritis, developed breathlessness and cough following return to Singapore from the UK. He had fever and worsening dyspnoea the following day, which prompted a visit to the emergency department.
His chest radiograph demonstrated consolidation in the right middle and lower zones, suggestive of a lung infection. Arterial blood gas analysis revealed severe hypoxaemia, which necessitated intubation and admission to the intensive care unit (ICU). He was diagnosed with COVID-19 through a SARS-CoV-2 polymerase chain reaction (PCR) test from an endotracheal tube aspirate.
A computed tomography angiography of the pul-monary arteries showed diffuse patchy air space opacities and ground-glass attenuation of both lungs, with no evidence of pulmonary embolism or intrapulmonary vascular malformation. Transthoracic echocardiogram demonstrated a normal left ventricular ejection fraction with mild pulmonary hypertension. No intracardiac shunt was evident. His liver function test was normal.
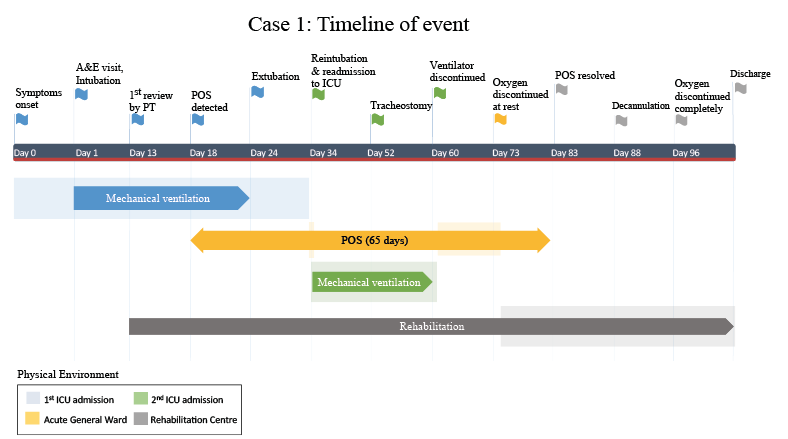
The patient was mechanically ventilated (with oxygen support) for approximately 7 weeks (Fig. 1). Tracheostomy was performed due to persistent respiratory failure and multiple episodes of ventilator-associated pneumonia. At 60 days from the time of symptoms onset, he was successfully weaned off mechanical ventilation and put on a tracheostomy mask with a fraction of inspired oxygen (FiO2) of 28%.
Fig. 1. Timeline of events in Case 1. A&E: accident and emergency department; ICU: intensive care unit; POS: platypnea-orthodeoxia syndrome; PT: physiotherapist.
Physiotherapy commenced on day 12 of admission, whilst the patient was still supported on mechanical ventilation. He was noted to have POS, 18 days after onset of first symptoms, when verticalization was first attempted. A supine oxygen saturation (SpO2) of 96% dropped to 84% when he was seated on the edge of the bed. This was accompanied by dyspnoea and tachypnoea. He was given an FiO2 of 100,% which abated his symptoms and increased his SpO2 to 100%. During this time, the positive end expiratory pressure (PEEP) was unchanged and maintained at 10 cmH20. He was able to commence therapy in a seated position. Gradually, it was observed that the patient only required an up-titration of FiO2 from 30% (at baseline) to 40% for maintenance of SpO2 above 90% during periods of verticalization. The degree of oxygen supplementation steadily reduced with resolving pneumonia. Through a series of active range-of-motion exercises and muscle strengthening exercises with light-resistance weights, and with increased supplemental oxygen use during therapy, he progressed to standing and eventually walking.
The patient also manifested exertion-induced desatura-tion and dyspnoea, and postural hypotension during this period. The former was effectively managed with respiratory techniques (e.g. deep breathing, controlled breathing) and activity pacing. Early in rehabilitation, he had persistent tachycardia, but this resolved with time.
The patient experienced POS for 65 days and had complete resolution thereafter. He did not require any supplemental oxygen use upon discharge. On discharge he was able to ambulate and perform self-care with supervision.
Case 2
A 63-year-old male with a past medical history of liver cirrhosis, hepatocellular carcinoma (in remission), chronic back pain, hypertension, diabetes mellitus, chronic obstructive pulmonary disease (COPD), and chronic psychiatric illnesses presented to the emergency department with a 4-day history of cough and fever. He was admitted following a diagnosis of COVID-19, confirmed by a positive SARS-CoV PCR test from a nasopharyngeal swab.
His condition remained stable until day 13 of ad-mission, when he became increasingly breathless and required supplemental oxygen. Arterial blood gas analysis revealed severe hypoxaemia, and he was admitted to the ICU for high-flow oxygen support and closer monitoring.
A computed tomography angiography of pulmonary arteries revealed bilateral patchy airspace consolidation with ground glass changes, suggestive of infection. There was no evidence of pulmonary embolism or intrapulmonary vascular malformation. He had a normal transthoracic echocardiogram, which did not reveal any intracardiac shunt. His liver function test was abnormal, but this did not differ much from his pre-infection findings.
Hypoxaemia resolved with a lateral/prone positioning regime and high-flow oxygen support. He was transferred to the general ward after staying for 8 days in the ICU.
Physiotherapy was initiated on the first day out of the ICU (day 26 from symptom onset). A supine SpO2 of 96% was noted whilst the patient was receiving 4 l/min of oxygen provided via nasal cannula. When he was stood and walked, SpO2 decreased to 88%, whilst on 4 l/min of oxygen delivered via nasal cannula. He was immediately rested, reclined and instructed to carry out deep controlled breathing. This restored his SpO2. A subsequent physiotherapy session was conducted 2 days later. Once again, his SpO2 decreased from 96–99% to 92–93% as he sat up from a lying position (whilst on 3 l/min of oxygen via nasal cannula). This was associated with tachypnoea and dyspnoea. There was a concomitant increase in heart rate (from 95 to 114 beats/min on verticalization), with no significant change in blood pressure. An increase in intranasal oxygen to 4 l/min improved his SpO2 to 95–97%, with relief of dyspnoea. This strategy was sufficient to allow for standing and ambulation training. The degree of oxygen supplementation was tuned downwards after the therapy sessions. During exertional activities, his SpO2 occasionally dropped to 88%, but this resolved with activity pacing and deep breathing. Caution was taken with oxygen supplementation for this patient in view of his background of COPD.
The patient experienced 22 days of POS, followed by complete resolution. He did not require supplemental oxygen on discharge, and was independent in ambulation and performing self-care tasks.
Verticalization is an integral part of rehabilitation. Vertical tolerance, either sitting or standing, is a pre-requisite to mobilization, activities of daily living (ADL) training or performance. Vertical intolerance will limit rehabilitation and hamper the functional recovery of the patient. Post-ural hypotension, a cause of vertical intolerance, is common, and has been described in patients with prolonged bedrest. POS, another cause of vertical intolerance due to dyspnoea and arterial desaturation while in the upright position, however, is a rare clinical entity. It is commonly seen with intracardiac shunting (e.g. patent foramen ovale or atrial septal defect) (5). Other described mechanisms include intrapulmonary shunts, hepatopulmonary syndrome, and pulmonary ventilatory-perfusion mismatch (6). POS in COVID-19 ARDS has been reported recently (7). However, we wish to highlight the impact of POS on verticalization, which prevents effective delivery of rehabilitation in patients with COVID-19.
Tan et al. hypothesized that the mechanisms under-lying COVID-19 ARDS-associated POS are related to a gravitational exacerbation of intrapulmonary shunting due to COVID-19-associated vasculopathy (e.g. microangiopathy, microthrombi) and alveolar hypoventilation (4). Factors that decrease cardiac output could contribute to further reduction in the areas of non-dependent zone of blood flow of the lungs, thereby worsening POS (4).
A reduced cardiac output typically follows prolonged bedrest. Protracted immobility and recumbency cause a redistribution of fluids in the supine body, triggering diuresis and reduction in blood volume. Cardiac deconditioning subsequently results. The lower leg skeletal muscle pump function is often compromised (owing to sarcopaenia from bedrest), resulting in reduced venous return during verticalization (8). Therefore, to mitigate the effects of reduced cardiac output on POS, it is imperative that exercise interventions and/or mobility training are implemented early. In the presence of concurrent post-ural hypotension, compression stockings and abdominal binders can be prescribed, along with optimization of hydration or fluid status. In addition, pharmacological adjuncts, such as fludrocortisone or midodrine, may be warranted.
Physical therapy
Early mobilization has been made a priority in our ICU. It has been shown to improve functional outcomes in patients, particularly in achieving mobility targets (9). During the initial discovery of POS, upright positioning of the patients was attempted with supplemental oxygenation, which was titrated to keep SpO2 above 90%. This progressed from head-up in bed to sitting out of bed and then to standing. Mobilization out of bed, including ambulation and ADL training, were prescribed once maintenance of SpO2 of more than 90% was possible for a period of at least 10 min.
While our patients were responsive to supplemental oxygen therapy, POS with poor response to increased FiO2 may also be possible (10). In such cases, in-bed exercises can be prescribed to minimize disuse-related muscle deconditioning whilst active treatment of the underlying cause is underway. These can include active range of motion exercises and resistive muscle training (core muscles, appendicular muscles, respiratory muscles, etc.). For patients with COVID-19, infection control policies may limit the use of cycle ergometry or functional electrical stimulation during periods of infectivity, which was the case in our institution. Use of such equipment can be considered once the patient is out of isolation.
In order to alleviate the symptoms of dyspnoea during rehabilitation, respiratory techniques, such as pursed-lip breathing, deep breathing and assumption of a forward leaning posture, were taught and adopted. Breathing retraining was also performed. As anxiety may also contribute to the sensation of dyspnoea, reassurance was provided and underlying causes of anxiety were address-ed, as appropriate.
Mild-to-moderate intensity resistance and endurance exercises were prescribed and carried out in short frequent sessions. High-intensity exercises of prolonged duration were avoided, as concerns arose over exacerbation of ventilation-perfusion mismatch in the lungs (11). Interval exercise training (e.g. scheduling multiple breaks in each session) was prescribed initially and slowly progressed to continuous exercise training as the patients’ vertical tolerance improved. In order to maximize therapy time and minimize the exposure of healthcare workers, self-directed, nursing-supervised exercises were also prescribed and encouraged between therapist-supervised sessions. During rehabilitation sessions, synchronous monitoring of SpO2 and heart rate were instituted. Blood pressure checks and assessment of dyspnoea and effort (using a self-reported scale) were performed at regular intervals during therapy. Paradoxically, POS in our patients may have been unmasked as a result of rigorous monitoring of vital signs during physiotherapy. POS may have existed prior to our detection, but remained undiagnosed due to the preceding period of recumbency.
Undoubtedly, the prolonged duration of POS negatively impacted the pace of rehabilitation in these patients. This was particularly disabling when POS persisted even after the patients were de-isolated and transferred to a dedicated tertiary rehabilitation centre for focused physical therapy and ADL training.
Following their time in inpatient rehabilitation, both patients’ POS resolved, and they were weaned of their need for supplemental oxygen during activities. The 6-Minute Walk Test for cases 1 and 2 were 210 m and 300 m, respectively, at discharge. The discharge Functional Independence Measure (FIM) scores were 116 and 120 (out of a possible 126), respectively.
There are a number of limitations to this study. Firstly, even though there was clinical evidence to demonstrate the presence of POS, the search for an underlying cause was daunting. There was a lack of definitive investigation to exclude the presence of intracardiac shunting due to logistical challenges. However, echocardiograms were performed for both patients, which did not reveal any significant anatomical abnormalities. Given the background of liver pathology, hepatopulmonary syndrome could be the aetiological basis for POS in CASE 2. However, as with intracardiac shunting, we believe that the likelihood is low, due to the absence of any reported signs and/or symptoms of POS prior to COVID-19 infection, and resolution of POS in tandem with improvement in COVID-19 pneumonia.
Secondly, the interventions used were explorative, borrowing from our experience in pulmonary rehabilitation and intensive care rehabilitation. The interventions described here were the successes that we had with our patients. Whilst the interventions helped with the patients’ coping with POS, they are by no means specific in mitigating the effects of POS. The mechanisms underlying and influencing POS are complex and poorly understood. As such, efficacious interventions may work directly and/or indirectly via a number of pathways.
POS is a disabling, but reversible, rare manifestation in severe COVID-19 pneumonia. It can co-exist with other more common presentations, such as dyspnoea or desaturation at rest or on exertion. Management is largely aimed at ameliorating its associated symptoms through the provision of supplemental oxygen and respiratory techniques whilst awaiting improvements in lung mechanics from resolution of ARDS/pneumonia. This facilitates ambulation training and other physical therapy, which mitigates the effects of prolonged recumbency owing to POS-associated vertical intolerance. In-bed therapy may be prescribed during the interim in order to maintain muscle activity and joint range-of-motion, whilst the body habituates to a vertical position.
This study was approved by the Institutional Review Board. Informed consent was obtained from subjects involved in the study.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize