THE EFFICACY OF IN-REACH REHABILITATION IN MORBIDLY OBESE POST SEPTIC PATIENTS: TWO RETROSPECTIVE CASE REPORTS

1Aged Care and Rehabilitation, Concord Repatriation General Hospital, Sydney, NSW, Australia
2Aged Care and Rehabilitation, South Western Sydney Local Health District, Sydney, NSW, Australia
3University of NSW, Sydney, Australia
4Hammondcare Health, Sydney, Australia
5Department of Rehabilitation Medicine, Royal Prince Alfred Hospital and St Vincent’s Hospital, Sydney, NSW, Australia
Objective: To report the functional outcomes of two patients with morbid obesity (> 250 kg) who received in-reach rehabilitation after hospitalization for sepsis in Sydney, Australia.
Case reports: A retrospective review of hospital charts was performed with the informed consent of both patients. Body mass index, demographics, length of stay, functional status at admission and discharge, medical comorbidities, social history, hospital course, equipment needs, therapy methods used, and discharge disposition were compared.
Results: Both patients had a positive outcome. Func-tion improved in case 1, from requiring hoist transfers, to mobilizing 80 m with 2 assistants. The patient was transferred to a subacute rehabilitation facility, but did not make any gain in Functional Independence Measure. Function improved in case 2, from requiring 2 assistants to walk with a frame, to walking independently with a 4-wheeled walker. The patient was discharged home from the acute hospital, with a minimal Functional Independence Measure gain of 8. Both patients lost approximately 45 kg during acute hospitalization.
Conclusion: These case reports demonstrate that in-reach rehabilitation can play an important role in the functional recovery of morbidly obese patients hospitalized with severe sepsis. This report also highlights the need for preventive interventions to reduce avoidable acute hospital presentations and to prevent functional decline.
Key words: obesity; bariatrics; rehabilitation; sepsis.
Accepted Oct 21, 2020: Published Nov 27, 2020
JRM-CC 2020; 3: jrmcc00043
Correspondence address: Baheerathan Narayanan, Aged Care and Rehabilitation, Concord Repatriation General Hospital, Sydney, NSW, Australia. E-mail: dr.baheerathan@gmail.com
Doi: 10.2340/20030711-1000042
These 2 case reports demonstrate the role of a rehabilitation intervention in improving functional outcome in severely obese patients who have lost function after being admitted to hospital for a severe infection. Both patients weighed over 250 kg, and received rehabilitation after a severe infection. These cases demonstrate how in-reach rehabilitation, provided by a rehabilitation team, resulted in improved function, enabling one patient to be discharged directly home, and the other to be transferred to a dedicated rehabilitation facility. These cases illustrate the complexities and benefits of providing rehabilitation in the acute hospital setting for this patient group.
In-reach rehabilitation (IR) refers to intensive and multidisciplinary therapy provided to patients with functional limitations who require ongoing management under an acute medical team (1). The goal is to improve physical and functional status and facilitate discharge home with reduced caregiver burden. Patients typically receive 1–2 h of multidisciplinary therapy each day, in addition to standard ward therapy. IR is an intervention that is suitable for patients who have ongoing medical issues that prevent discharge home and transfer to a subacute rehabilitation facility.
The combination of morbid obesity and sepsis creates complex medical management issues for caregivers during hospitalization and after discharge (2). There are many barriers to provision of effective IR for bariatric patients, including a lack of bariatric-specific equipment in acute wards, lack of standards of care specific to obese patients, biased attitudes among some healthcare staff, and lack of training programmes specializing in bariatric rehabilitation (3). Previous studies examining rehabilitation after hip and knee arthroplasty have shown that morbidly obese patients admitted to inpatient rehabilitation have a longer length of stay and higher costs to achieve Functional Independence Measure (FIM) gains compared with the non-morbidly-obese population (4, 5). Furthermore, compared with non-obese patients, morbidly obese patients are fearful of movement due to pain, which can be one of the factors that limits the functional gains made with rehabilitation after hip arthroplasty (6). Research suggests that multidisciplinary pain rehabilitation leads to improvement in physical and psychological functioning among obese patients (7). However, there is limited research on the impact of IR in morbidly obese patients post-sepsis.
We report here on 2 patients with morbid obesity who received IR after initial hospitalization for sepsis in Sydney, Australia. These cases demonstrate the efficacy of IR in severely decompensated morbidly obese patients, in achieving both functional gains, and significant weight loss. This report highlights some challenges in providing therapy in this patient group.
Case 1
Case 1 is a 63-year-old morbidly obese man weighing 280 kg who presented with septic shock secondary to worsening bilateral lower limb cellulitis. His medical history included obstructive sleep apnoea and chronic recurrent lower limb cellulitis. His clinical course in the intensive care unit (ICU) was further complicated by development of a sacral pressure ulcer and atrial fibrillation. After 9 days in intensive care, he was transferred to the medical ward, where his renal function normalized and he did not require further dialysis.
Case 1 is a retired truck driver who lived with his wife in a single-storey house with 4 access steps. Prior to hospital admission, he ambulated with a walking stick indoors and outdoors and was independent with all activities of daily living (ADL).
After 41 days in the acute ward, the IR team was consulted. At the time of initial review, the patient was severely deconditioned and required 8 staff for bed mobility, 4 staff for hoist transfers, 4 staff for assistance with sit-to-stand, and full assistance with personal care.
The initial goals of IR were to reduce the care burden to 3 staff for transfers and to begin sit-to-stand training with a forearm support frame (FASF), motivate the patient to lose weight, and coordinate sacral pressure care management. The medium-term plan was to enable smooth transition to a subacute rehabilitation facility once feasible.
A strict schedule for physical therapy sessions was enforced. Case 1 was encouraged to comply with dietitian recommendations, including meals with no added salt, low calorie intake, and high-protein diet. The dietary goal was to facilitate wound healing and promote weight loss.
After the second week of IR on the acute ward, the patient’s functional status had improved to requiring 3 staff to assist with bed mobility and transfers (no longer hoist dependent), one staff to assist with sit-to-stand, and he was able to mobilize 20 m with 5 seated rests using a FASF. However, he still required full assistance with ADLs.
By the end of 4 weeks, he required 2 staff to assist with bed mobility, 1 staff for sit-to-stand with a 2-wheel frame, and walked 80 m with 4 seated rests with 2 staff members. The patient was then transferred to a subacute inpatient rehabilitation unit for ongoing therapy. At the time of discharge from hospital, his body weight was 236 kg, a loss of 44 kg from admission. There was no FIM gain at the time of transfer to subacute rehabilitation facility despite demonstrated functional improvement.
Case 2
Case 2 is a 57-year-old morbidly obese woman weighing 270 kg who presented with sepsis, on a background of worsening lower limb cellulitis. Her medical history included chronic lower limb lymphoedema, type 2 diabetes, depression, epilepsy, obstructive sleep apnoea, recurrent deep vein thrombosis and pulmonary embolism.
At presentation, the patient required ICU admission for 6 days and was managed with intravenous antibiotics for group B Streptoccocal bacteraemia. She was stepped down to the medical ward after 6 days in ICU. The IR team was consulted on day 32 of the admission in the acute ward, and at the time of consultation, her lower limb cellulitis was resolving. She required 5 staff for bed mobility and 2 staff to sit to stand with a FASF. She could mobilize 18 m with a FASF with 2 staff members assisting. She needed full assistance with all her ADL.
Case 2 was commenced on a low-calorie, high-protein diet. During therapy sessions, she was highly motivated, gained self-confidence and participated well. By day 10 of IR, she had met all of her rehabilitation goals, including mobilizing independently with a 4-wheel walker. She was discharged home, with her daughter assisting with ADL, and was referred for home-based physiotherapy. Her weight at discharge was 225 kg; a loss of 45 kg over the course of the admission. Her motor FIM gain was only 8 at the time of discharge home.
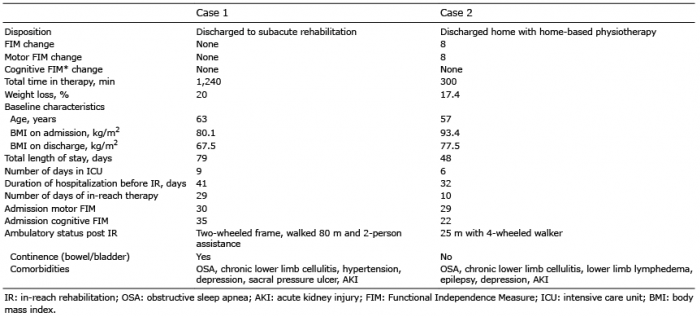
These 2 cases have some similar characteristics. There was no change in FIM in case 1 and only a small increase in case 2 as mentioned in Table I. Both were in the very high BMI category (>40 kg/m2), and of similar age. Prior to admission, despite significant obesity, both were functional indoor ambulators with the assistance of a walking aid. Both patients reported that dyspnoea and body habitus were limiting factors in performing ADL and had lifelong weight problems, with associated low self-esteem and low mood. There was no change in FIM in case 1 and only a small increase in case 2.
Table I. Summary of 2 cases with morbid obesity who received in-reach rehabilitation after hospitalization for sepsis
The literature suggests that, in comparison with non-obese patients, morbidly obese patients admitted to the ICU have higher morbidity and mortality (8). Rapid physical deconditioning and loss of function is common (9). In addition, poor peripheral muscle strength has been associated with decreased walking distance and inferior rehabilitation outcomes in patients with sepsis (10). There is strong evidence that morbid obesity is associated with poor overall quality of life and functional disability, while body fat percentage contributes to pain, fear of movement, anxiety and depression (11). In the 2 cases reported here, the interventions for achieving weight loss included strict caloric intake, increased physical activity and increased positive reinforcement to maintain a healthy diet. In the current study, both individuals lost approximately 20% of their initial body weight.
Depression is the most common psychological problem in morbidly obese patients, and is associated with negative body image and various forms of discrimination and prejudice (12, 13). Depression is a well-documented risk for non-compliance with treatment and disability (14). Both cases described here had depression. The psychological factors that were significant in both cases included decreased treatment motivation, marginal social role, maladaptive behaviour style, and poor coping mechanisms.
In both cases, deconditioning occurred in the context of a prolonged acute hospital admission. This may have been prevented or minimized with earlier involvement of the IR team, or earlier identification and treatment of cellulitis in the community, e.g. with home-based intravenous antibiotics. Low mood and poor self-monitoring and self-care may have contributed to the late medical presentation of both cases. In particular, the obesity itself probably prevented both individuals from self-identifying the early signs of lower limb cellulitis and seeking early medical attention.
Despite the absence of FIM change in case 1, there was a significant change in function. At the time of IR involvement, the patient was bed-bound, while at the completion of IR, he was able to mobilize 80 m with a 4-wheeled walker and the assistance of 2 staff. This improvement helped facilitate transfer to a subacute rehabilitation ward, but was not reflected in the FIM, which indicates the limitation of this tool in this cohort. Earlier commencement of IR and a shorter ICU admission for case 2 may have also played a role in achieving superior outcomes compared with case 1 (15).
A number of challenges in the provision of IR were noted in these cases, including the need for extra staff from other wards, organizing porters, utilizing nursing staff to assist in therapy sessions, and time taken to obtain bariatric-specific equipment. Also, as noted in other studies, body habitus was observed to reduce gait speed (16), and particularly high abdominal adiposity complicated the use of exercise equipment and gait aids (17). Furthermore, nursing staff encountered difficulties providing personal care for these cases including hygiene, prevention of decubitus and toileting (18). There was limited specific knowledge among staff of the management of morbidly obese patients, which further contributed to greater time and complexity in providing care.
In conclusion, IR (or other forms of rehabilitation) is essential in the functional recovery of morbidly obese patients following hospitalization with severe sepsis. With the increase in the prevalence of obesity globally, there is a need for structured rehabilitation interventions in the acute hospital setting to prevent and reverse functional deterioration, and in the community to prevent functional decline prior to health problems that may require hospital admission.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize