
Department of Rehabilitation, Tianjin Hospital, Tianjin, China
We report a case of a Chinese man who developed retroperitoneal haemorrhage almost 1 year after surgery for pelvic fracture (1). To the best of our knowledge, this type of delayed haemorrhaging is rarely observed in clinical practice. We also review the literature to identify the common causes of retroperitoneal haemorrhage in patients undergoing surgery for pelvic fracture and to examine the aetiology of this case.
Key words: retroperitoneal haemorrhage; rehabilitation; pelvic surgery
Accepted Aug 11, 2020; Published Sep 25, 2020
JRM-CC 2020; 3: jrmcc00039
Correspondence address: Xinlong Ma, Department of Rehabilitation, Tianjin Hospital, Tianjin, China. E-mail: maxinlong8686@sina.com
Doi: 10.2340/20030711-1000040
Retroperitoneal haemorrhage (RPH) is a common complication of pelvic fracture, which is associated with the risk of mortality. However, delayed RPH occurring several months after pelvic fracture surgery is rare.
We report here a case of RPH in a Chinese patient, which occurred nearly 1 year after surgery for pelvic fracture. In addition, we review the literature on the aetiology of RPH and analyse the causes in this case.
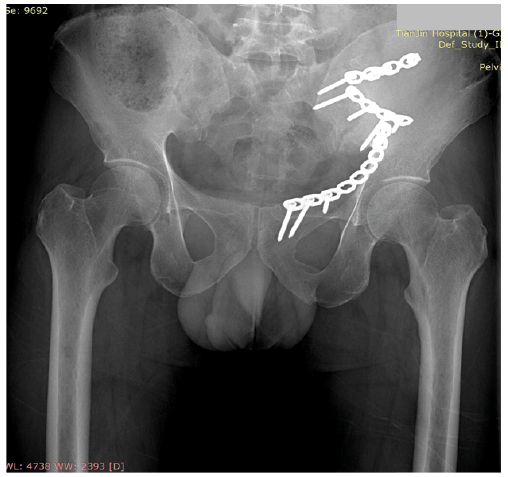
A 36-year-old man was first admitted to our hospital for abdominal pain caused by a forklift truck crush injury in February 2019. He had pelvic fracture of the lumbar transverse process (Fig. 1). The patient had a history of appendectomy, and no history of haematological or congenital anomalies. On 6 March 2019, he underwent open internal fixation of the pelvic fracture under general anaesthesia, followed by transfer to the rehabilitation department for functional training of the lower limbs. During rehabilitation, the patient reported intermittent abdominal pain (in the umbilical region), with no loss of appetite, or nausea and vomiting. There were no changes in his bowel movements (once every 1–2 days).
Physical examination revealed that the patient’s abdomen was flat and soft, with tenderness (positive abdominal tenderness; visual analogue scale score 2–3) in the periumbilical region and no rebound pain. No vascular anomalies were found on abdominal ultrasound or computed tomography (CT). On 16 January 2020, the patient underwent physiotherapy, during which he was treated with an electrical myofascial impactor (gun) (China) for 2 min to induce deep muscle stimulation, in order to release the stress in the left groin region (Fig. 2). After 30 min of treatment, the patient experienced pain in the left lower abdomen, which gradually worsened. Emergency abdominal ultrasound revealed a left lower abdominal haematoma 8.3 × 3.5 × 2.2 cm in size (Fig. 3). A CT image taken the next day showed the haematoma had increased in size to 10.5 × 4.4 × 2.7 cm (Fig. 4). Both Grey-Turner’s sign and Cullen’s sign were absent. The patient was transferred to the vascular interventional department, where angiography revealed haemorrhaging from the left internal iliac artery angiography.
Fig. 1. After pelvic fracture surgery (left sacroiliac joint separation and pubic fracture ) on the AP pelvic radiograph. The open reduction and internal fixation technique used in the operation. The internal fixation is a reconstructed titanium alloy plate (USA, Zimmer Inc)
Fig. 2. Electric myofascial impactor (gun) used by the physiotherapist. The fascia guns we use are manufactured in China. It typically produces three types of vibration (low, medium and high), and its probe transmits physical vibration waves to the body’s soft tissues, which are used by physiotherapists to relax and loosen the adhesion of the patient’s limbs and back. It can’t hit the joints, head, abdomen. Do not use for more than 10 minutes at a time to avoid soft tissue damage.
Fig. 3. Abdominal computer tomography (CT). Arrow: haematom; horizontal view.
Fig. 4. Computer tomography (CT) scan of the abdomen; sagittal view.
A spring coil was used to stop the haemorrhage. Laboratory tests conducted 24 h after the operation indicated that the patient’s blood haemoglobin level had decreased from the preoperative level of 9 to 6.7 g/l. The patient also had abdominal distension and worsening back pain. After consulting the vascular surgeon, a repeat angiography was performed and no leakage of contrast medium was detected. Laparotomy was performed and the extensive haematoma at the base of the retroperitoneal space was cleared. After the second operation, the patient was transferred to the intensive care unit (ICU), and returned to the general ward 2 days later. The patient was then transferred to the rehabilitation ward.
Spontaneous retroperitoneal haemorrhage
Spontaneous RPH seldom occurs alone and is often accompanied by other complications involving the abdominal organs. The retroperitoneum is adjacent to several organs, and for the purpose of simplification, it is divided into 3 regions; the upper abdomen region, the kidney region, and the pelvic region (2). RPH occurring in any region is usually related to the adjacent organs or blood vessels. For example, haematoma in the upper abdomen region often originates from the pancreas and/or duodenum.
Acute pancreatitis. This is a common cause of acute abdomen, presenting with symptoms of acute epigastric pain, nausea, vomiting, fever, and increased serum levels of amylase. In acute stages of inflammation, pancreatic enzymes may reach the adjacent retroperitoneum, causing RPH (3, 4).
Haemorrhagic diseases. Haemophilia is caused by deficiency of coagulation factors and mainly manifests as haemorrhage. Breath-holding during exertion, and the subsequent increase in abdominal pressure, can cause RPH in patients with haemophilia (5). Evans syndrome is characterized by the simultaneous or sequential occurrence of autoimmune haemolytic anaemia and immune thrombocytopaenic purpura. Similar to patients with haemophilia, patients with Evans syndrome have an obvious bleeding tendency, particularly haemorrhage in the abdominal cavity, with strong concealment. In such cases, the diagnosis may often be missed or mistaken due to the lack of sufficient data from clinical reports (6).
Tumour. Moore et al. reported 1 case of retroperitoneal massive haemorrhage with metastatic mixed germ cell tumor. They believes that certain tumors have usually proliferation, excessive vascularization with subsequent ulceration, necrosis, and eventually bleeding (7). Figueroa-Jiménez et al. reported a rare case of RPH resulting from a splenic artery aneurysm (8), wherein the patient remained asymptomatic for life, and rupture of the aneurysm resulted in death (9).
Renal failure and dialysis. Although RPH in renal failure and patients on dialysis has generally been reported as individual cases, several such reports have been published in the literature (10–13). In particular, the incidence of RPH is high in patients undergoing chronic haemodialysis, while also receiving anticoagulant therapy (14). This high incidence may be attributed to the location of the kidney and the pathophysiological changes associated with renal failure, similar to those occurring in pancreatitis.
Cirrhosis. Bisceglie et al. (15) reported 2 cases of RPH in patients with cirrhosis. RPH may often occur in the late stages of cirrhosis due to distension of the lateral branches of the peritoneum vein (a branch of the portal vein) with an increase in portal vein pressure.
Rare diseases. RPH has been reported to occur in some rare diseases. It is vital that clinicians are aware of this possibility. Menkes’ disease, also known as curly hair syndrome, is a rare congenital disorder of copper metabolism, which is acquired through X-linked recessive inheritance. Weng et al. reported a case of MD complicated with retroperitoneal hematoma (RPH), which is very rare in children. Spontaneous RH in children mostly occurs as a complication of other diseases (16).
Non-spontaneous retroperitoneal haemorrhage
Iatrogenic injury. In a retrospective analysis of 9,585 patients who had undergone femoral artery catheterization, Kent et al. identified 45 cases (0.5%) of RPH (17). The incidence rate of RPH was low compared with that of other complications (17). Most patients undergoing interventional therapy need postoperative anticoagulant therapy. RPH caused by puncture may often be hidden and atypical in presentation. In patients undergoing procedures while also receiving anticoagulant therapy, RPH can be severe. Therefore, RPH is an important risk factor associated with anticoagulant therapy in such cases.
Anticoagulant drugs. The use of anticoagulants has been long identified as one of the most direct causes of RPH. Palleja et al. have shown that 0.1–6.6% of patients receiving anticoagulant therapy developed retroperitoneal haematomas (18, 19). Forfar et al. have reported that RPH is one of the most serious complications of haemorrhage after anticoagulation (20), even in the absence of the overuse of oral anticoagulants (21). Although some anticoagulants have been found to be safer and more convenient to use than traditional drugs (e.g. warfarin), there is still a lack of long-term observational data regarding the risk of haemorrhage in patients receiving anticoagulant therapy.
Trauma. RPH is often reported in cases of fracture of the pelvis or lumbar vertebrae (22). In such cases, RPH can be confirmed by CT. Patients with the possibility of progressive haemorrhage should be monitored closely. Due to the close proximity of the retroperitoneum and the pelvis and lumbar vertebrae, patients may be unable clearly to describe the nature of pain. Therefore, assessment with CT or abdominal ultrasound is necessary to detect signs of RPH.
Factors that may have led to RPH in the current patient were delayed haemorrhage following surgery for pelvic fracture, long-term use of anticoagulants before and after surgery, and use of a myofascial gun.
The patient had discontinued anticoagulants 3 months prior to the occurrence of RPH, but they may have accumulated, exerting a continuous influence on blood flow stability (23). The patient reported intermittent abdominal pain after the operation, which was probably the result of a local inflammatory reaction and adhesion of the retroperioneal tissue after surgery. The high vibration frequency of the myofascial gun may be transmitted to the deep tissues via areas with thick fat deposits, such as the abdomen, resulting in tearing and bleeding at the adhesion site of the retroperitoneal membrane. Inoue et al. reported the occurrence of RPH following extracorporeal shock wave lithotripsy (ESWL) (24). This kind of physical shock has a serious effect on the retroperitoneal vascular tissue, particularly in patients who are taking anticoagulant drugs, and may even be fatal.
In order to determine the cause of haemorrhage and establish a proper treatment strategy, it is necessary to identify whether the RPH is spontaneous or non-spontaneous by detailed history-taking and careful imaging studies. Nicolsky et al. found that nearly one-fifth of patients (n = 10,440) who had undergone coronary intervention had symptomatic peripheral arterial insufficiency (25). Compared with patients without peripheral artery disease, these patients had a higher incidence of RPH after coronary intervention, which is an iatrogenic cause of haemorrhage.
Initial clinical judgement as to whether RPH is spontaneous or non-spontaneous may be based on whether the patient has had an injury or iatrogenic intervention. However, this approach ignores existing diseases and previous hidden injuries, which are also important. Determining whether the haemorrhage is spontaneous or non-spontaneous may directly affect the treatment plan and prognosis. Some investigators have found that only 16% of cases of peritoneal haematomas require intervention or surgical intervention (26); however, the study did not classify cases based on spontaneous or non-spontaneous RPH. For traumatic or iatrogenic RPH, the amount of haemorrhage is often large, and the risk of haemorrhagic shock is high.
In this case of RPH the patient had a history of pelvic surgery and anticoagulant therapy. His level of physical activity had increased gradually during the later stages of rehabilitation, and he had undergone vibratory stimulation of deep muscles with a myofascial gun as part of physiotherapy. Together, these factors resulted in occurrence of delayed RPH. In-depth analysis of the aetiology of RPH in this case suggests that the main causes of the haemorrhage were haemodynamic changes, stress, and inflammatory reaction.
This case indicates that delayed RPH could be caused by multiple factors. Careful observation and monitoring of the patient is essential to ensure early identification and correct treatment of RPH in patients who have undergone surgery for pelvic fracture.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize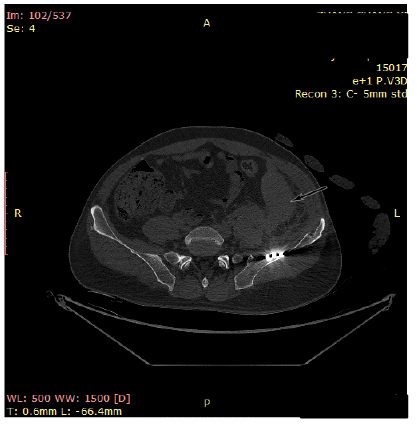 Click to show fullsize
Click to show fullsize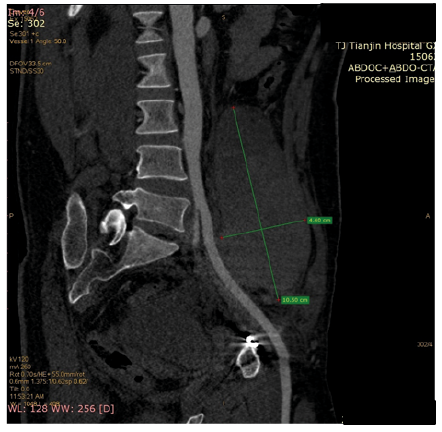 Click to show fullsize
Click to show fullsize