
1Department of Rehabilitation Medicine (Neurology), Salford Royal Hospital, Salford, UK
2Division of Neuroscience and Experimental Psychology, University of Manchester, Manchester, UK
3Academic Department of Rehabilitation Medicine, University of Leeds, Leeds, UK
Objectives: Hyper-Acute Rehabilitation Units (HARUs) provide multidisciplinary rehabilitation to patients with acute neurological injuries. This includes managing patients with tracheostomies. This is the first study of its kind to examine clinical outcomes in patients with brain injury and tracheostomy managed in a HARU.
Methods: Retrospective analysis of clinical outcomes in tracheostomy patients admitted to a HARU over a 2-year period.
Results: A total of 208 patients were admitted to the HARU, of whom 99 (60 males and 39 females) had a tracheostomy either at admission or during their stay in the HARU. Mean Glasgow Coma Scale
score at admission was 11 (range 5–15) and at discharge was 13 (range 8–15). Mean Functional Independence Measure and Functional Assessment Measure (FIM+FAM) score improved from 52 at admission to 95 at discharge. Mean FIM+FAM cognitive admission cognitive sub-score improved from 23 to 42, and mean motor sub-score from 29 to 42. Changes in scores were deemed to be clinically significant as per thresholds reported in the literature. Of the total patients in this study, 79% were successfully decannulated and 21% needed long-term tracheostomy.
Conclusion: Patients with tracheostomy following brain injury can be appropriately managed in a HARU and show clinically significant improvement in functional outcomes.
Key words: brain injury; intensive care; weaning; decannulation; tracheostomy.
Accepted Oct 30, 2019; published Dec 19, 2019
JRM-CC 2019; 2: 1000024
Correspondence address: Manoj Sivan, Division of Neuroscience and Experimental Psychology, Clinical Sciences Building, Salford Royal NHS Foundation Trust, Salford, Stott Lane, M6 8HD, UK. E-mail: manoj.sivan@manchester.ac.uk
A Hyper-Acute Rehabilitation Unit (HARU) provides rehabilitation to patients with sudden neurological injury, such as traumatic brain injury or stroke. In order to maintain a safe airway some of these patients have an artificial tube inserted into the trachea through an opening in the neck. This procedure is called a tracheostomy.This study analysed outcomes in tracheostomy patients admitted to a HARU over a 2-year period. A total of 208 patients were admitted to the unit, of whom 99 had a brain injury and had had a tracheostomy, either at admission or during their stay in the HARU. Functional activity, measured using Functional Independence Measure and Functional Assessment Measure (FIM+FAM) scales, showed significant improvement in both physical and mental ability in these patients. The tracheostomy tubes were removed successfully in 79% of patients as they became more independent and able to maintain their airway. However, long-term tracheostomy was needed in 21% of patients. This study shows that patients who have a tracheostomy following an acute neurological injury can be managed appropriately in a HARU and improve in functional ability.
A tracheostomy is one of the most commonly performed procedures in an intensive care unit setting, to assist weaning from ventilator support and provide airway support for patients with impaired respiratory function or those with an obstructed upper airway (1–3). Tracheostomy is useful for secretion management and is used for airway protection in patients with impaired swallowing reflexes, such as those with neurological injuries (4). After the acute injury has been dealt with (e.g. by evacuation of bleed or decompressive craniectomy) and the patient starts to show signs of recovery of reflexes, gradual weaning, with the aim of decannulation, can be commenced.
The increasing number of tracheostomies performed has led to an increasing number of patients being discharged to non-specialized settings (3). There is often difficulty in identifying teams or individuals in such settings who have the necessary skills to provide tracheostomy care for these patients. They would need to be adequately trained in all aspect of tracheostomy care, including humidification, suction and stoma care, weaning protocols and dealing with emergency situations (5). LeBlanc et al. (6) demonstrated in their study that the implementation of a “multi-disciplinary tracheostomy team” had positive clinical benefits for patients with traumatic brain injury (TBI), including reduced length of stay (LOS) and decreased time to decannulation (6, 7). There is also evidence for better recovery and improved outcomes in patients with a TBI with early rehabilitation input (with tracheostomy weaning as part of this) (8).
Tracheostomy weaning care for patients with neurological injuries in settings outside the intensive care unit (ICU) in the UK National Health Service (NHS) is generally provided by a critical care outreach team. HARUs are specialist units based within tertiary care hospitals which can provide tracheostomy care as part of the rehabilitation programme. Patients admitted to these units are still at an early stage in their rehabilitation pathways and have ongoing medical or surgical needs (9). Although currently few in the UK, more such units are being set up to meet the needs of these patients. The HARU in this study is part of a rehabilitation network that is within a metropolitan county and combined authority area within the UK. The unit manages patients with acquired brain injury, either traumatic or non-traumatic.
Tracheostomy weaning and management in these units is led by a Rehabilitation Medicine (RM) consultant, alongside a multi-disciplinary team (MDT), comprising specialist neuro-physiotherapists, speech and language therapists, occupational therapists and rehabilitation nurses. Prior to the set-up of this HARU, patients were managed disjointedly by different group of clinicians and lacked a streamlined specialist management pathway. This study retrospectively analysed all patients admitted to the HARU with brain injury and tracheostomy. Patients’ functional outcomes were measured by the MDT team using the FIM+FAM scoring method, which has been shown to be valid to measure disability in brain-injured or neurorehabilitation patients in an inpatient setting (9–11). As far as we are aware, although there are published studies on the merits of early rehabilitation and decannulation (8), there are currently no published studies on functional and tracheostomy outcomes from any HARU, particularly in relation to patients with acquired brain injury.
Understanding the outcomes in patients admitted to the HARU with brain injury and tracheostomy will help clinical teams to evaluate the quality of care for these patients in such units, and may support the need for such units in any tertiary care neuroscience setting in order to streamline the care of these patients with complex needs.
Setting
The HARU in this study is based in a tertiary care neurotrauma centre and is one of the few units in the UK that manages patient with an active tracheostomy weaning plan. It accepts patients who have been stepped down from ICU, neuro-high dependency unit (NHDU), acute neurosurgical or neurology or spinal surgery wards. The unit accepts inter-hospital transfers from acute neuro-wards (and occasionally spinal ward), including patients with a tracheostomy. The unit has a level 1 United Kingdom Rehabilitation Outcomes Collaborative (UKROC) status, providing rehabilitation for patients with highly complex rehabilitation needs that are beyond the scope of local and district specialist services (9). The service is supported through NHS England specialist commissioning and is delivered through co-ordinated service networks planned for a regional population of 1.5 million. The MDT of the unit comprises rehabilitation medicine physicians, specialist neuro-physiotherapists, speech and language therapists, occupational therapists, rehabilitation nurses, neuropsychologists, rehabilitation co-ordinators, support workers and a social worker (Fig. 1). Patients in the HARU receive rehabilitation on a daily basis, from different practitioners, throughout the week. Patients are given worksheets and are assisted by therapist assistants throughout the week. The availability of specific therapy rooms, equipment and plinths aids the rehabilitation process. Patients are also under the care of a rehabilitation physician. In comparison, patients in the general acute wards or ICU only receive rehabilitation intervention once a week, for an hour at best.
Tracheostomy weaning is an essential part of the rehabilitation process that is normally initiated in the ICU or NHDU, when the patient is deemed clinically ready. If the patient is transferred or stepped down to other settings, the weaning is initiated in the acute neurosurgical or neurology ward supported or supervised by the critical care outreach team. When weaning is commenced in the HARU, it is initiated and monitored by the multi-disciplinary team, which consists of a rehabilitation medicine consultant, specialist trainee registrar, physiotherapist, speech and language therapist, specialist nurse and rehabilitation coordinator. There is a dedicated tracheostomy ward round every week to address the needs of these patients. In the HARU, all patients participate in a standard tracheostomy weaning protocol, which involves stages such as using speaking valves, gradual capping of the tracheostomy, and subsequent decannulation.
Fig. 1. Flowchart of admission and discharge into the Hyper-Acute Rehabilitation Unit (HARU). An Intermediate Neuro-Rehabilitation Unit (INRU) is a rehabilitation unit that cares for patients with neurological diagnosis and rehabilitation needs. Patients need to be medically stable and able to participate in daily therapies. Patients with tracheostomies are generally not accepted. A&E: Accident and Emergency Department; NHDU: Neuro-High Dependency Unit; Dist gen hosp: District General Hospital; NH: Nursing Home; Residential: Residential Home; FU: follow-up.
Outcome measures
The Glasgow Coma Scale (GCS) gives an indication of consciousness level in response to defined stimuli and related to the seriousness of the brain injury. Severity of brain injury is categorized as mild (score 13–15), moderate (score 9–12) or severe (score 3–8) (12, 13). The functional ability of patients at admission and discharge is measured using the Functional Independence Measure (FIM), together with the Functional Assessment Measure (FAM). FIM+FAM has a scoring system for all 30 items from 1 to 7 (where 1 = complete dependence and 7 = fully independent) and comprises a 16-item motor subscale and 14-item cognitive subscale (14). A higher FIM+FAM score indicates greater independence or functional ability. Admission FIM+FAM is performed 7–10 days after admission into the HARU, allowing adequate time for members of the MDT to assess the patient and perform a fair assessment. Discharge scoring is performed within 7 days of discharge by the same team. The lowest possible scoring would be 30 for a patient who is dependent for all needs.
Data collection and analysis
Electronic notes for all patients with tracheostomy during their HARU stay were reviewed. Local institutional regulations regarding the review of patient’s notes and collection of data were followed for this study. The collection of data was approved by an institutional quality improvement project regulatory team. All data collected and evaluated were anonymized with no patient identifying details, in line with data protection policies.
A 2-year period was analysed. Inclusion criteria were: presence of tracheostomy either at admission to the unit or insertion during the stay in the unit and a diagnosis of brain injury. Patients were followed up until they were discharged from the HARU. The type of neurological insult, brain scan images and subsequent management were reviewed. The indication for the tracheostomy insertion was identified. Factors that affected the weaning process, such as respiratory secretion and oropharyngeal secretion management, were recorded. Patient’s GCS on admission and discharge and duration of stay in the hospital and the unit were also included. Patient’s FIM+FAM scores on admission and prior to discharge were extracted from the notes.
Data collection was performed by author KM and review and analysis of data were performed by authors LC, KM and MS. All authors contributed to the interpretation of data and writing the manuscript. Statistical analysis was performed using Microsoft Excel. Quantitative data are presented as means and/or medians and standard deviation. Factors affecting the success of weaning are presented in relation to the number of patients and percentages.
A total of 208 patients were admitted to the HARU over the 2-year period. There were 112 patients who met the inclusion criteria of having a tracheostomy upon arrival at the HARU or a tracheostomy placed during their stay in the HARU. Five patients (out of 112) were excluded as they did not sustain a brain injury (2 patients with spinal injury, 2 with Guillain-Barré syndrome, and 1 with critical illness myopathy). Eight patients were subsequently excluded from the data interpretation, as 5 died during this period, 2 were transferred to a different hospital, and 1 remained as an inpatient at the end of this period. Therefore, a total of 99 patients were included for analysis. The demographics of the patients are summarized in Table I.
Table I. Patient demographics
At the end of the 2-year period, 78 patients were successfully decannulated and 21 patients remained with a tracheostomy. The reasons for long-term tracheostomy were increased secretion load, recurrent aspiration pneumonia and other causes (Table II).
Table II. Reasons for long-term tracheostomy
The comparison between outcomes in patients who were successfully decannulated (D) and those who required long-term tracheostomy (LT) is summarized in Table III and Table IV.
Table III. Outcomes in patients who were successfully decannulated and those who required long-term tracheostomy
Table IV Further subgroup analysis patients’ Glasgow Coma Scale among the decannulated and long-term tracheostomy group
The mean GCS for all 99 patients had changed from 11 (range 5–15, standard deviation 2.3) at admission to 13 (range 8–15, standard deviation 2.3) at discharge (p < 0.001). Both patient groups D and LT improved their GCS from admission to discharge. The admission GCS was higher in the D group compared with the LT group (p < 0.001). Further subgroup analysis within the D and LT groups revealed that 49% of patients in the D group had a mild injury admission GCS, whilst 9% of the D group had severe brain injury. All patients with mild brain injury were successfully decannulated. Seventy-one percent of the LT group had mild brain injury (χ2 = 17.964 (df = 2), p < 0.001).
The mean FIM+FAM for all patients improved from 52 on admission to 95 on discharge. The mean total cognitive sub-score improved from 23 to 42, and the mean total motor sub-score from 29 to 53. The changes in FIM+FAM scores were deemed clinically significant as per thresholds of 8 for the motor subscale and 7 for the cognitive subscale, as reported previously (14).
Paroxysmal sympathetic hyperactivity (PSH) is a condition specific to the brain-injured patient. PSH was more common in the LT group compared with the D group (6% vs 47.62%). LOS was greater in patients with a diagnosis of PSH.
The discharge destinations of patients is summarized in Table V.
The majority of patients in D group (n = 78) were discharged to an INRU, compared with the majority in LT group (n = 21) who were discharged to a nursing home or for slow stream rehabilitation. This reflects the provision of local services within the region.
Table V. Discharge destinations of patients
This observational service evaluation study highlighted that, in general, patients who were transferred to a HARU had clinically significant functional improvements, as measured by their FIM+FAM scores. Also, 79% of patients were successfully weaned and decannulated from their tracheostomy. This helped to facilitate discharge planning and presumably reduced the complexity of long-term care for these patients.
The common reasons for delay in tracheostomy weaning and decannulation were increased secretion load and chest infections, as observed in other studies (15, 16). Managing these problems requires a MDT of professionals trained in tracheostomy care, which includes a medical team, physiotherapists, speech and language therapists and specialist nurses. The MDT team of the HARU is well placed to manage these problems and enable a timely and closely monitored tracheostomy weaning programme, which can be integrated into the physical and cognitive rehabilitation programme. In addition, rehabilitation medicine physicians are trained to treat and manage secretion load, including the skill of performing botulinum toxin injections to the salivary gland, should this be required. The added benefit of the HARU managing these patients is that intensive care and acute neurosurgical and neurology wards are able to transfer such patients with rehabilitation needs to the HARU and use their beds to focus on their usual workload of acute neurological emergencies. It is recommended that a HARU team should be involved early in the rehabilitation pathway of patients with severe neurological injuries. Previous studies have shown that early neuro-rehabilitation also aids decannulation in patients with severe acquired brain injury (8).
The patients with severe injury GCS at admission had higher rate of long-term tracheostomy. This is in keeping with other studies (15–17). These patients remain as inpatients for a longer duration in any acute ward and need care in a dedicated rehabilitation unit where the complexity of care (including managing the expectations of family and friends) needs to be managed. This requires input from an expert MDT such as that available in a HARU. The transfer of these patients from the HARU to long-term care facilities is likely to be well organized and smooth compared with transfer from acute neurological wards.
The HARU patients in the LT group had a longer LOS, by a mean of 174 days, compared with those in D group. The recommended LOS for this patient group within specialist prolonged disorders of consciousness neurorehabilitation services is 3–4 months (90–120 days) (5). Patients in D group had a mean LOS within the recommended guidelines, at 97 days. Patients in LT group had a mean LOS longer than the recommended guides, at 271 days. When further examined D group + PSH LOS was 172 days and LT group +PSH LOS was 293 days. PSH appears to increase the length of tracheostomy wean and LOS. PSH + LT tracheostomy were the most significant factors increasing the LOS (293 days). PSH has been shown to prolong tracheostomy wean in patients with severe TBI (18). Majority of LT tracheostomy patients (90%) required either slow stream rehabilitation or a specialist nursing home, but these services are sparse in the UK(6). These factors explain the increased LOS in the HARU.
Staying in the HARU enabled a high discharge rate to intermediate neurorehabilitation units (INRU). It can be argued that the unit enabled a comprehensive rehabilitation programme, which included a timely tracheostomy weaning programme and improved patients’ functional status to merit a place in INRUs. INRUs have strict acceptance criteria, based on manageable complexity of care and rehabilitation potential. The Intensive Care Society standards recommend that patients are only discharged to wards or units where adequate tracheostomy management is available (8), which is not normally the case in most INRUs. Many patients in thus study would therefore have not been accepted in these units if they had been referred from acute wards without decannulation of their tracheostomies. A HARU can successfully bridge this gap. This study showed that 79% of patients in the HARU were decannulated, and that the majority of this group (91%) progressed to further rehabilitation units (INRU 60 patients, slow stream rehabilitation 3 patients or home 8 patients).
Limitations
This observational study has some limitations. Firstly, as this is an uncontrolled study, a comparison arm of routine care is not available to demonstrate whether care in the HARU provided greater functional returns and more rapid decannulation rates compared with routine care. This would be an interesting aspect for future research. Secondly, this study does not provide cost-effectiveness analysis comparing HARU unit and routine care; how-ever, this could be explored further in future using the economic analysis of UKROC data (19). Thirdly, a majority of patients in this study (62%) were discharged to local INRUs, and presumably they would continue to have further functional gains in those units. This study examines the gains in HARU alone and does not analyse the functional gains over the entire rehabilitation pathway. Finally, such units are expensive to run and require additional specialist staff. Whether the additional costs match the enhanced outcomes needs further research.
Conclusion
This study highlights the importance of having a HARU in a tertiary care neurosciences unit. It enables a streamlined dedicated pathway for patients with severe neurological injuries, particularly those with respiratory problems needing insertion of a tracheostomy. The care in a HARU provided by a skilled MDT leads to clinically significant functional improvements for patients, enables a timely weaning plan as part of their rehabilitation programme, and enables discharge to destinations that are preferred by patients, their families and healthcare professionals. HARU provides an appropriate link between acute intensive care and subacute intermediate rehabilitation units in the community, and ensures that timely rehabilitation and maximal functional gains continue to occur in the golden window period after neurological injury.
The authors would like to thank all of our MDT colleagues for their hard work and valuable input towards the care provided in the unit.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize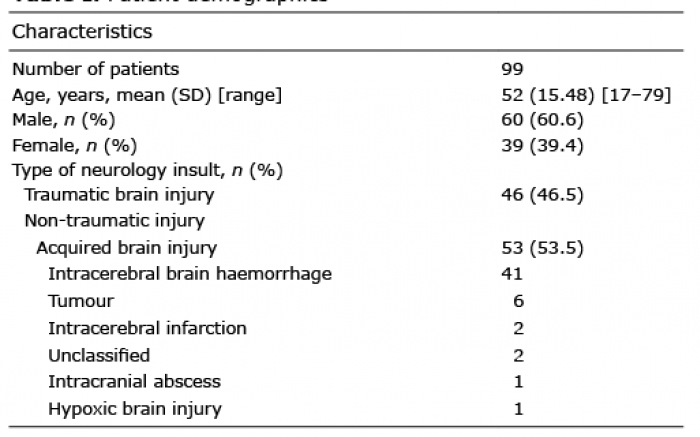 Click to show fullsize
Click to show fullsize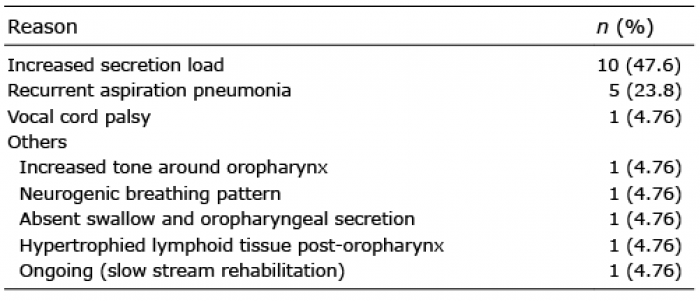 Click to show fullsize
Click to show fullsize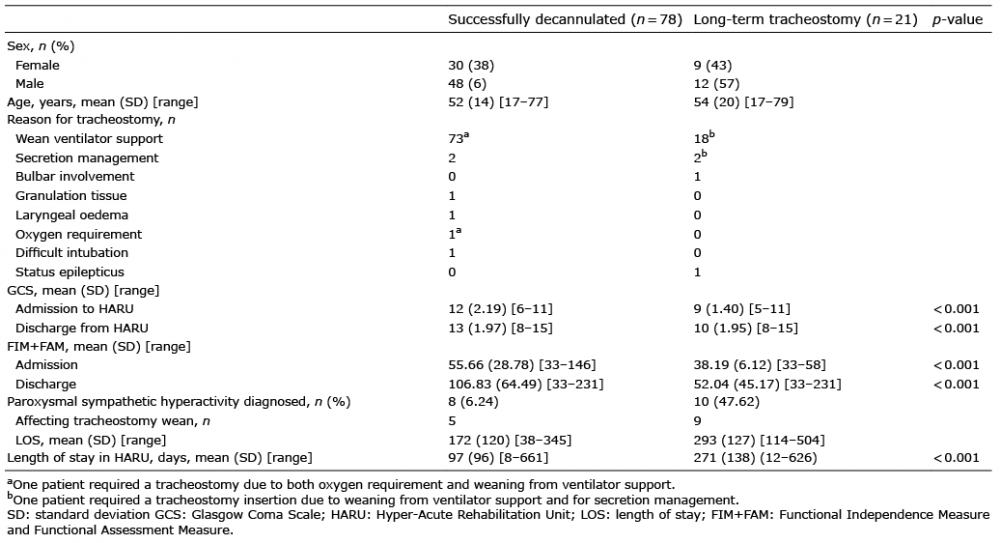 Click to show fullsize
Click to show fullsize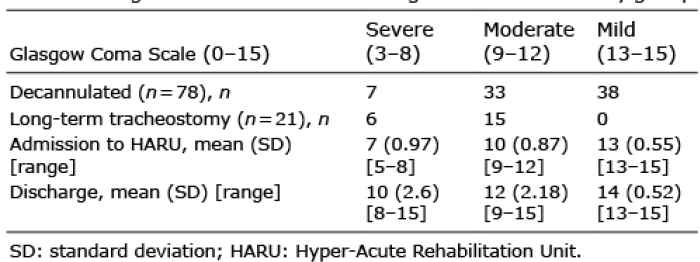 Click to show fullsize
Click to show fullsize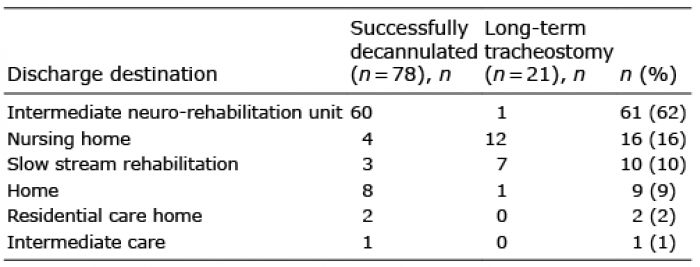 Click to show fullsize
Click to show fullsize