
1Adelante Centre of Expertise in Rehabilitation and Audiology, Hoensbroek, The Netherlands
2Department of Rehabilitation Medicine, Research School CAPHRI, Maastricht University, Maastricht, The Netherlands
3Libra Rehabilitation and Audiology, Eindhoven/Weert and 4Research Group Experimental Health Psychology, Maastricht University, Maastricht, The Netherlands
Objective: Painful diabetic neuropathy is associated with low quality of life, depression and anxiety. Patients are limited in their performance of activities of daily living due to fears related to their condition. Treatment modalities are needed to help patients cope with their pain and pain-related disability. Exposure in vivo is an effective treatment in other chronic pain syndromes, increasing patients’ functional ability and quality of life. This paper presents an Exposure in vivo treatment protocol for patients with painful diabetic neuropathy.
Protocol: An 8-week Exposure in vivo treatment protocol was specifically adapted to the needs and risks of patients with painful diabetic neuropathy. New screening tools were developed for patients with PDN; the Painful Diabetic Neuropathy Anxiety Rasch-Transformed Questionnaire (PART-Q30) identifies specific fears related to painful diabetic neuropathy (e.g. fear of hypoglycaemia); and a customized version of the Photograph-series Of Daily Activities (PHODA-PDN) detects fear-eliciting activities related to the condition in individual patients. During Exposure in vivo, catastrophic interpretations regarding painful stimuli are challenged and corrected, thereby diminishing pain-related fear and enabling the patient to re-engage in activities of daily living. An interdisciplinary team provides Exposure in vivo in 1-h sessions twice a week.
Discussion: To the best of our knowledge, this treat-ment protocol is the first intervention using Exposure in vivo specifically adapted to the needs and risks of patients with painful diabetic neuropathy.
Key words: diabetic neuropathies; physical and rehabilitation medicine; quality of life.
Accepted Mar 6, 2019; published July 15
JRM-CC 2019; 2: 1000015
Correspondence address: Charlotte C. M. van Laake-Geelen, Adelante Centre of Expertise in Rehabilitation and Audiology, PO Box 88, NL-6430 AB Hoensbroek, The Netherlands. E-mail: c.laake@adelante-zorggroep.nl
Painful diabetic neuropathy is associated with low quality of life, depression and anxiety. Treatment modalities are needed to help patients cope with their pain and pain-related disability. Exposure in vivo is an 8-week biopsychosocial rehabilitation treatment that aims to restore a normal pattern of daily functioning. During Exposure in vivo, catastrophic interpretations regarding painful stimuli are challenged and corrected, thereby diminishing pain-related fear and enabling patients to re-engage in activities of daily living. An interdisciplinary team provides Exposure in vivo in 1-h sessions twice a week. Current Exposure in vivo treatments are designed for chronic pain conditions that generally have no medical risks or restrictions regarding physical activity. To the best of our knowledge, this treatment protocol is the first Exposure in vivo intervention specifically adapted to the needs and risks of patients with painful diabetic neuropathy. New screening tools were also designed for patients with painful diabetic neuropathy.
The increasing incidence of diabetes mellitus represents a serious challenge for the medical profession worldwide. Diabetic neuropathy (DN) is present in up to 50% of all patients with chronic diabetes and is a major cause of morbidity and mortality (1). In the USA alone, the annual costs associated with DN are USD 10.9 billion (2).
Up to 25% of patients with diabetes develop painful diabetic neuropathy (PDN), characterized by pain, paraesthesia and sensory loss (3). Sensory loss can lead to the development of pressure ulcers (PUs), balance impairments, an altered gait with a potentially increased risk of falling (4) and impaired levels of physical activity (5). Reduced mobility can lead to restrictions in daily and social activities, dependency on others, and depression, resulting in reduced quality of life (QoL) (6). Depression, in turn, can amplify diabetic complications related to suboptimal glycaemic control (7).
An increasing number of studies has shown that a substantial proportion of patients with diabetes with PDN experience anxiety and fears, such as fear of pain, falling, and disturbed glucose regulation, and consequently avoid physical activity (8). Current care, mostly based on pharmacotherapy and physical training, appears to ignore the debilitating role of those fears in increasing physical activity and regaining normal daily functioning (9). It is well known that increasing physical activity in patients with DM has favourable effects on diabetes-related outcomes (10). However, dropout rates in physical exercise programmes are high, with rates up to 45% (11). An interdisciplinary therapeutic approach has therefore been recommended in order to improve daily life functioning (12).
Since patients with PDN frequently share the comorbidities of depression and fear (and as a consequence disability) with other chronic pain populations (13), it seems appropriate to integrate the knowledge obtained in populations with other pain syndromes into the field of PDN. An example of a cognitive behavioural treatment modality for patients with chronic pain is Exposure in vivo (EXP), which is based on the principles of classical conditioning (14). EXP aims to decrease pain-related disability by specifically targeting irrational thoughts and fears about pain and its consequences (15). EXP has been shown to be effective in improving functional ability and QoL, and to reduce pain-related fear and the perceived harmfulness of physical activity in patients with various chronic pain conditions (14, 16–18). EXP has also shown to be cost-effective (19, 20).
We have developed an 8-week EXP treatment adjusted specifically to the needs and risks of patients with PDN. The treatment has a multidimensional approach to improving daily functioning and includes methods derived from research in psychology, behavioural sciences, physical therapy, diabetes care and rehabilitation medicine. This interdisciplinary rehabilitation treatment involves physicians in rehabilitation medicine, physiotherapists, occupational therapists and psychologists. The EXP treatment protocol for patients with PDN is presented below.
All procedures performed in this study were in accordance with the Good Clinical Practice guidelines outlined by the International Conference on Harmonization, the ethical standards of the institutional and national research committee, and with the Declaration of Helsinki 1964 and its later amendments of comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
At the Adelante Centre of Expertise in Rehabilitation and Audiology, Maastricht University Medical Centre, EXP treatment is embedded in the usual care for patients with chronic pain syndromes, such as Complex Regional Pain Syndrome Type I (CRPS-I) and chronic low back pain, who report substantial pain-related fear, and fear of movement/(re)injury in particular (14, 15). The EXP treatment is highly structured, protocolled, individually tailored, and aims to restore a normal pattern of daily functioning (15). The current EXP treatments are designed for chronic pain conditions that generally have no medical risks or restrictions regarding physical activity. PDN, however, can present with potential risks for injury, PUs and/or hypoglycaemia, which can make EXP unsuitable for patients with PDN. Also, the behavioural and psychosocial processes in patients with PDN could differ from more unspecific chronic pain syndromes, such as chronic low back pain. We report here the theoretical framework and procedures that were used to customize the already existing EXP treatment to the needs and risks of patients with PDN.
In order to gain further insight into the perceptions, fears and consequences of PDN in daily life, the project started with a qualitative study (21). Three focus groups, each with 4 patients with PDN, were formed. Patients reported experiencing substantial pain, disability, polyneuropathy and diminished QoL. The consequences of PDN were physical (weakness, pain, physical restrictions), psychological (feelings of loss, feelings of depression, anger, sadness), and social (social withdrawal, isolation, work limitations, lower career opportunities). Furthermore, patients reported several fears related to diabetes and pain that could be important predictors of physical and social activities, such as fear of hypoglycaemia, (increased) pain, total exhaustion, physical injury, falling, loss of identity and negative evaluation. Fear seemed to be associated with different types of avoidance behaviour; patients avoided various activities, were less physically active and withdrew from performing activities (21). A second study in a cross-sectional design by our group showed that PDN was associated with catastrophic thinking, which in turn led to a perceived decline in physical activity, increased disability and reduced QoL (13). The identification of these fears enabled us to determine potential specific PDN-related targets for the behavioural intervention (5).
All procedures performed in this study were in accordance with the Good Clinical Practice guidelines outlined by the International Conference on Harmonization, the ethical standards of the institutional and national research committee, and with the Declaration of Helsinki 1964 and its later amendments of comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
At the Adelante Centre of Expertise in Rehabilitation and Audiology, Maastricht University Medical Centre, EXP treatment is embedded in the usual care for patients with chronic pain syndromes, such as Complex Regional Pain Syndrome Type I (CRPS-I) and chronic low back pain, who report substantial pain-related fear, and fear of movement/(re)injury in particular (14, 15). The EXP treatment is highly structured, protocolled, individually tailored, and aims to restore a normal pattern of daily functioning (15). The current EXP treatments are designed for chronic pain conditions that generally have no medical risks or restrictions regarding physical activity. PDN, however, can present with potential risks for injury, PUs and/or hypoglycaemia, which can make EXP unsuitable for patients with PDN. Also, the behavioural and psychosocial processes in patients with PDN could differ from more unspecific chronic pain syndromes, such as chronic low back pain. We report here the theoretical framework and procedures that were used to customize the already existing EXP treatment to the needs and risks of patients with PDN.
In order to gain further insight into the perceptions, fears and consequences of PDN in daily life, the project started with a qualitative study (21). Three focus groups, each with 4 patients with PDN, were formed. Patients reported experiencing substantial pain, disability, polyneuropathy and diminished QoL. The consequences of PDN were physical (weakness, pain, physical restrictions), psychological (feelings of loss, feelings of depression, anger, sadness), and social (social withdrawal, isolation, work limitations, lower career opportunities). Furthermore, patients reported several fears related to diabetes and pain that could be important predictors of physical and social activities, such as fear of hypoglycaemia, (increased) pain, total exhaustion, physical injury, falling, loss of identity and negative evaluation. Fear seemed to be associated with different types of avoidance behaviour; patients avoided various activities, were less physically active and withdrew from performing activities (21). A second study in a cross-sectional design by our group showed that PDN was associated with catastrophic thinking, which in turn led to a perceived decline in physical activity, increased disability and reduced QoL (13). The identification of these fears enabled us to determine potential specific PDN-related targets for the behavioural intervention (5).
PDN, aged > 18 years, who experience PDN-related fears and want to improve their level of activity and QoL. During the EXP treatment, patients with PDN are guided to learn and recognize which bodily sensations correspond to actual PDN-related risks, such as falling or current blood glucose levels. This is achieved by addressing thoughts and beliefs about bodily sensations in relation to actual measurements (e.g. clinimetric parameters, blood glucose levels pre- and post-treatment). Patients are then encouraged to increase the level of physical activity and apply their recognition skills in novel situations.
A treatment team, comprising a psychologist, occupational therapist, physiotherapist and a rehabilitation physician, all experienced in cognitive behavioural rehabilitation of patients with chronic pain, provides the EXP treatment. All team members should be trained in the risks and special needs of patients with diabetes. For example, if a patient has a high risk of developing an episode of hypoglycaemia, blood glucose levels should be measured pre- and post-treatment. Furthermore, the physician and team members must be aware of the risk of developing PUs and should be able to identify PUs in a timely manner.
The EXP treatment protocol comprises 3 parts: (i) intake by a rehabilitation physician; (ii) an extensive 1-day screening; and (iii) an 8-week EXP treatment. The full treatment is described below, and Table I provides an overview of the treatment protocol.
Table I. Schematic overview of the exposure in vivo treatment protocol for patients with painful diabetic neuropathy (PDN)
During the intake session, the rehabilitation physician takes a full medical history and assesses the current PDN-related complaints, risks and medication. Topics such as hypoglycaemic episodes, (risk of) PUs, and withdrawal/ reduction of pain medication are discussed.
Physical examination. A thorough physical examination of the lower extremity is performed. Peripheral polyneuropathy is checked and classified based on a standardized clinical neurological examination (CNE), in which a CNE score >5 indicates the presence of peripheral neuropathy and a score of >15 is considered severe peripheral neuropathy (22). The CNE score is determined by examining the Achilles tendon reflex, vibration awareness, sharp–blunt discrimination, touch sense, position sense at the hallux and manual assessment of extensor muscle strength of the hallux and flexor muscle strength of the foot in which all items are scored as either normal, impaired or absent (0–2 points). In addition, the scoring of light touch sense is related to the anatomical level below which it is impaired (toe, mid-foot, ankle, mid-calf and knee) (0–5 points). Previous research has shown that electromyography (EMG) and CNE scores resulted in the same diagnosis of distal polyneuropathy in patients with Diabetes Mellitus type II (DMII) (23, 24). In order to limit the risks for the development of PU’s, all patients are screened on PUs on their feet and on wearing adequate (orthopaedic) shoes. Walking ability is also tested. Based on the findings, the rehabilitation physician decides whether the patient can undergo the treatment. If the risks of injury are considered too high, the patient is excluded.
Elaboration on PDN-related fears. The rehabilitation physician screens for pain and diabetes-related fears that may inhibit the patient in performing daily activities. Based on the results of our qualitative studies, our group developed the Painful Diabetic Neuropathy Anxiety Rasch-Transformed Questionnaire (PART-Q30)(25).The PARTQ-30 is used to determine and quantify the impact of these specific disabling fears. This 30-item questionnaire can be applied easily in clinical practice and identifies the impact of specific disabling fears for the individual patient based on a relatively simple procedure (25). An elaboration of the current level of physical activities and participation in daily life is performed, according to the International Classification of Functioning, Disability and Health (ICF) model (26).
When PDN-related fears are present and cause limitations in participation in daily life activities, the rehabilitation physician will provide more information on the EXP treatment. Then, a short elaboration on possible treatment goals is performed. The patient is eligible for EXP treatment when he/she meets all 4 eligibility criteria: (i) there are PDN-related fears present that limit the patient in participate in daily life activities; (ii) the patient can formulate relevant treatment goals aimed at participation in daily life; (iii) the patient is committed and motivated to undergo the 8-week treatment programme; and (iv) there are no medical or psychological restrictions to participation (e.g. PUs, high injury risks, comorbid severe depression). Eligibility criteria are shown in Table II.
Table II. Eligibility criteria for exposure in vivo treatment
Screening consists of behavioural analyses by the psychologist, observation during activities and physical examination by the physical therapist, goal identification by the occupational therapist, a team meeting with the physician and all therapists, and an educational session with all team members and the patient, as described below.
Behavioural analysis. The aim of this session with the psychologist is to complete a behavioural, cognitive and psycho-physiological analysis of the problems associated with PDN. The Hospital Anxiety and Depression Scale (HADS) (27) and Pain Catastrophizing Scale (PCS) (28) are administered. The psychologist focusses on the patient’s catastrophic interpretations and fears related to PDN. The assessment also includes information about any antecedents (situational or internal, episodes of hypoglycaemia, recurrent falls, etc.) of pain-related fear and about direct and indirect consequences. The screening could also include other areas of life stress, as they might increase arousal levels and indirectly also fuel pain-related fear.
Observation during activities. The intake session with the physical therapist comprises a physical examination and an observation of the specific body movements during various activities. During this observation particular attention is paid to behavioural responses to specific activities (e.g. fear or avoidance). Whenever there are physical complaints or restrictions, these are noted in the medical file.
Goal identification. PDN can have profound effects on a patient’s life (5, 29) and the repeated interference with tasks that are essential to achieve various life goals and maintain a role in society, will impact on their sense of self, both their current self and, perhaps, more importantly, their plans and ideas about who they might become (30). The occupational therapist emphasizes that EXP does not primarily aim at reducing pain, but at the restoration of functional abilities through which patients’ capacity to live according to their life values can be restored. The patient is invited to formulate his/her own treatment goals together with the occupational therapist. The Canadian Occupational Performance Measure (COPM) is used by the occupational therapist to assess perceived limitations in activities and participation and to aid the goal formulation process. The patient and occupational therapist agree on One or more realistic and specific goals, which are formulated in positive terms. Activities (e.g. walking on uneven ground) that are in line with these goals (e.g. running errands) will be included in EXP.
PHODA-PDN. A listing of fear-eliciting activities is made using the Photograph-series Of Daily Activities (PHODA) (31, 32). This is a standardized method during which patients are requested to judge the perceived harmfulness of various physical daily life activities represented by photographs. Using a thermometer, the patient rates each picture between 0 and 100 regarding harmfulness (0 represents a situation that is not harmful for the lower extremity; 100 represents a situation that damages the lower extremity). Based on the associations between activities and expected negative outcomes (amputation, exhaustion, etc.), individually tailored behavioural experiments can be developed (31). For this treatment protocol, the PHODA for lower extremities was specifically adapted with additional photographs of PDN-related fears, resulting in the PHODA-PDN. These fears included fear of hypoglycaemia, falling, amputation, pain, exhaustion, injury, social isolation and loss of identity (13, 21).
Within the theory of classical conditioning, conditioned responses (CR), for example fears, occur when an unconditioned stimulus (US) is paired with a conditioned stimulus (CS). In PDN, the feared catastrophic consequence can be considered the US, while the activity in which the fear occurs is the CS. For example, “If I walk up a flight of stairs (CS), I will fall and break my leg (US)”. EXP treatment will then target the CS, providing a new experience for the patient: no catastrophic consequence occurs. In this example, the patient will experience that he or she can walk up a flight of stairs (CS) without falling and breaking his or her leg (no US). This newly learned association (CS – no US) will then increase the likelihood that the patient will no longer avoid walking up a flight of stairs in future situations. The original PHODA is designed to represent activities (CSs) that may be considered harmful (USs). However, the fears that were identified in our previous studies (fear of falling, hypoglycaemia etc.) are mostly feared consequences (USs), rather than specific activities (CSs). To overcome this issue, the PHODA-PDN is used in 2 phases. First, the patient identifies which PDN-related feared consequences (US) were present (e.g. fear of hypoglycaemia or of amputation). Then, the pictures of PDN-related fears are paired with pictures of activities from the original version of the PHODA (CSs). In this way, we could determine during which activity (CS) this PDN-related fear (US) occurred (e.g. walking on uneven ground).
Team meeting. After these sessions, there is a meeting with the treatment team, including the rehabilitation physician, without the patient. The team summarizes and elaborates on all the information that was obtained. In this meeting, the treatment team will make a final judgement as to whether the patient is eligible for EXP treatment. Directly after this, there is a final session with the patient, rehabilitation physician and physiotherapist, during which the patient will be informed about their eligibility for EXP treatment. If the patient is eligible, the screening finishes with an educational session.
Educational session. The patient receives an educational session with the rehabilitation physician, psychologist and physiotherapist. This educational session comprises a medical education on PDN and an explanation of the Fear-Avoidance-Model (FAM) and treatment rationale.
Medical education: the rehabilitation physician elaborates on the aetiology of diabetes and PDN and the medical consequences and risks, stressing the importance of adequate glycaemic control and physical activity. The aim of this educational session is to provide information and clarify any potential misconceptions regarding diabetes, pain and physical activity. Table III shows which topics should be addressed during this session. At the end of the session, the patient should be informed and aware of his/her medical condition on the one hand and, on the other hand, should realize that physical activity is important for good glycaemic control, and is not harmful when performed in the correct way.
Education of FAM: using their own individual symptoms, beliefs and behaviours in relation to their pain complaints, patients are given a careful explanation of the FAM (33) by the psychologist. Pain catastrophizing, pain-related fears, diabetes-related fears, avoidance and safety behaviours are discussed. The treatment team illustrates the paradoxical and dysfunctional effects of these coping strategies. In addition, the team stresses the risks of this behaviour, as it can lead to a higher risk of developing diabetes-related complications in the long-term. One of the major goals of the educational session is to help the patient understand that the consequences of PDN, in his/her case, are catastrophically overestimated and that physical activity is beneficial in the self-management of PDN and its complications.
Table III. Topics that should be discussed during the medical education session
The rehabilitation treatment commences after screening. In this 8-week programme, the patient receives 1-h sessions of EXP treatment, twice a week; a total of 16 sessions. During these sessions, the patient is systematically exposed to the tailored and fear-provoking activities. These fears can be diabetes- or pain-related and an elaboration will be done on the cognitions, fears and expectations of the patient regarding the feared activity. After this, the actual exposure to the feared activity will take place. For example, one activity that potentially induces both diabetes- and pain-related fears could be prolonged walking on uneven ground. By performing this activity for a longer period of time, it may activate the fear that an episode of hypoglycaemia may set in. The fact that a patient is walking on uneven ground can reinforce their fear of falling. During each exposure session patients are encouraged to engage in these fearful activities as much as possible until disconfirmation has occurred.
A member of the treatment team checks every activity on safety for patients with PDN, e.g. wearing adequate shoes before walking on uneven ground. Before every session, the patient is asked about current PUs. The treatment session can only start if the patient reports that their skin is in good condition. However, if the patient reports that PUs are present, or he/she is in doubt about the current condition of his/her skin, the therapist will inspect the feet. In case there are current PUs, the rehabilitation physician will be consulted and the EXP session will be halted. Because this treatment aims to decrease fears and increase self-management skills, we opted not to systematically screen the feet of all patients before and after every session, as we believe this will enhance hypervigilance and fear, rather than decrease it. In all patients who are insulin-dependent, glucose levels are measured pre- and post-treatment. In case fear of hypoglycaemia was specified as a limiting factor for physical activity in non-insulin dependent patients, these additional measurements can also be performed. In the final session, treatment effects are assessed and recorded using the PHODA-PDN, COPM and PART-Q30.
Team meetings and aftercare. During the EXP treatment, 2 team meetings take place (in weeks 3 and 7). During these meetings, the treatment team discusses the individual treatment goals and progression of the treatment. After each team meeting, the patient has an evaluation session with the rehabilitation physician to discuss progress and answer any questions that arise. After the final session, advice about future follow-up will be provided. Usually, aftercare consists of a meeting with the treatment team 6 weeks’ post-treatment and a final check-up with the rehabilitation physician 3 months after completion of the treatment.
This paper describes the treatment protocol of our 8-week EXP treatment, which was designed specifically for patients with PDN who are limited in in performing daily life activities by PDN-related fears. To the best of our knowledge, this treatment protocol is the first rehabilitation intervention based on the principles of classical conditioning for patients with PDN. The EXP intervention aims to increase physical ability and QoL by establishing a new positive association between previously expected negative outcomes during a specific activity. This intervention distinguishes itself by the fact that it aims to change behavioural patterns through physical and cognitive exposure of underlying cognitions and fears in specific daily life situations. Furthermore, this treatment protocol is based on a theoretical framework that integrates knowledge from the fields of psychology, behavioural sciences, physical therapy, diabetes care and rehabilitation medicine. Based on this knowledge, customized screening tools were developed and used. The result is a treatment rationale that provides an integrated approach to the individual needs and treatment goals for every single patient. The effectiveness of the EXP treatment protocol for patients with PDN is currently being tested in a repeated measures single case experimental design (SCED) with a 6-month follow-up period (ActiFeet study, ClinicalTrials.gov Identifier: NCT03066570).
This innovative 8-week EXP treatment protocol has been designed specifically for the risks and needs of patients with PDN. It aims to change behavioural patterns through physical and cognitive exposure of underlying cognitions and fears in specific daily life situations, thereby increasing levels of activity and QoL.
The present study was funded by the Dutch Diabetic Foundation, grant number 2010.13.1361.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize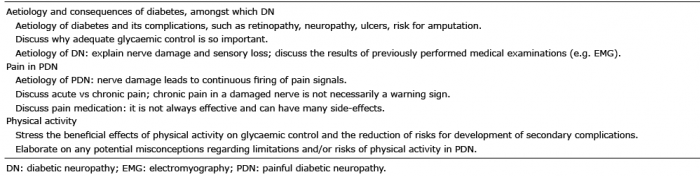 Click to show fullsize
Click to show fullsize