
1Epidemiology and Social Medicine, Institute of Medicine, The Sahlgrenska Academy at University of Gothenburg, SE-405 30 Göteborg, Sweden
2Centre for Equity in Health Care, Region Västra Götaland, Regionens Hus, SE-405 44 Göteborg, Sweden
3Centre for Specialist Care, Region Västra Götaland, Regionens Hus, SE-405 44 Göteborg, Sweden
4Pain Center, Frölunda Specialist Hospital, SE-422 21 Västra Frölunda, *present address: Smärthjälpen, Anders Personsgatan 12, SE-412 50 Göteborg, Sweden
Objective: Long-lasting pain is a challenge for patients’ everyday lives. The aim of this study was to examine how women and men who have participated in multimodal pain rehabilitation experience its impact in their everyday lives.
Patients and methods: Individual semi-structured interviews with 5 women and 3 men who had participated in multimodal pain rehabilitation at a clinic in Sweden, analysed using qualitative content analysis.
Results: Participants perceived that their “sense of control” increased, which had a positive impact in their everyday life. Sense of control consisted of 3 categories: importance of the patient–provider relationship, knowledge gained (especially on body functions and medication), and pain in a social context. Three results were discussed in particular: (i) a trustful patient–provider relationship based on confidence in the provider’s expertise was a prerequisite for pain acceptance; (ii) patients were aware of gender norms in healthcare; (iii) social support was not stressed as important to cope with pain.
Conclusion: The importance of patients’ confidence in the provider’s expertise and patients’ awareness about gender norms need consideration in terms of the patient–provider encounter. The value of social support for pain rehabilitation was found to be less important compared with previous research; this should be explored further.
Key words: chronic pain; gender; acceptance process; social support.
Accepted Dec 18, 2018; Published Apr 24, 2019
JRM-CC 2019; 2: 1000014
Correspondence address: Anke Samulowitz, Epidemiology and Social Medicine, Institute of Medicine, The Sahlgrenska Academy at University of Gothenburg, SE-405 30 Göteborg, Sweden. E-mail: anke.samulowitz@gu.se
We interviewed 5 women and 3 men with long-lasting pain and asked them how pain rehabilitation had affected their everyday life. The interviews were analyzed with a technique called “qualitative content analysis”. The participants experienced a trustful patient–provider relation, particularly trust in the providers’ expertise, as necessary for their pain acceptance. Pain acceptance, in turn, together with knowledge about body functions and medication, helped the participants to gain a sense of control over their pain and everyday life. Whilst highlighting a positive patient–provider relation, they saw gender norms as a potential obstacle that could affect relations with health care negatively. As research has emphasized social support as important to deal with pain in everyday life we asked about it. Surprisingly, social support was perceived as neither important to handle pain in daily life nor as affected by pain rehabilitation.
Between 12% and 50% of the European population experience self-reported chronic pain, according to cross-sectional surveys (1–3). In one survey, 19% of the adult population in 16 European countries reported moderate to severe pain for at least 6 months and at least twice a week during the month prior to the survey (3). Social consequences are human suffering and high public costs (3, 4). For instance, long-lasting pain lowers patients’ quality of life more than other diagnoses, such as multiple sclerosis and psoriasis (5). It is notable that the prevalence of pain is higher in women compared with men in cross-sectional surveys (1–3, 6), and women dominate most chronic pain syndromes (6, 7). It has not been possible to fully explain this preponderance of women (6–10). In addition to biological differences, psychosocial factors have been suggested to explain sex differences in pain prevalence, as well as in pain treatment (6, 7, 10). Gender bias in pain medication has been reported (6), as well as disrespect for women’s pain from healthcare personnel (9, 11).
Different factors promoting treatment of long-lasting pain have been highlighted by patients; for instance, to be treated with respect, knowledge about pain, body and exercise, and self-consciousness (12–16). In addition, the teaching of strategies for acceptance in pain rehabilitation programmes has been recommended (4). Although studies have shown that both women and men benefit from social support (13, 14), it has also been described as a women-dominated coping strategy (6, 8, 17).
Multimodal pain rehabilitation (MPR), a biosocial approach combined with physical, psychological and social interventions, has been suggested as a treatment option for chronic pain (4, 18–20). However, several researchers have highlighted the need to further study the impact of MPR in everyday life, including personal and social factors and, not least, the influence of gender (10, 21, 22).
The aim of this study was to examine how women and men who had taken part in MPR experienced its impact in their everyday lives. Patients’ reports are important in providing valuable knowledge and enabling the design of individualized rehabilitation programmes, suitable for all patients, both women and men.
The empirical data from this study consists of individual qualitative interviews. The study was initiated by a specialized pain rehabilitation clinic, with the aim of collecting information about patients’ experiences of MPR. The study was conducted independently from the clinic. One researcher (AS) had met the pain rehabilitation team in a quality improvement project prior to the study, but did not have any contact with the patients.
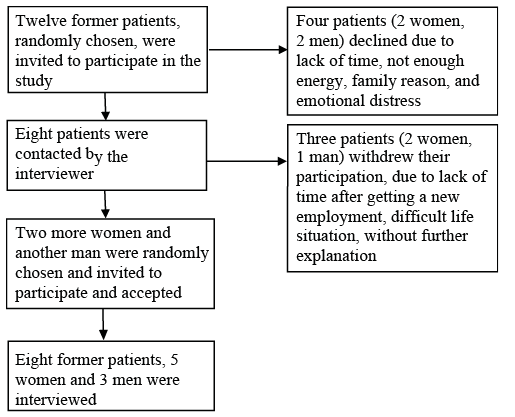
Five women and 3 men who had participated in MPR in Gothenburg, Sweden were interviewed. Inclusion criteria for MPR were: Swedish-speaking adults (16–67 years) with pain in the back, neck, shoulder and/or widespread pain for at least 3 months. More women were included in order to reflect the distribution of women and men in MPR. Inclusion criteria for the study were that participants had attended the MPR in 2013 or 2014, had had their 1-year follow-up during 2014 or 2015 (a questionnaire sent by post), and had returned the follow-up questionnaire. Seven women and 5 men were selected randomly and received an invitation letter and information about the study. Eight patients agreed to participate, and 4 declined due to lack of time or energy, family reasons, or emotional distress. The 8 patients who agreed to participate were contacted by the interviewer. Subsequently, 3 participants decided to withdraw their participation: one due to lack of time after obtaining new employment, one had a difficult life situation, and the third did not give an explanation. Another man and 2 more women were contacted and agreed to participate (Fig. 1).
Fig. 1. Flow chart of the participant recruitment process in an interview-study, carried out in 2016 in Sweden, with former multimodal pain rehabilitation (MPR) patients on pain rehabilitation and its impact in their everyday lives.
The participants represented varying sex, age, work status, and pain experience (Table I). Three participants were single, 3 were married, and 2 lived with a partner.
Table I. Study population characteristics in an interview-study, carried out in 2016, in Sweden, with former multimodal pain rehabilitation (MPR) patients on pain rehabilitation and its impact in their everyday lives
Eight semi-structured interviews were conducted in March and April 2016 (23). The interviews were carried out by one researcher (PN), a health communicator and quality improvement facilitator. The first interview was observed by another researcher (AS), also a quality improvement facilitator, with a background as a physiotherapist and psychologist, to enable the researchers to discuss and, if needed, adjust the interview guide. After this first interview and the following discussion, one question was modified and one question was added, as the participant contributed with valuable information about the role of gender for the rehabilitation process. All interviews were conducted in private rooms, at the rehabilitation clinic, another hospital or the interviewee’s workplace. They lasted between 30 min and 1 h 8 min, were tape-recorded and transcribed verbatim by an agency. The open-ended questions focused on the following domains:
An example of the questions included was: “What is your most important experience from MPR?”. The interview guide was based on the literature and pre-tested with a patients’ representative.
During the interviews, the participants were asked if their quality of life had changed with MPR. However, the concept of quality of life was perceived as difficult to relate to. Rather than talking in terms of quality of life, the participants described changes in their everyday life after participation in MPR.
Well, quality of life, I don’t know what to say. Maybe to be able to do things you like. (…) I recently bought a house, fix things at home, a lot of stuff is going on. I kind of like it when there is some action. I couldn’t do such things before. (Tomas)
Qualitative content analysis (24) was performed manually. Two researchers (AS and PN) read the interviews several times to obtain an overall impression. Meaning units were identified, which could be words, sentences, or paragraphs relating to one another through their content and context. Meaning units were condensed according to their core intent and labelled with a code. Two researchers (AS and PN) coded the material individually and compared their results. When needed, the researchers discussed until consensus was reached. A third researcher (MW) then coded a random set of examples (42 quotations), with accordance. The codes were assembled into categories and sub-categories. Finally, an overall theme developed.
The Regional Ethical Review Board in Gothenburg approved this study (Dnr: 784-15). Participation was voluntary, and the participants were informed that they could withdraw their participation at any time without further explanation. All participants signed written informed consent after receiving verbal and written information about the study. To avoid any risk of recognition, the participants are listed numerically in Table I, and given fictitious names when quoted.
An overall theme of “sense of control” emerged. The participants described that MPR increased the sense of control over their pain and their everyday life.
Yes, I can treat it [pain] myself. First of all, I’ve accepted it. I’ve learned to live with it in a, what I feel, good way. (Mary)
They discussed a positive patient–provider relationship and trust in the provider’s expertise as a basis for the rehabilitation process and their acceptance of pain. Pain acceptance and to receive useful tools were, in turn, perceived as a prerequisite to deal with everyday life despite pain. However, social support was not perceived as important to deal with pain in daily life.
Three categories, with 4, 2 and 3 subcategories, emerged during analysis: importance of the patient–provider relationship; knowledge gained; and pain in a social context (Table II).
Table II. Three categories, 9 subcategories and their codes, generated from interviews carried out in 2016, in Sweden, with former multimodal pain rehabilitation (MPR) patients on pain rehabilitation and its impact in their everyday lives
Healthcare experiences prior to pain rehabilitation. When the participants talked about the time prior to MPR, they were most eager to talk about their experiences with primary healthcare and social insurance officials. Both were described as an ongoing struggle. Occasional positive relationships were mentioned as the exception, rather than the rule. Not being taken seriously, to perceive professionals as ignorant and hesitant, and constant changes of staff and administrative routines created a sense of “getting nowhere”’.
It was like “My God, why can’t you stop being this sensitive?” – it was really that mentality [in primary care]. It was no fun taking me in because they didn’t know what to do. They gave me prescriptions – “hopefully that works”, and I was being annoying when I called and said “either I need a higher dosage or a new appointment to try something else”. (Lena)
Meeting the team was expressed as a relief. The team members listened. They gave the participants the time they needed to tell their story and were perceived as understanding and empathic.
They saw my injury. You could say they believed in it, I didn’t have to explain again and again (…). (Sven)
The sense of finally being heard was described as a turning point and emphasized as necessary to start the rehabilitation process. To feel treated as a credible patient also altered the participants’ self-esteem and empowered them to take control of their life.
The participants stressed the pain rehabilitation team’s competence as equally important as their empathy. In contrast to the staff in primary care, the participants trusted the pain rehabilitation team’s expertise.
The participants had less pain compared with their time prior to MPR, but were still affected by pain almost every day. To be able to accept the pain was emphasized as important for everyday life. For both women and men, acceptance meant knowing that there was nothing else to do and that they had received all available treatments. Confidence in the team’s expertise helped the participants to accept the pain.
With such specialists, good at pain, if they can’t help me in any way, maybe you can put the struggle aside to try to find something that works. And maybe that helps, in the long run, to accept it [pain], somehow, even if you don’t really want to. (Eva)
First when they had accepted the pain, they could focus on finding ways to deal with everyday life despite pain.
Well, you must be able to take that step and look forward instead and accept “I have that injury”. I can’t change that, I can’t perform magic, it’s there, and I will have it until the day I die, it is as simple as that. Just try to make the best of it. (Sven)
When the participants were asked whether sex played a role on how they had been treated, all but one woman had a clear answer. The women were convinced that gender norms had led professionals in primary care to dismiss their pain.
You listen more to a man, that’s documented. I guess, you as a scientist know that (laughter). I also believe that many people believe that men don’t say anything until they are really in pain, while women complain. You know, they are in pain but it isn’t that serious. (…) So, if I had been a man, I believe that I would have gotten help earlier, or at least some kind of help at all. Or maybe I wouldn’t have had to get angry to get help. (Anna)
Male participants, on the other hand, felt it was being implicated that men should withstand pain and believed that they would have gained more understanding if they had been women.
Well, men aren’t supposed to whine, they are big and strong, they shouldn’t have problems, they’re not supposed to have pain. And the picture about women is, unfortunately, that they are expected to have pain, to whine, well that’s the general picture in society, unfortunately. (…) Yes, I would have been given more help, maybe, I believe so. (Sven)
Conversely, another man’s assumption was that he would not have been treated differently as a woman. However, he explained it with the accident he had been in.
I had been in such an accident. If it hadn’t been dangerous [injury], if it hadn’t been so bad [injury], I guess, maybe then there would have been more of such a difference. (Tomas)
The participants were convinced that gender norms had a negative effect on their treatment prior to MPR. They also showed awareness about gender norms in society and healthcare. One man even explained that gender norms exist in pain treatment, but only when the pain cannot be explained by obvious injuries. However, the participants exemplified only with their experiences from primary care and did not mention gender bias in MPR.
Control of the body. The participants had experience of physiotherapy in primary care, but stated that they improved their body awareness mainly during MPR. Awareness about their posture made them use the body in a more efficient way, which reduced pain or helped to control pain in everyday activities. Exercises, such as stretching, made sense when explained in a broader context, such as their impact on posture. Exercises were still performed when the participants felt that they needed it.
It has been an enormous help that she [physiotherapist] formed the basis. Since, I have used it [physiotherapy] almost all the time and I know what I should keep in mind… (Lena)
Medication. Participants expressed a cautious attitude towards painkillers, including a fear of dependence. During MPR they learned for the first time how the drugs worked. Knowledge of medication helped the participants to understand and control their drug intake.
I have learned more about how to take pain killers, in a more structured way. It’s very important to feel that you are not afraid of it either, but now I know how I can do. (Eva)
As previous research has pointed to the importance of social support for patients living with pain, we asked the participants about their social network. They described the importance of family and friends generally, but toned down their role when it comes to deal with pain in daily life. Even meeting other patients during MPR was experienced as ambivalent. Generally, MPR did not change the participants’ attitude to social support.
Feeling of isolation and the need to withdraw. Pain was associated with a feeling of social isolation.
I was bedbound, I didn’t socialize with anyone, not with any mates. I was very lonely, because I live on my own, you know. The only people I met, was when I went to the grocery shop. (Lars)
I tried to pretend that it was fun or interesting [to meet others] but it didn’t feel like it. It felt as if I was pretending all the time. It was a hard feeling. (Tomas)
Even though isolation was presented as an unpleasant feeling, the participants described the need to withdraw and to deal with the pain on their own.
I’m rather by myself when I’m most in pain. I think it’s the easiest way, I don’t know what use I may have of other people then. (Anna)
Family and friends. Generally, participants appreciated support from their family.
I had full support. For a while, I couldn’t drive the car and things like that, and then my daughters fixed it [groceries] before they went to work and… when they had time. (Mary)
Conversely, they also noticed the inability to help.
Well, it’s not that they [friends and family] don’t want to, but they don’t know how. They are quite helpless, you know, they come up with some ideas, things you already thought about six years ago, sort of. (Anna)
Even though the participants described relations as an important part of their life, they mainly discussed how they could manage the pain on their own, their unwillingness to ask for help, and the need to protect family and friends from the consequences of their pain.
Not many people have noticed it [my pain]. (…) I was on sick leave, I was ill and I didn’t want to meet anyone. (…) Still, I didn’t show it, I was pretending [being fine]. (Lisa)
I would have gotten more help if I had asked for it. But I don’t like to ask. (…) I don’t know, they are my problems. (…) I don’t want to burden others, I want to take care of myself. (Lars)
Other patients. Even the role of other patients during MPR was portrayed in an ambivalent way. It was a relief to see that others had similar challenges.
Well, it’s nice to see that you’re not alone, that others have the same problems, you get a sense of belonging. As I was misbelieved in the beginning, it was quite nice to meet others like “Damn, there are more than me with problems, maybe it’s not just me being stupid, kind of”. (Lars)
At the same time, the participants were reluctant towards other patients. They expressed it as not being interested in others or being afraid to be affected emotionally by them.
I’m not that kind of person who can talk in front of others about how I’ve been doing. And then I hear a lot of other stories that make me very sad and that makes it worse for me. (Lisa)
MPR was perceived as increasing the participants’ sense of control over their pain and their everyday life, and tools received from MPR were perceived as supporting their independence. Patients’ desire for autonomy and control has been described previously (15, 25–27). It has also been shown that healthcare providers tend to overestimate healthcare interventions when it comes to patients’ experienced quality of life (28). Our study showed that patients did not focus on their symptoms, but rather on their ability to deal with life, despite pain. That confirms also the research of Skuladottir & Halldorsdottir (25) who stated that professionals are seen as powerful and can, through empowerment and true dialogue help patients to regain and maintain a sense of control, which is the main challenge for women with chronic pain (25).
The results of the current study point to some factors that were identified as enabling patients to strengthen their sense of control. A trustful patient–provider relationship was mentioned as a prerequisite for rehabilitation, which also is in line with previous research (12–14, 25, 27, 29). Whereas earlier experience of mistrust was perceived as an obstacle for rehabilitation, the supportive attitude of the pain rehabilitation team was experienced as a great relief and as a new beginning.
A trustful patient–provider relationship was also emphasized as a prerequisite for pain acceptance. Interestingly, the participants’ acceptance of pain was related, not only to the feeling that the provider was supportive, but also competent, and had discussed all adequate treatment options with the patient. The importance of patients’ pain acceptance has been widely discussed (11, 14, 27) and has been described as a complex process, including different components, such as social support, self-care and recognizing limitations (11, 26, 27). Even though earlier research mentioned that patients preferred professionals who were both supportive and professional (12, 29), a focus has been on providers’ empathic qualities (12, 29). Thus, it was surprising that the participants explicitly noted the importance of the provider’s expertise, as a prerequisite to start the process of acceptance.
The patient–provider encounter is influenced by gender (30–32). In addition, gender is a social construct, changeable and constantly negotiated (33). Professionals’ consciousness about gender norms is necessary for equit-able healthcare (21, 32, 34). However, the role of patients’ gender awareness is seldom discussed. The participants not only perceived gender norms as biasing their patient–provider encounter, but also showed awareness about gender norms in society and healthcare. Consequently, patients should be recognized as a part in the construction, re-construction and challenge of gender norms. As the patient–provider relationship consists of mutual interactions, further research on patients’ awareness about and response to gender bias in the patient–provider encounter is highly recommended.
Several studies have stressed the importance of education in pain treatment (11, 16). Two areas of important knowledge gained through MPR were mainly mentioned in our study. Knowledge about medication, how it works, and its short- and long-term effect on pain, as well as knowledge about body, posture, and exercises, were used as tools for making one’s own decisions and to gain control in everyday life. These results, highlighting the importance of participation and of promoting independence in pain rehabilitation, are supported by previous research (12, 35).
The role of social support in pain rehabilitation has been emphasized, especially for women (8, 11, 13). Surprisingly, the participants had an ambivalent attitude towards social support from their family, social network and other patients, and toned down their role when they had to deal with pain in everyday life. Social support is a complex area and there could be different reasons why the participants in our study did not stress the importance of social support, such as their way of life or mental wellbeing. It is also possible that their need for support from healthcare prevailed the need of support from social networks. As the participants emphasized their autonomy, it could also be that they were eager to present themselves as independent of others.
All participants had taken part in MPR and selection bias to MPR have been demonstrated (36, 37). For instance, in a Swedish study, women with 9 years’ compulsory school were less often referred to MPR, compared with women with longer education, despite the same pain level (37). As the use of social support may be greater in lower social class women (38), the selection of participants in this study may have affected their view on social support. However, as the importance of social support, especially for women, has been stressed, the value of social support for different patients, under different circumstances should be explored further.
Eight former patients were interviewed in this study, which constrains the generalizability of the results and their transferability to other settings, as well as the possible diversity of the data collected. In addition to the limited number of participants, they all had been part of MPR. However, the participants represented varying sex, age, work status, material status and pain experience. They discussed similar challenges, such as the importance of pain acceptance, even when asked open and general questions. Saturation was reached when the central theme, categories and sub-categories clearly emerged.
The interview-guide included a question about quality of life, which was perceived as vague by the patients; they preferred to talk about their everyday life instead. It could be perceived as a weakness that we did not persist on asking about quality of life. However, as this qualitative study was aimed to examine participants’ experiences we decided not to hold on to a certain term, but followed the participants’ way of expression. In addition, research has stated that the concept of quality of life is multidimensional and subjective. Other terms, such as functional status and health status, have been used interchangeably, by research and patients (28, 39).
It is a strength of this study that 2 researchers (AS and PN) with different backgrounds, with and without previous experience with the treatment of pain, coded the interviews independently. A third researcher (MW) coded a set of quotes thereafter, with congruence, which strengthens trustworthiness. All 3 researchers worked apart from the pain rehabilitation clinic. The possibility of alternative understandings of the data was discussed with NS (physician in the pain rehabilitation team) and GH (without any connection to the pain rehabilitation team), to reinforce dependability.
To deal with pain in everyday life is a complex field, influenced by subjective experiences and other factors that could not be addressed in this study, such as cultural background and socioeconomics. Although this study can respond to only a limited number of questions, it contributes additional knowledge to the complex field of pain.
The importance of patients’ confidence in the provider’s expertise needs to be considered, as well as patients’ awareness about gender norms. The value of social support in the rehabilitation process was less important compared with previous research and should be explored further in larger samples and different settings.


 Click to show fullsize
Click to show fullsize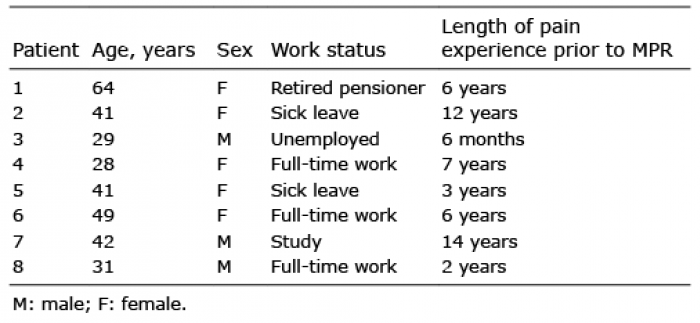 Click to show fullsize
Click to show fullsize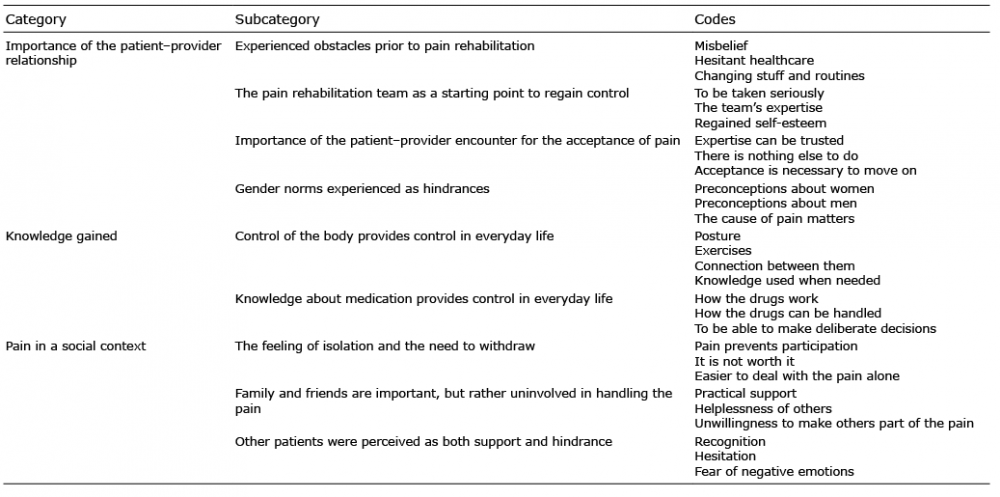 Click to show fullsize
Click to show fullsize