
1Centre de Recherches sur la Cognition Animale, Centre de Biologie Intégrative, Université de Toulouse, CNRS, UPS, Toulouse, France
2Physical Medicine and Rehabilitation Center, MAS Marquiol, Toulouse, France
Objective: Gait rehabilitation is a major concern for adults with an intellectual disability or a neuropsychological disorder. This study evaluated a collective task exercise that could complement an individual rehabilitation routine in such individuals. The movements of 3 individuals (2 patients and 1 healthy individual) were measured while walking alone and in pairs. The recovery rate, amplitude and speed of centre of mass of individuals walking alone were measured and compared with the values of the centre of mass of the system formed by pairs of individuals.
Results: When individuals were walking alone, all parameter values were lower in the 2 patients than in the healthy individual. When the patients were walking in pairs, their recovery rate decreased, but their speed increased when each of them was paired with a healthy individual. In pairs, the recovery rate and the amplitude of the centre of mass remained the same as when walking alone.
Conclusion: Gait rehabilitation does not appear to improve when intellectually disabled patients walk in pairs compared with when they walk alone. However, walking with a healthy individual seems to be more efficient.
Key words: intellectual disability; gait; adults; physiotherapist.
Accepted Sep 27, 2018; Published Dec 20, 2018
JRM-CC 2018; 1: 1000009
Correspondence address: Pierre Moretto, Centre de Recherches sur la Cognition Animale, Centre de Biologie Intégrative, Université de Toulouse, CNRS, UPS, 118 Route de Narbonne, FR-31064 Toulouse, France. E-mail: pierre.moretto@univ-tlse3.fr
A standard method to study locomotion is to analyze the trajectory of the center of mass of walking individuals. In our paper we propose to use this method to evaluate the changes in gait efficiency when such patients are walking alone and when they are walking in pairs linked by a load they transport. We worked with two patients suffering from an intellectual disability. These two patients could be paired either together or with their physiotherapist. Our results show that when the patients were walking in pairs their gait was less efficient than when walking alone. However, when the patients were paired with their physiotherapist, gait efficiency was the same as that as when they were walking alone. We suggest that this collective work could be used as a physical, social and mental exercise they could perform with their physiotherapist and that could be included in their rehabilitation routine.
T
he Maison d’Accueil Spécialisé (MAS) Marquiol rehabilitation centre (Toulouse, France) treats patients with cerebral palsy or brain trauma. A rehabilitation doctor, a physiotherapist and an occupational therapist re-educate patients. The rehabilitation of gait and motor abilities is an essential part of the treatment, and the patient’s walking ability thus needs to be assessed regularly. The main objective of this study was to propose a relevant exercise for this assessment. Based on a protocol used to investigate the collaboration between 2 healthy individuals (1), an exercise was conceived that aimed to enable 2 patients with intellectual disability to work together.
The centre of mass (CoM) was measured during a complete walking cycle at constant speed, first of 2 patients walking alone, then of 2 of the same patients walking in pairs together, or with a healthy subject, while linked by an object they were carrying. It was investigated whether, when walking alone, the patients walk in the same way as healthy individuals and whether, when walking in pairs, they are able to collaborate to move as efficiently as they can alone.
In a previous study (1) we showed that the gait of the system formed by a pair of healthy individuals walking together while transporting a box was as economical as that of healthy individuals walking alone. The current study tested the hypothesis that this is also true for pairs of patients with an intellectual disability. In addition, we tested whether a pair of such patients is as economical as a pair comprising one such patient and a healthy individual.
Three individuals participated in this study; 2 patients and 1 healthy individual. The first patient (P1) had cerebral palsy (male, height 1.71 m, weight 59.2 kg, age 25 years), and wears a foot orthosis in his daily living due to an orthopaedic deformation (varus of the ankle). He has been evaluated as level 1 in the Gross Motor-Function Classification System (GMFCS). The second patient (P2) has brain trauma (male, height 1.65 m, weight 64.2 kg, age 45 years). Both patients have few motor dysfunctions with no joint limitations, but their clinical gait pattern is not qualitative (i.e. they show unusual movements of the body segments and a decrease in walking speed). They do not report any pain in their everyday life. The occupational therapist also categorized the level of autonomy of the 2 patients according to the Functional Autonomy Measurement System (SMAF, 2). P1 has a disability score of –32.5, a handicap score of 0, and a 3rd category Iso-SMAF profile of 10 (predominant alterations in cognitive functions). P2 has a disability score of –35, a handicap score of 0, and a 3rd category Iso-SMAF profile of 8 (predominant alterations in cognitive function). Because of their need for assistance in daily living, both patients live permanently in the rehabilitation centre. They are able to understand simple orders and can walk without help. The healthy individual in our study (control) was the patients’ physiotherapist (male, height 1.78 m, weight 67.1 kg, age 25 years). The patients and the physiotherapist signed consent forms.
P1 and P2 are friends and have undergone weekly rehabilitation sessions with their physiotherapist during the previous 2 years.
The experimental protocol was non-invasive and corresponded to the level of daily activity practiced by the patients, i.e. it was in agreement with the definition of a non-interventional study of the CNRS bioethical office. The patients performed 1 trial alone and 2 trials in which they had to walk side-by-side while carrying a box (mass 13.41 kg) with 2 lateral handles, first with the other patient (P1/P2), then with the physiotherapist (P1/C and P2/C). During the experiment the individuals walked at a spontaneous, stable speed along a 13-m walkway; communication was not allowed.
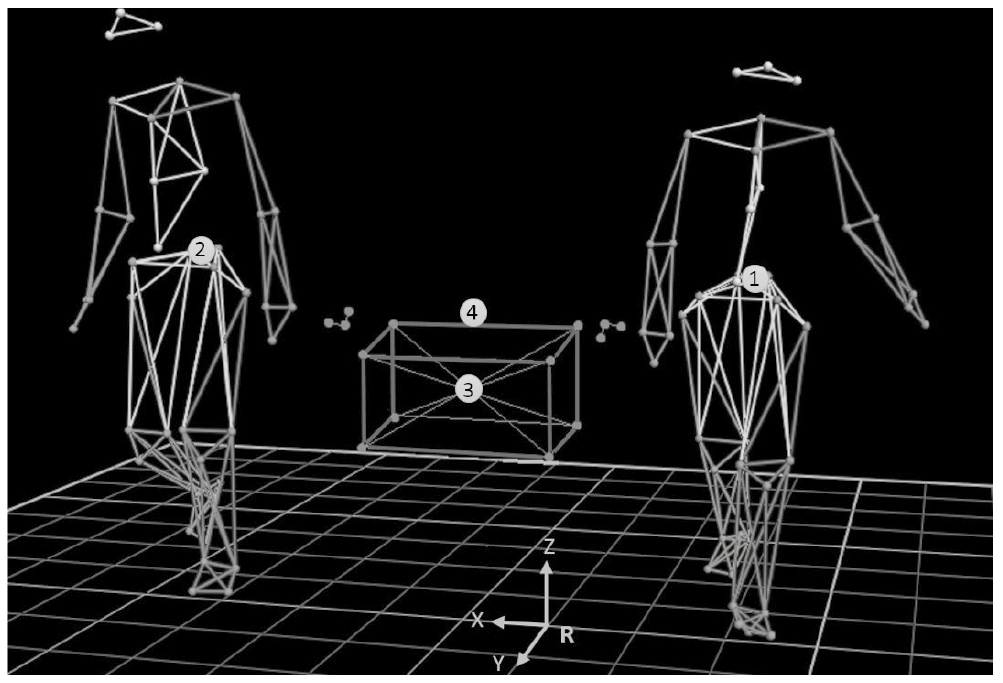
Thirteen infrared (11 MX3 and 2 TS40) transmitter-receiver video cameras (Vicon©, Oxford) were used to acquire the kinematic data. The gait cycle of an individual walking alone was recorded from his first to his third heel strike. The gait cycle of paired individuals was recorded from the first heel strike of individual 1 to the third heel strike of individual 2 (Fig. 1). Forty-two retro-reflective markers were placed on each individual, according to Wu et al. (3, 4), and their positions were recorded at a frequency of 200 Hz (filtered by a 4th order Butterworth filter and a 5-Hz cut frequency). Fourteen markers were placed on the box. The estimated error for the localization of the markers in the Galilean reference frame R was 1 mm. To allow kinematic analyses, the individuals and the box were reconstructed using Vicon NexusTM 1.8.5 software (Oxford Metrics).
The patients had time to become familiarized with the research room and the equipment before the experiment (i.e. they wore false markers taped on their body during the whole week preceding the exercise).
Fig. 1. Reconstruction of the patients and the load they carry on Vicon NexusTM. The points correspond to the locations of the markers. The circles represent the centre of mass (CoM) of individual 1 (1), individual 2 (2), the box (3) and the Poly-Articulated Collective System (PACS) (4). The patient’s side was randomly determined when they were paired together: Patient 1 (P1) was located at individual 1 location and Patient 2 (P2) at individual 2 location. When the physiotherapist was paired with a patient, the patient remained in his previous location. The R referential was drawn with x as the medio-lateral axis, y the antero-posterior axis, and z the vertical axis.
De Leva anthropometric tables (5) were used to estimate the mass (mi) and the CoM of each body segment and to compute the position of the global CoM of the individuals (6) walking alone and of the system formed by the pairs of individuals and the box they carried.
Following Cavagna et al. (7), the recovery rate (RR) of the CoM of the individuals and of the pairs in the sagittal plane was computed to obtain an indication of the percentage of transfer between potential and kinetic energy. These energies depend on the CoM location in the referential used (7–9). The closer the value of RR to 100%, the higher the amount of transfer between potential and kinetic energy and the more economical the gait. The amplitude (A= Zmax-Zmin, where Z is the height of the CoM in m) and the speed (m.s–1) of the CoM were also assessed. Fumery et al. (1) have shown that the RR of a pair of individuals performing a collective transport task is comparable to the RR of single individuals. We thus compared the RR of single individuals with that of the pairs they formed when walking together.
All data were analysed with Matlab R2016b©.
The pairs of each patient with the healthy individual (C) were: P1/C and P2/C. P1 had cerebral palsy and P2 brain trauma. The control individual was the patients’ physiotherapist.
When the patients were walking alone their RR was 5.68% and 3.5% lower (Fig. 2A), the amplitude of their CoM 16.89% and 8.67% lower (Fig. 2B), and the speed of their CoM (Fig. 2C) 42.55% and 47.48% lower than the control individual, for P1 and P2 respectively.
When the patients were walking together, the RR of the pair was 6.20% and 8.30% lower compared with when they were walking alone, for P1 and P2, respectively.
When the patients were paired with the control individual, the RR of the pair increased by 6.07% and 6.52%, and the amplitude of the CoM of the pair by 61.74% and 71.30% (Fig. 2E) compared with the situation where they were paired together, for P1 and P2, respectively.
Fig. 2. Recovery rate (A, D), amplitude (B, E) and speed (C, F) of the centre of mass (CoM) of the 2 patients (P1 and P2) and of the healthy individual (Control=C) walking alone (A, B, C) and of the CoM of the sytem formed by the box and the pair (D, E, F) of 2 patients (P1/P2).
It was anticipated that the proposed exercise would be entertaining for patients with an intellectual disability. This was indeed the case; the patients enjoyed achieving the task, which constituted a welcome change to their rehabilitation routine. Our main result shows that the CoM of the system formed by a pair patients with intellectual disability has a less pendulum-like behaviour than the CoM of the pairs of the same patients with a healthy individual.
When P1 and P2 were walking alone, they walked nearly half the speed of the control individual, who walked at the standard natural speed reported in the literature (i.e. 1.1–1.4 m.s–1) (9). When P1 and P2 were walking together, their spontaneous speed increased slightly (≈+0.11 and + 0.18 m.s–1 for P1 and P2, respectively). When P1 or P2 were paired with the control individual they walked at approximately the same speed as when they were paired together. Therefore, the control individual had to greatly decrease his walking speed, whereas the patients slightly increased their speed. Thus, walking with another patient or with a healthy individual does seem to have a positive effect on the patients’ walking speed.
Secondly, when P1 and P2 were walking alone, the amplitude of their CoM displacement was close to 4 cm. Holt et al. (10) reported a similar value (i.e. 3.9 cm) for healthy individuals walking at 1.4 m.s–1. However, at the imposed speed of 0.8 m.s–1, corresponding to the speed of our patients walking alone, these authors found an amplitude of 2.6 cm, lower than the value we found. This discrepancy could be due to the fact that, in Holt et al.’s study, the individuals did not walk at a spontaneous speed, and thus had to adapt their gait. When P1 and P2 were walking together, the amplitude of the CoM of their pair was lower than that when they were walking with the control. Therefore, walking together with another patient seems to have a negative effect on the locomotor pattern of the patients. This could be due to a lack of coordination between patients when they walked together.
Finally, when P1, P2 and the control were walking alone, their RR was comparable with that reported by Bastien et al. (9) for unloaded and untrained individuals (RR = 61%). The values of RR for P1 and P2 were similar, but were lower than that of the control. Thus, when walking alone the healthy individual had a more pendulum-like behaviour than the patients, which means that his locomotion was more economical. When P1 and P2 were walking together, the RR of their pair decreased substantially compared with when they were walking alone. When P1 or P2 were walking with the control, the RR of their pair remained at the same level as when they were walking alone. These values are comparable with those reported by Fumery et al. (1) (i.e. RR ± CI0.95 = 60.25 ± 7.59%). This shows that walking together had a lower positive effect on the gait of the pair formed by the patients than on that formed by a patient and a healthy individual.
In conclusion, the rehabilitation exercise had a more positive effect on gait rehabilitation of our patients when each of them walked with a healthy individual than when they walked together. There were few differences between the results of P1 and P2, which highlights the fact that the type of pathology does not seem to affect the way the patients interact with a healthy individual in the proposed exercise. It might be interesting to perform the same type of analysis after a collective rehabilitation sessions during a few weeks in order to investigate whether the rehabilitation exercise is more efficient than the standard rehabilitation protocol used on single individuals in rehabilitation centres.
Financial support was provided by ANRT (CIFRE 2015/1321) and MAS Marquiol for G.F’s PhD. The authors wish to thank Soïzic Benezech (the occupational therapist) for his expertise in this research.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize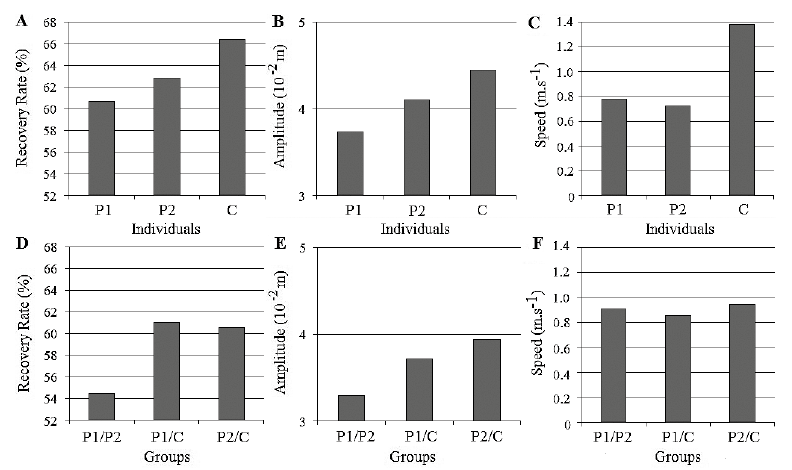 Click to show fullsize
Click to show fullsize