
From the 1School of Kinesiology, University of British Columbia, 2International Collaboration on Repair Discoveries (ICORD), Vancouver Coastal Health Research Institute, Vancouver, BC, Canada, 3Department of Urology, University Hospital Basel, University of Basel, Basel, Switzerland and 4Department of Urological Sciences, Faculty of Medicine, University of British Columbia, Vancouver, BC, Canada
Objective: The primary aim of this study was to determine the feasibility of delivering an exoskeleton-assisted walking intervention targeting lower urinary tract function in people with motor-complete spinal cord injury. Secondary aims were to determine if exoskeleton walking activates the pelvic floor muscles, and compare 2 exoskeleton programmes regarding lower urinary tract function.
Design: Randomized pilot trial.
Subjects: Adults with motor-complete spinal cord injury at or above T10.
Methods: Participants were randomized to receive Ekso or Lokomat training. Feasibility outcomes included recruitment rate, adherence, and adverse events. Pelvic floor muscle electromyography was recorded during walking. Urodynamic studies, 3-day bladder diary, and Qualiveen-30 were administered pre- and post-training.
Results: Twelve people were screened and 6 people enrolled in the study. Two subjects withdrew from unrelated reasons. There was one adverse event. Pelvic floor muscle activity was greater in the Ekso group. Lower urinary tract function did not clearly change in either group.
Conclusion: This pilot study demonstrates the feasibility of delivering an exoskeleton training programme targeting lower urinary tract function. Ekso-walking elicits pelvic floor muscle activity, but it remains unclear how locomotor training impacts lower urinary tract function.
Key words: spinal cord injury; exoskeleton device; pelvic floor; electromyography; lower urinary tract symptoms.
Accepted Jul 21, 2021; Epub ahead of print Aug 12, 2021
J Rebabil Med 2021; 53: jrm00222
Correspondence address: Tania Lam, School of Kinesiology, University of British Columbia, International Collaboration on Repair Discoveries (ICORD), 818 West 10th Avenue, Vancouver BC, Canada. E-mail: tania.lam@ubc.ca
Doi: 10.2340/16501977-2864
Some studies in people with spinal cord injury have reported improvements in urinary bladder health after gait therapy, but the mechanisms behind this are unclear. Strong pelvic floor muscles are crucial to urinary bladder health, and these muscles are normally active during walking. It is possible that the pelvic floor muscles are similarly engaged during exoskeleton-walking in people with spinal cord injury, and this could improve urinary bladder health. This study demonstrates that delivering an exoskeleton intervention to people with spinal cord injury for urinary bladder health is feasible. Participants were successfully recruited to a training programme, and any dropouts were because of issues unrelated to the study. Furthermore, the study showed that the pelvic floor muscles are active while walking in 1 type of exoskeleton, but it remains unclear how exoskeleton-walking may help improve urinary bladder outcomes. Further research is needed to explore how exoskeleton interventions may engage the pelvic floor muscles and improve urinary bladder health outcomes for those with spinal cord injury.
Neurogenic lower urinary tract dysfunction (NLUTD) impacts nearly 80% of the spinal cord injury (SCI) population and has far-reaching implications for physical and psychosocial health. The consequences of chronic NLUTD are a leading cause of rehospitalization post-injury (1), and recovery of lower urinary tract (LUT) function is a top priority for the SCI community (2).
While rarely prescribed to people with SCI, physical therapy approaches targeting the pelvic floor muscles (PFM) are the first-line treatment for urinary incontinence (UI) in the able-bodied population. This approach focuses on strengthening the PFM to better assist the external urethral sphincter in closing the urethra for maintaining urinary continence (3). There is also evidence that PFM contractions can reflexively relax the detrusor muscle, effectively reducing detrusor overactivity and increasing bladder capacity (3, 4). This mechanism is of particular interest for people with SCI, who often experience neurogenic detrusor overactivity.
The PFM are also active during gait, possibly as part of a control strategy to regulate intra-abdominal pressure, in coordination with other muscles of the trunk (5). In people with SCI, gait interventions may improve LUT function, but the mechanisms are unclear (6). The degree of trunk muscle engagement in people with SCI varies with the type of gait training device used. During Ekso-assisted walking, which is overground and requires weight-shifting to trigger steps, we have observed activation of muscles in the trunk even in people with motor-complete SCI (mcSCI) (7). In contrast, during Lokomat-assisted walking, which is treadmill-based, no trunk muscle activation is observed (7).
Considering that the PFM co-activate with trunk muscles and are active during gait, and taking into account recent evidence of spared innervation to the PFM in people with mcSCI (8), it is plausible that these muscles would be similarly activated during Ekso walking. However, it is yet to be determined if Ekso walking is a viable approach to improve LUT function through training the PFM. The purpose of this pilot study was to determine the feasibility of an Ekso vs. Lokomat-assisted walking programme on LUT function in people with mcSCI. Our secondary aims were to determine if the PFM are active during exoskeleton walking, and compare the possible effects of 2 exoskeleton training programmes on LUT function.
Participants
Participants had to be between 19 and 65 years of age; at least 6-months post-injury; and have a mcSCI (i.e. American Spinal Injury Association Impairment Scale (AIS) A or B) at or above the T10 neurological level, as verified by the International Standards for Neurological Classification of SCI examination, which was performed post-enrolment. Participants had to meet the Ekso and Lokomat manufacturer requirements and present with NLUTD. Individuals were excluded if they had a cognitive impairment or additional neurological impairment beyond SCI. All procedures were approved by the University of British Columbia’s Clinical Research Ethics Board, and all participants provided informed written consent.
Since this was a pilot study, a sample size calculation was not performed (9). However, the study aimed to recruit 10 participants, which was considered a large enough sample to determine the practicalities of delivering a similar intervention as a full-scale randomized control trial.
Procedures
This study employed a parallel-group randomized design, in which participants were randomized using a computer-generated sequence with allocation concealment to receive either a Lokomat or Ekso walking programme. Group allocation was revealed after completion of baseline assessments.
The training intervention included 36 sessions of exoskeleton training (45 min walking/session), scheduled thrice weekly, over 12 weeks. A session rating of perceived exertion (RPE) score was calculated by taking the mean of RPE values reported by the participant every 10 min. Total distanced walked and mean speed in the Lokomat, as well as total steps taken and speed as determined by the 10-Meter Walk Test in the Ekso, were recorded.
Feasibility outcomes
Recruitment was examined by recording the number of participants approached, screened for eligibility, and randomly assigned, as well as the reasons for exclusions. Adherence was determined by the number of participants who participated in the intervention, their attendance to scheduled sessions with reasons for drop-outs and missed sessions, and the time taken to complete the intervention. Adverse events to the intervention or outcomes measures were recorded. Feasibility of the training intervention was measured by changes in RPE, speed, steps (Ekso), and distance (Lokomat).
Pelvic floor muscle recruitment
To evaluate the activation pattern of the PFM in the different devices, electromyography (EMG) recordings were taken from each participant while they walked at a comfortable, self-selected pace in their assigned exoskeleton during a post-training session. Bilateral surface electrodes were placed perianally (Trigno, Delsys Inc., Natick, Massachusetts, USA) and data were recorded at 2,000 Hz.
Lower urinary tract function
LUT function was assessed using urodynamic studies (UDS), a 3-day bladder diary, and the Qualiveen-30 questionnaire. UDS were performed in accordance with the International Continence Society Good Urodynamic Practices guidelines by a blinded assessor and UDS reports were reviewed by a blinded urologist (10). For the 3-day bladder diary (11), participants were instructed to record their 24-h fluid intake (ml), 24-h catheterized urine volume (ml), and any episodes of UI per 24-h.
To assess the impact of NLUTD on quality of life (QoL), participants completed the Qualiveen-30 questionnaire (12). This questionnaire includes 30 questions on a 0–4 scale in 4 categories: Bother with Limitations, Frequency of Limitations, Fears, and Feelings.
Data analysis
Mean speed, steps, distance, and session RPE were taken for each participant during the first and last 5 sessions to assess improvement in exoskeleton use over time.
All EMG data were band-stop filtered at 60 Hz and then high-pass filtered at 30 Hz with an 8-order dual-pass Butterworth filter and rectified.
Five outcomes were extracted from the UDS data: bladder compliance (ml/cmH2O), maximum storage detrusor pressure (cmH2O), cystometric capacity (ml), presence of neurogenic detrusor overactivity (NDO), and volume at first involuntary detrusor contraction (ml).
Six outcomes were extracted from the 3-day bladder diaries: number of UI episodes, mean catheterized urine volume (ml), maximum catheterized urine volume (ml), number of bladder-emptying events via catheterization, fluid intake and (ml) catheterized urine volume (ml) per 24-h. For each outcome, the mean over the 3 days was calculated.
The Qualiveen-30 results were calculated as per the scoring guidelines. Total and subdomain scores range from 0 to 4, with lower scores representing better QoL.
Descriptive statistics were applied (Microsoft Excel 2016, Redmond, Washington, USA). Raw data were plotted or placed in a table for visual inspection.
Feasibility
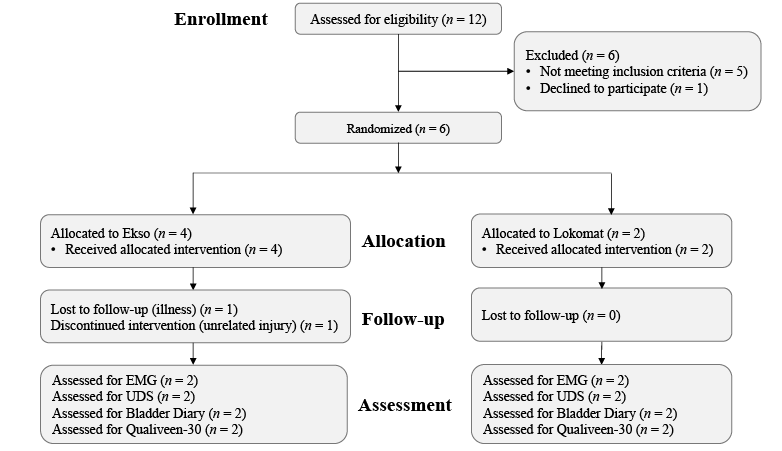
Fig. 1 shows the CONSORT flow diagram of participant recruitment and retention. Twelve individuals were screened for eligibility. Five individuals did not meet the study criteria and one eligible person decided against participating due to scheduling commitments. The other 6 individuals were enrolled and began the intervention (n = 4 Ekso, n = 2 Lokomat). One Ekso participant withdrew after 5 sessions due to an injury from a motorcycle accident, and 1 Ekso participant finished the intervention, but was unable to complete the post-training assessments due to unrelated illness. Demographics and injury characteristics of the 5 participants who completed the study are shown in Table I.
Fig. 1. Consolidated Standards of Reporting Trials (CONSORT) flow diagram for pilot and feasibility trials. EMG: electromyography; UDS: urodynamic studies.
Table I. Participant demographics
All 5 participants completed 36 sessions of exoskeleton training. Training time ranged from 92 to 154 days (Table II). All participants rescheduled at least one appointment due to unrelated illness or scheduling conflict, and there were some delays in training due to extraneous factors, such as transportation or unexpected work commitments.
Table II. Training outcomes
The majority of training sessions included 45 min of walking, but some sessions had to be stopped early for various reasons, including neuropathic pain (LK01 once), lower limb spasticity (EK01 once, EK02 twice), symptomatic autonomic dysreflexia (EK01 once), or bowel incontinence (EK02 once).
All participants improved their walking speed and steps/distance from pre- to post-assessment (Table II). There was minimal or no change in RPE from early to late training for all participants, with the exception of EK01 (Table II).
Only one adverse event (grade 1, i.e. mild) was recorded during this study. LK01 developed minor skin abrasions over the anterior surface of his tibias, where the Lokomat’s leg cuffs were in contact. The participant was given time off training to allow for healing. When training resumed, extra padding and additional body-weight support was provided.
Pelvic floor muscle recruitment
Bilateral activity was observed in the PFM EMG in both EK02 and EK03 during Ekso walking trials (Fig. 2). The activity appeared rhythmic in EK02, while there was no clear activation pattern in EK03. Little, if any, PFM EMG activity was observed in LK01 and LK02 as they walked in the Lokomat; LK01 showed possible PFM activity on the right side, but this activity was of a much smaller amplitude compared with those in the Ekso group.
Fig. 2. Pelvic floor muscle electromyography (PFM EMG) recordings during quiet supine (rest) and walking in either the Ekso or Lokomat. The speed at which each participant walked is reported under their ID. The top trace (light grey) represents the right muscle, while the bottom trace (dark grey) represents the left muscle. The envelope of each signal is overlaid on each plot as a black trace. The grey vertical lines during the walking condition represent right heel strikes.
Lower urinary tract outcomes
The results from the UDS, 3-day bladder diary, and Qualiveen-30 questionnaire are shown in Table III. Changes in UDS outcomes were minor and variable across participants.
For the 3-day bladder diary, EK02 used a condom catheter to void, limiting the parameters that could be extracted from this participant. UI episodes improved for both participants in the Lokomat group; neither participant in the Ekso group experienced UI at the pre- or post-assessment.
For the Qualiveen-30 questionnaire, EK02 showed an improvement (overall score reduced by more than half), while LK02 had a more substantial worsening of LUT-associated QoL (overall score doubled). Only minor changes in scores were reported by EK03 and LK01. Changes in subdomain scores were variable across participants.
Table III. Lower urinary tract function and quality of life outcomes
This pilot study demonstrates the feasibility of delivering an exoskeleton training programme to people with mcSCI to assess changes in LUT function. While we saw reasonable participant recruitment and adherence, with only one adverse event, it remains unclear how LUT function may be impacted by this type of training.
Exoskeleton training is a feasible intervention
Recruiting individuals with SCI to clinical trials is challenging; however, exoskeletons are generally viewed positively for rehabilitation and health benefits (13), and the opportunity to use an exoskeleton may incentivize participation. The current study aimed to recruit 10 participants, and screened 12 individuals, but only half were eligible and enrolled in the study. Of the 6 participants who started the intervention, 2 withdrew from the study. Reasons for dropout were not due to the demands of the study or adverse events, suggesting that the study protocol was well tolerated. However, participants took between 8 and 70 days longer to complete the intervention than intended. Traditional PFM training protocols are often more concentrated, as participants may perform exercises daily and over a shorter period of time (3); it is unclear how the protracted duration of the protocol in this study might have impacted LUT outcomes.
Ekso walking elicits more pelvic floor muscles activity than Lokomat walking
More PFM activity was observed in participants who walked in the Ekso than those who walked in the Lokomat. It is possible that trunk muscle activation evoked by the Ekso (7) is sufficient to co-activate the PFM during walking. In comparison, reduced trunk engagement observed during Lokomat walking could minimize any co-activity of the PFM.
Previous work in able-bodied participants has demonstrated that PFM activity increases with gait speed (5). While walking speed was not matched across participants, the speed of the 2 Lokomat participants was within the range of the Ekso participants. As such, variance in speed between the 2 devices is unlikely to account for the increased PFM activity seen in the Ekso users.
Does exoskeleton training impact lower urinary tract function?
Considering the relatively small sample size, the results of the current study did not yield a clear pattern in UDS findings between groups. While UDS is considered the gold standard for assessing LUT function, previous studies have demonstrated poor repeatability of UDS outcomes in people with SCI (14). Clinically significant changes in UDS outcomes have also yet to be established, but the current findings seem to fall largely within the range of normal variability, suggesting that the changes observed in the current study post-intervention are likely not significant (15).
Similar to the UDS findings, the 3-day bladder diary results did not provide a clear picture. Importantly, UI was reduced or eliminated in both Lokomat users post-training. However, neither Ekso participant experienced UI initially, so we are unable to make effective comparisons between the 2 groups.
The Qualiveen-30 results were also variable; while 1 Ekso user substantially improved and 1 Lokomat user substantially worsened, the other 2 participants had only minimal change. The substantial improvement in the Ekso user is encouraging, but additional work is needed to explore these findings.
Methodological considerations
As we did not stratify by the severity of NLUTD symptoms at intake, there was an imbalance where no participant in the Ekso group experienced UI at the pre-assessment, which made for ineffective comparisons. Future studies may consider stratifying participants by symptoms at intake.
EMG recordings were only taken while each participant was in their assigned exoskeleton. It remains unclear from this small sample size if the PFM activity observed in the current study was due to the effect of the device itself or individual variation.
Despite these potential limitations, this pilot study demonstrates the feasibility of delivering an exoskeleton training intervention on LUT function to people with mcSCI. These findings suggest that the Ekso can elicit PFM activity from mcSCI, but it remains unclear how this intervention may impact LUT function and LUT-related QoL.
The authors thank all of the participants involved in this study for their time and efforts, and the staff at the Brenda and David McLean Integrated Spine Clinic for their assistance with the UDS procedures, especially Ivy Allard, Teresa Lim, and Tammy Wilder for conducting these examinations. Finally, the authors thank all of the individuals who assisted with the exoskeleton training and/or data collection over the course of this trial, including Amanda Chisholm, Gevorg Eginyan, Andrea Lynn, Maya Sato-Klemm, Mason Chow, Riley Louie, and Catherine Chan.
Funding. This work was supported by the Blusson Integrated Cures Partnership and the Canadian Institutes of Health Research (PJT-166040). These funders provided financial support for the conduct of this research, but played no role in study design, collection, analysis, interpretation of data, preparing the report, or submitting this article for publication.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize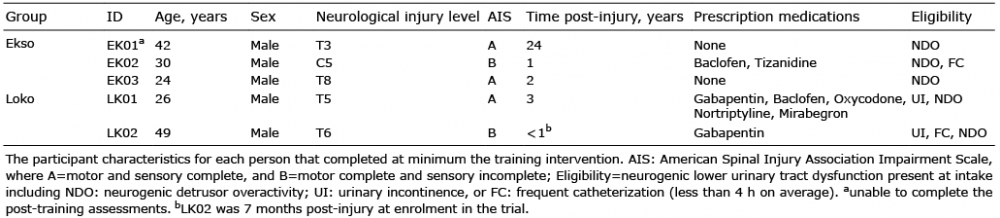 Click to show fullsize
Click to show fullsize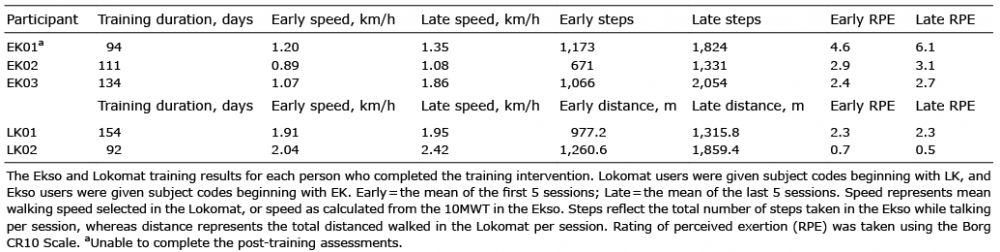 Click to show fullsize
Click to show fullsize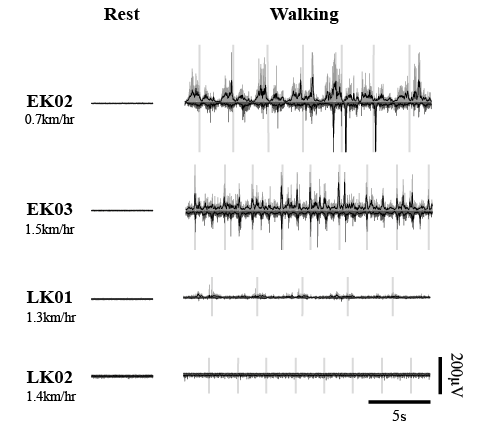 Click to show fullsize
Click to show fullsize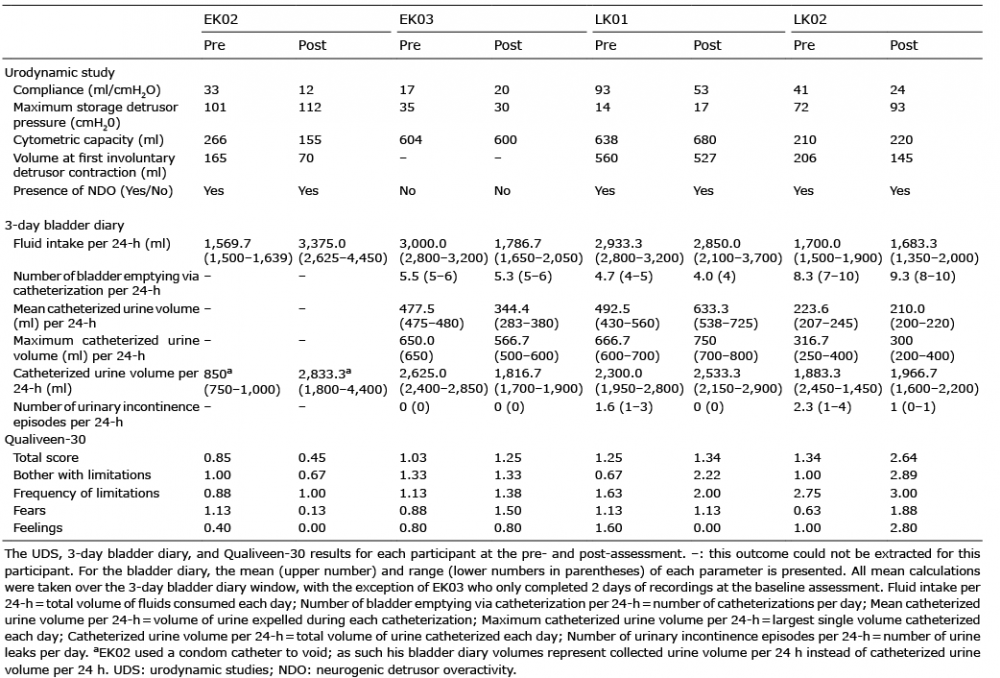 Click to show fullsize
Click to show fullsize