
From the 1Department of Neurology, Elisabeth-Tweesteden Hospital, Tilburg, 2Department of Psychiatry and Neuropsychology, School for Mental Health and Neuroscience; and Department of Neuropsychology and Psychopharmacology, Faculty of Psychology and Neuroscience, Maastricht University, Maastricht, 3Limburg Brain Injury Center, Maastricht University and Maastricht University Medical Center, 4Department of Rehabilitation, Physical Therapy Science and Sports, UMC Utrecht Brain Center, University Medical Center 5Center of Excellence for Rehabilitation Medicine, UMC Utrecht Brain Center, University Medical Center Utrecht, and De Hoogstraat Rehabilitation, Utrecht and 6Department of Rehabilitation Medicine, University of Groningen, University Medical Center Groningen, The Netherlands
Objective: To examine the temporal evolution of subjective cognitive complaints in the long-term after stroke, and to identify predictors of long-term subjective cognitive complaints.
Methods: Prospective cohort study including 395 stroke patients. Subjective cognitive complaints were assessed at 2 months, 6 months and 4 years post-stroke, using the Checklist for Cognitive and Emotional consequences following stroke (CLCE-24). The temporal evolution of subjective cognitive complaints was described using multilevel growth modelling. Associations between CLCE-24 cognition score at 4 years post-stroke and baseline characteristics, depression, anxiety, cognitive test performance, and adaptive and maladaptive psychological factors were examined. Significant predictors were entered in a multivariate multilevel model. Results: A significant increase in subjective cognitive complaints from 2 months up to 4 years (mean 3.7 years, standard deviation (SD) 0.6 years) post-stroke was observed (p≤0.001). Two months post-stroke, 76% of patients reported at least one cognitive complaint, 72% at 6 months, and 89% at 4 years post-stroke. A higher level of subjective cognitive complaints at 2 months and lower scores on adaptive and maladaptive psychological factors were significant independent predictors of a higher level of subjective cognitive complaints at 4 years post-stroke.
Conclusion: Post-stroke subjective cognitive complaints increase over time and can be predicted by the extent of subjective cognitive complaints and the presence of adaptive and maladaptive psychological factors in the early phases after stroke.
Key words: stroke; rehabilitation; cognition; cognitive complaints.
Accepted Apr 20, 2021; Epub ahead of print May 5, 2021
J Rehabil Med 2021; 53: jrm00205
Correspondence address: Caroline M. van Heugten, Maastricht University, PO Box 616, 6200MD Maastricht, The Netherlands. E-mail: c.vanheugten@maastrichtuniversity.nl
Doi: 10.2340/16501977-2840
Many people suffer a stroke in the brain leading to consequences in different areas of functioning. Complaints in the domain of thinking (memory, attention, planning and organization) are frequent post-stroke. This study investigated the occurrence and type of complaints experienced in the first years after a stroke. The study found that these complaints increase over time. Long-term complaints are found in those people who already have problems early after stroke.
Subjective cognitive complaints (SCC) are common after stroke, with prevalence rates varying between 28.6% (1) and 90.2%, (2), depending on stroke characteristics, time since stroke, SCC definitions and the instruments used. The most commonly reported complaints are mental slowness (in 46–80% of patients) and difficulties in concentration and memory (in 38–68% and 38–94% of patients, respectively) (3). Previous cross-sectional studies showed that SCC are present in both the early stages after stroke (1–6 months after stroke) (4–6), and in the long-term (> 1 year after stroke) (1, 7, 8). To date only a few studies have examined the temporal evolution of SCC. Tinson & Lincoln observed an increase in SCC between 1 and 7 months post-stroke (n = 95) (9). The authors used the Everyday Memory Questionnaire (10), focusing on memory-related complaints. Wilz & Barskova also found an increase in SCC over time after stroke (3 vs 15 months post-stroke, n = 81) (11). SCC were measured with the Patient Competency Rating Scale cognition subscale (12). Van Rijsbergen et al., who used the Checklist for Cognitive and Emotional consequences following stroke (CLCE-24) (13), recently found that SCC remained stable between 3 and 12 months after stroke (n = 155) (14). Long-term results on the course of post-stroke SCC are lacking. Since SCC were found to be independently related to lower quality of life in patients with mild cognitive impairment (15), and patients with subarachnoid haemorrhage (16), it is important to assess SCC after stroke. Furthermore, earlier research showed that SCC were most strongly associated with participation after stroke, compared with cognitive tests in a neuropsychological test battery, and the Montreal Cognitive Assessment (MoCA) (17, 18). Hence, in order to improve participation and integration in society after stroke, it is important to take the patients’ perspective into account, rather than only determining objective cognitive measures.
The presence and severity of SCC is expected to be a direct reflection of the presence and severity of cognitive deficits. However, previous studies investigating the relationship between SCC and cognitive performance in stroke patients have shown conflicting results (1–4, 7, 8, 13, 19, 20). Other factors have shown to be related to SCC, in particular psychological factors, such as depressive symptoms (2, 4, 6, 7, 21), anxiety (21, 22), perceived stress (14), personality traits (7, 22), and coping style (23). To date, only one study on SCC used a longitudinal design (14), which prevents conclusions on the temporal evolution of SCC in stroke patients in the long term. Since more stroke patients survive, recover well and are discharged home nowadays, it is important to address predictors of SCC in the early phases after stroke, in order to identify patients who need more intensive monitoring at follow-up. Once identified, it is possible to investigate whether the patients will benefit from more focused rehabilitation programmes.
The aim of this longitudinal study was to examine the temporal evolution of SCC, from 2 months until 4 years post-stroke. Furthermore, the study assessed which factors are predictive of SCC at 4 years post-stroke, taking into account demographic and stroke-related characteristics at baseline, and cognitive deficits and psychological factors measured at 2 months post-stroke.
Design and procedure
The current study is an extension of the Restore4Stroke cohort study, a multicentre longitudinal prospective cohort study investigating the course and determinants of quality of life and participation after stroke, in which stroke patients were initially followed for 2 years (24). Patients were recruited from stroke units in 6 participating general hospitals in the Netherlands between March 2011 and March 2013. With the extension of the study, extra measurements were conducted at 4 years after stroke (mean 3.7 years after stroke). The collection of these data took place between June 2015 and November 2016. The current study reports data from stroke onset (T1), 2 months (T2), 6 months (T3), and 4 years post-stroke (T4). The baseline assessment (T1) consisted of demographic and stroke-related factors, assessed by a trial nurse 4 days post-stroke at the hospital. At T2, T3 and T4, trained research assistants conducted assessments of cognitive complaints. At T2, depression, anxiety and psychological factors were assessed using questionnaires, and cognitive performance was assessed by research assistants. The research assistants were all trained by the same investigator to ensure inter-observer agreement. Assessments either took place in the nearest participating hospital or at home (if patients were not able to travel). The Restore4Stroke cohort study was approved by the medical ethics committees of all participating hospitals (Medical research Ethics Committees United number NL34676.100.10) and informed consent was obtained from all patients.
Subjects
Patients were eligible if they had a clinically confirmed diagnosis of stroke (ischaemic or haemorrhagic, judged from computed tomography (CT) scan in the acute phase) and had had a stroke in the preceding 7 days. All patients had to be at least 18 years old. Patients were excluded if they: (i) had a serious other condition whereby an interference with the study outcomes was expected (e.g. neuromuscular disease); (ii) were already dependent regarding activities of daily living (ADL) before their stroke, as defined by a Barthel Index (BI) score ≤ 17; (iii) had insufficient command of the Dutch language to understand and complete the questionnaires; or (iv) were already experiencing cognitive decline, as defined by a score of one or higher on the Heteroanamnesis List Cognition (25) before their stroke.
Measures
The presence of SCC was assessed using the cognitive complaints scale of the Checklist for Cognitive and Emotional consequences following stroke (CLCE-24), which consists of 13 items (e.g. problems with “doing two things at once” or “remembering new information”) (13). The items are based on the cognitive domains most affected after stroke, being speed of information processing, orientation, attention, memory, executive functioning, praxis, visuospatial functioning and language. The CLCE-24 was conducted by a research assistant, who scored “0” for absence and “1” for presence of complaints; the sum score indicates the number of experienced complaints (range 0–13). The CLCE-24 is a feasible and valid instrument to use in stroke patients (13, 26).
Demographic characteristics included sex, age and level of education. The study recorded the patients’ level of education, ranging from 1: did not finish primary school, to 7: university education (27). The hemisphere involved, the type of stroke (ischaemic or haemorrhagic), history of previous stroke(s), and discharge destination were obtained from medical charts. The severity of stroke was assessed with the National Institutes of Health Stroke Scale (NIHSS) (28). ADL was assessed by the BI (29). Comorbidity was scored on the Cumulative Illness Rating Scale (CIRS) (30), assessing physical impairment based on the function of 13 organ areas. On a 5-point scale (score 0–4) the degree of severity is measured, ranging from “none” to “extremely”. The total comorbidity score is the sum of all 13 items.
Cognitive performance was assessed with the Montreal Cognitive Assessment (MoCA) (17). Cognitive domains assessed include visuospatial functioning, executive functioning, language, memory, attention, abstract reasoning, and orientation. Scores range from 0 to 30, where higher scores indicate better cognitive performance. Patients with < 12 years of education were assigned one additional point.
To study anxiety and depressive symptoms the Hospital Anxiety and Depression Scale (HADS) was administered (31). This scale consists of 14 items (7 about depression, 7 about anxiety) scored on a 4-point scale (score 0–3, higher scores indicating more symptoms).
Psychological factors included proactive coping, passive coping, self-efficacy, optimism, pessimism, extraversion and neuroticism. All measures concerning these psychological factors have good psychometric properties for use in stroke patients (33–36). Proactive coping was measured using the Proactive Coping Competence Inventory (PCI) (32). The PCI consists of 21 items scored on a 4-point scale, with scores of competence ranging from “not at all” to “very”. An example question is “To what extent do you have the capacity to recognize signals that something might go wrong”.
Passive coping was measured with the passive reaction pattern subscale of the Utrecht Coping List (UCL-P) (33). This subscale consists of 7 items, which are scored on a 4-point scale ranging from “seldom” to “very often” (e.g. “taking refuge in fantasies”).
Self-efficacy was measured with the General Self-Efficacy Scale (GSES) (34). This scale consists of 10 items scored on a 4-point scale, ranging from “not at all true” to “exactly true” (e.g. “I am confident that I could deal efficiently with unexpected events”).
Optimism and pessimism were assessed with the Life Orientation Test-Revised (LOT-R) (35). This test consists of 10 items; 3 items measuring optimism (e.g. “In uncertain times, I usually expect the best”), 3 items measuring pessimism (e.g. “If something can go wrong for me, it will”) and 4 distractor items. Items are scored on a 5-point scale, ranging from 0: “strongly disagree” to 4: “strongly agree”.
Extraversion and neuroticism were measured with the Eysenck Personality Questionnaire Revised Short Scale, consisting of 12 items on extraversion (EPQ-SS-E) and 12 items on neuroticism (EPQ-SS-N) (36). The items have dichotomous (yes/no) response options (e.g. “Are you a talkative person” on the extraversion scale, and “Does your mood often go up and down?” on the neuroticism scale).
Statistical analyses
Descriptive statistics were used to describe patients’ characteristics. Level of education was dichotomized into low (1–5) and high education (6–7; finished higher secondary or university education).
As a first step, this study explored the profile of separate SCC over time in complete cases only. Proportions of patients experiencing cognitive complaints on the separate items of the CLCE-24 were calculated at each time-point. Cochran’s Q tests were used to compare the proportions of patients experiencing SCC between the 3 time-points. In case of a significant Cochran’s Q test, post-hoc comparisons were performed using McNemar’s tests. Bonferroni correction for multiple testing was used leading to a p-value of 0.05/11 = 0.004 for Cochran’s Q tests and 0.05/3 = 0.017 for the post-hoc McNemar’s tests.
As a second step, this study explored the temporal evolution of SCC by using random coefficient analyses. All available data can be used with this statistical technique. The CLCE-24 cognition score was used as the dependent variable and time as the independent factor, which allowed for modelling and examination of the effect of time (2 months, 6 months, and 4 years). SCC might increase and decrease again over time (curvilinear trend), which is why we added both linear and quadratic time effects to the model. Time was added as a continuous variable. Likelihood ratio tests were used to assess model fit. Herewith, it was examined whether the addition of a quadratic time function added to the linear model. Likewise, random intercept and slopes and covariance structures were specified according to best fit.
The final step of the statistical analyses included the examination of predictors of SCC at 4 years post-stroke. This included grouping of the separate psychological factors into adaptive and maladaptive factors, based on theory and exploratory factor analyses of Wijenberg et al. (37). Proactive coping, self-efficacy, extraversion and optimism are adaptive psychological factors, whereas passive coping, neuroticism and pessimism are maladaptive psychological factors. Standardized scores (z-scores) were used as common metric, which were then averaged to obtain a total score of the adaptive psychological factors and maladaptive psychological factors separately.
Then, bivariate associations of demographic characteristics (age, sex, education), stroke-related factors (recurrence, NIHSS, BI, discharge destination), comorbidity (CIRS), cognitive performance (MoCA), cognitive complaints at 2 months (CLCE-24), emotional problems (HADS), adaptive and maladaptive psychological factors at 2 months, with the CLCE-24 cognition score at 4 years post-stroke were tested using bivariate multilevel modelling. Bivariately statistically significant associated variables (p < 0.05) were entered in a multivariate multilevel model regression analysis to determine the predictors of CLCE-24 cognition scores at 4 years post-stroke. Analyses were performed with IBM SPSS Statistics version 25.
Subjects
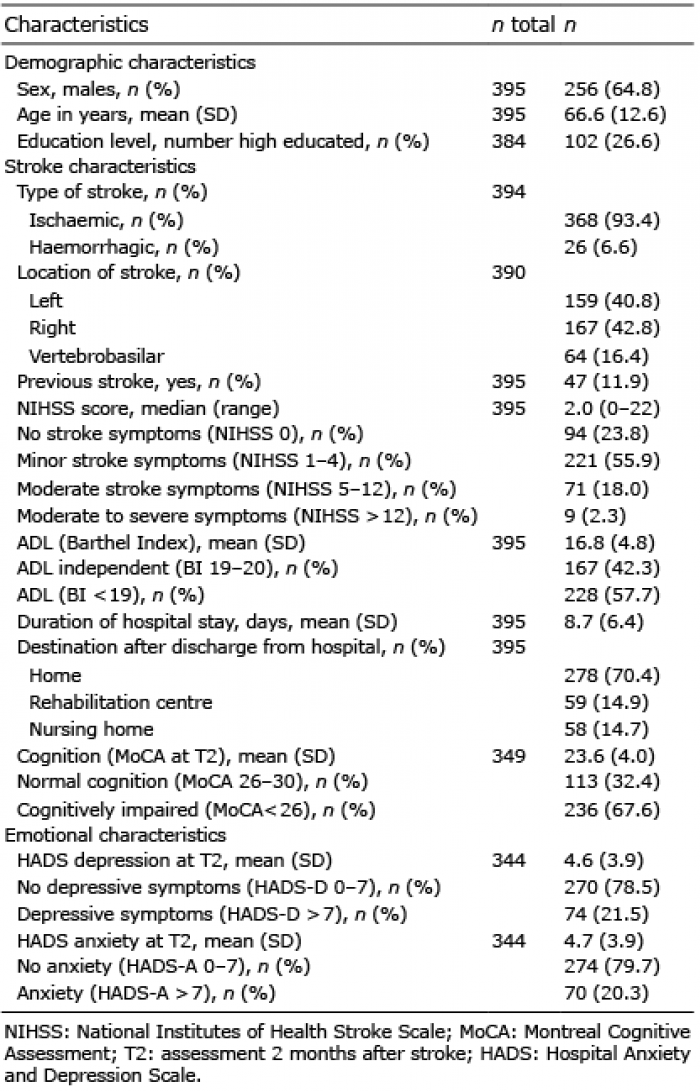
A total of 395 patients were included in the Restore4Stroke cohort study (Table I). At the onset of stroke, mean age was 66.6 years (SD 12.6), 64.8% of the patients were male, and 93.4% suffered an ischaemic stroke. During the course of the study, 235 patients were lost to follow-up (flowchart shown in Fig. 1). CLCE-24 cognition scores were available for 350 patients at T2, 342 patients at T3, and 157 patients at T4. Complete data on the CLCE-24 for all time-points were available for 121 patients (30.6%). Compared with the 274 patients without complete CLCE-24 data, the complete cases (n = 121) were significantly younger (mean 64.2 vs 67.7 years, p = 0.006), and their MoCA-scores at T2 were significantly higher (mean score 24.5 vs 23.0, p = 0.001). For all other variables, there were no significant differences between groups.
Table I. Characteristics of stroke patients (n = 395) at baseline
Fig. 1. Flowchart of participants in the Restore4stroke cohort study. T1: stroke onset; T2: 2 months; T3: 6 months; T4: 4 years post-stroke.
Profile of cognitive complaints over time in complete cases
At 2 months post-stroke, 76.0% of patients reported at least onecognitive complaint. At 6 months this percentage was 71.9%, and at 4 years post-stroke 89.3% of patients reported at least one cognitive complaint (p < 0.001). The mean number of cognitive complaints per patient was 3.2 (SD 2.9) at 2 months, 2.9 (SD 2.7) at 6 months, and 4.1 (SD 2.9) at 4 years after stroke (p < 0.001). The most-often reported SCC were mental slowness, problems with multitasking, memory problems for new information, and attention problems (Table II). In post-hoc analyses, complaints with remembering new information, remembering old information and taking initiative showed significant higher proportions at 4 years than at 2 or 6 months post-stroke (p < 0.017). The proportion of complaints about the item “perception of time” decreased significantly from 2 to 6 months post-stroke (p < 0.017). The proportions of complaints about the other cognitive domains remained stable over time.
Table II. Proportion of stroke patients with cognitive complaints on separate items of the CLCE-24 at 2 months, 6 months, and 4 years post-stroke (n = 121)
Temporal evolution of cognitive complaints (random coefficient analysis)
The best fitting model of CLCE-24 cognition score over time showed a curvilinear trend, including a significant linear (b = –0.099, p = 0.006) as well as a significant quadratic time effect (b = 0.002, p = 0.001). This curvilinear trend (U-shape) is shown in Fig. 2, which shows an initial small decrease in SCC between 2 and 6 months, followed by a larger increase in SCC up to 4 years after stroke.
Fig. 2. CLCE-24: Checklist for Cognitive and Emotional consequences of stroke. (CLCE-24) cognition scores over time by estimated marginal means (EMM) of multilevel growth model including significant linear and quadratic time effects
Determinants of cognitive complaints
Bivariate analyses showed that a recurrent stroke, worse cognitive performance (MoCA), more SCC (CLCE-24) at T2, more depressive symptoms (HADS-D), more anxiety (HADS-A), lower adaptive psychological score and higher maladaptive psychological score were significantly associated (p < 0.05) with higher scores on the CLCE-24 cognition domain (i.e. more SCC) at 4 years post-stroke (Table III).
In the multivariate multilevel model, experiencing more SCC at 2 months was the strongest predictor of experiencing more SCC at 4 years post-stroke. Accounting for SCC at 2 months, higher scores on both adaptive and maladaptive psychological factor scores were significant independent predictors of fewer SCC at 4 years post-stroke (Table III).
Table III. Univariate and multivariate analyses of independent variables (0–2 months post-stroke) and CLCE-24 cognition score at 4 years post-stroke (n = 395)
This study showed that the presence of SCC increases over time up to 4 years after stroke. At 4 years post-stroke, 89.3% of patients reported at least one cognitive complaint, compared with proportions at 2 and 6 months post-stroke of 76.0% and 71.9% respectively. Furthermore, the number of SCC per patient was significantly higher at 4 years post-stroke (mean 4.1 (SD 2.9)). Significant independent predictors of SCC at 4 years post-stroke were SCC at 2 months, adaptive psychological factors, and maladaptive psychological factors.
The increase in SCC over time is in accordance with the results of other studies (9, 11). This increase could be explained by heightened awareness of and/or confrontation with more cognitive difficulties in daily life. In current society, where everything gets faster and more complex (i.e. digital society), it might be difficult for patients to keep up and engage. The fact that mental slowness was the most often reported complaint supports this hypothesis. Since mental speed is often affected in stroke patients, reintegration into society might be difficult after stroke, because patients may have the feeling that they can no longer meet the expectations of society. This might also explain why SCC are strongly associated with participation restrictions after stroke (18). The onset of mild cognitive impairment/dementia, or a more general process of ageing during the follow-up period, might also have played a role in the increase in SCC (38).
The observation that the prevalence and number of SCC decreased slightly between 2 and 6 months post-stroke might be explained by the fact that cognition improved during this period, since most recovery occurs in the first 6 months post-stroke (39). Another explanation might be that, during this period, patients are focusing mainly on recovery, being aware that they survived a stroke. After that, patients are resuming their daily life activities, such as household, hobbies and work, and are confronted more by heir cognitive problems (40). Van Rijsbergen et al., who also used the CLCE-24, recently showed that SCC remained stable between 3 and 12 months after stroke (14). The mean number of complaints in the early phase after stroke (3.3 (SD 2.4) at 3 months) in their study is identical to the mean number of complaints in the early phase (3.2 (SD 2.9) at 2 months) in the current study. It may be possible that some recovery occurred between 3 and 6 months in their patients, which was, however, not observed because they did not include a 6-month observation. In extent, SCC may have increased from 6 to 12 months, leading to a stable level of SCC over time, as observed in their study. In the current study, the number of SCC at 12 months after stroke returned to the same level as the number at 2 months after stroke (Fig. 2), implying a stabilization of SCC between 2 and 12 months after stroke.
The increase in prevalence of SCC could not be explained by an accompanied increase in prevalence of cognitive deficits, as assessed with the MoCA. In complete cases, at 2 months 58.7% of patients were cognitively impaired (MoCA< 26), at 6 months 41.3%, and at 4 years post-stroke 48.8% (results not shown). Although the bivariate association between MoCA and CLCE-24 cognition score was significant, MoCA-score at 2 months was not a significant independent predictor of SCC at 4 years post-stroke in multilevel multivariate analysis, since psychological factors made the significant bivariate effect disappear. Our findings are in line with earlier studies that did not find objective cognitive functioning to be a significant independent predictor of SCC when depressive symptoms, fatigue, coping or personality traits were taken into account (2, 7, 14).
No independent significant relationship was found between depressive symptoms and SCC. Although previous studies mainly found depressive symptoms to be associated with more SCC in multivariate analyses (2, 7, 19, 23), there is one other study that did not find this significant relationship (22). Presumably, the different results depend on which factors are taken into account. As in the current study, the other study (22) added personality traits to the multivariate model, which could have cancelled out the effect of depressive symptoms.
In the current multilevel multivariate analysis, surprisingly, not only higher scores on adaptive psychological factors, but also higher scores on maladaptive psychological factors were independently related to fewer SCC at 4 years post-stroke. It is difficult to interpret why maladaptive psychological factor scores correlated positively with SCC at 4 years in the bivariate analysis (indicating an unfavourable effect of having more SCC), while the correlation coefficient changed to negative in the multivariate analysis (indicating a beneficial effect of having fewer SCC). In the multivariate analysis, maladaptive psychological factors continued to correlate positively with SCC at 4 years post-stroke until the factor SCC at 2 months was added to the model. Hence, maladaptive psychological factors in themselves actually have an unfavourable effect on long-term SCC. This seems quite logical, and is in accordance with previous research, since passive coping and neuroticism have shown to be associated with more SCC in patients with stroke (7, 22). It is unclear why the unfavourable effect of maladaptive psychological factors on long-term SCC was reversed by the presence of SCC at 2 months in the multivariate model. Our hypothesis is that patients scoring high on maladaptive psychological factors at baseline report more SCC at baseline. Extra analyses were performed, which showed that patients with many maladaptive psychological factors (> 1 SD) had higher number of SCC (mean 5.8) than patients with moderate (–1 to 1 SD) or few (≤ 1SD) maladaptive factors (mean 3.0 and 1.6 respectively). Because of these higher baseline SCC scores, they are less likely to show a further increase in SCC over time compared with the patients with lower scores on maladaptive factors. The “SCC change score” (calculated as SCC score at 4 years post-stroke minus SCC score at 2 months post-stroke) even became negative in the group with many maladaptive factors. The current study also found that higher scores on maladaptive psychological factors correlated significantly with a lower SCC change-score (r = –0.248, p = 0.002). Since our hypothesis is speculative, future research is needed to determine the mechanisms behind these results.
The beneficial effect of adaptive psychological factors on the temporal evolution of SCC found in this study is in accordance with previous literature, since proactive coping and self-efficacy have previously been associated with fewer SCC after stroke (7, 23, 41).
One of the strengths of the current study is its generalizability. The stroke patients were recruited from stroke units in general hospitals, and most had had a minor stroke, which is representative of the stroke population nowadays. Due to the rapidly evolving field of acute stroke care, with increasing numbers of patients receiving intravenous thrombolysis and/or intra-arterial thrombectomy, survival rates increase and functional outcomes improve. With increasing numbers of minor strokes, the invisible consequences of stroke, such as cognitive problems, will play a greater role in rehabilitation. Furthermore, the measures used in the current study (like the CLCE-24 and the MoCA) are also used in clinical practice.
However, some limitations of the current study should be mentioned. First, the results were not compared with a demographically matched control group. Since SCC are also present in the general population, it is unclear whether the high prevalence of SCC in our stroke population is mainly attributed to the stroke. However, earlier research concluded that, based on the CLCE-24, stroke patients reported more SCC than healthy controls (42). Secondly, it is not known if the increase in SCC over time could have been influenced by new vascular damage, since imaging of the brain was not repeated in the long-term after stroke. Finally, the attrition rate in complete cases was quite high. Selection bias may have played a role in complete cases analyses, since the complete cases were younger and less cognitively impaired compared with the total group. However, complete cases were only used in the proportion analyses (Table II). In all other analyses, the use of multilevel analyses enabled information for all included participants to be used, not only the complete cases.
In conclusion, during follow-up of stroke patients it is important to assess SCC, since they may interact with participation and quality of life after stroke. Psychological factors in the early phase after stroke should be examined, since they may influence the extent of SCC in the long-term. Although the effect of maladaptive psychological factors on SCC is difficult to interpret in multivariate analysis, the fact is that they are associated with more SCC in the long-term after stroke. This underlines the importance of taking psychological factors into account during rehabilitation (who is the “person behind the stroke”?), which may eventually result in better, personalized care. When SCC are present it is also important to provide some psycho-education; for instance, about the fact that SCC are not naturally accompanied by cognitive deficits, and that the way one deals with the consequences of stroke (depending on psychological factors) plays a role in the degree of complaints.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize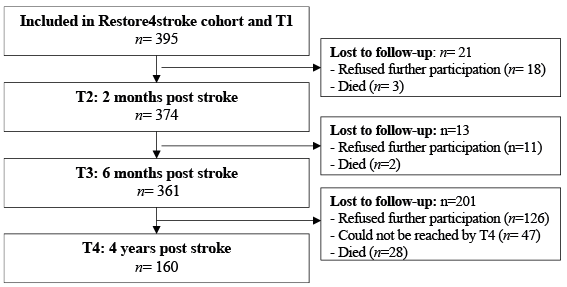 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize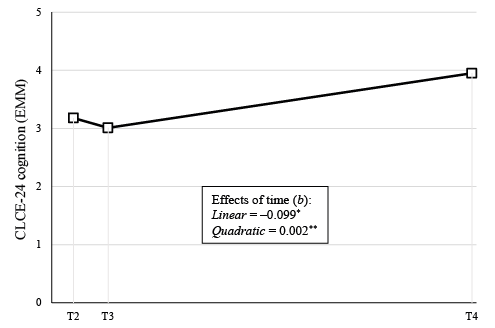 Click to show fullsize
Click to show fullsize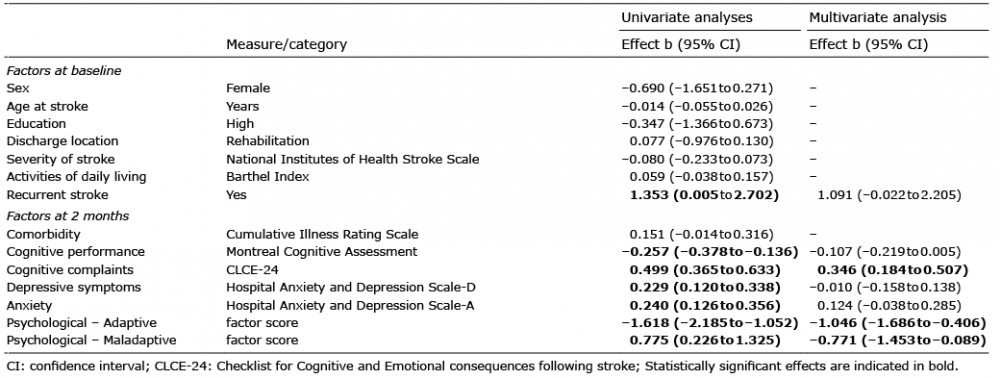 Click to show fullsize
Click to show fullsize