
From the 1Hanover Medical School, Department of Rehabilitation Medicine, 2Hanover Medical School, Department of Psychiatry, Social Psychiatry and Psychotherapy, 3Hanover Medical School, Department of Sports Medicine, 4Hanover Medical School, Human Ressource Management, Hanover, Germany
Objectives: To set up a comprehensive health programme for employees, with needs-based allocation to preventive and rehabilitative measures; and to evaluate the effects of the programme on work ability and sick leave.
Design: Prospective single-group observational study.
Methods: Employees of a university hospital were invited to participate in needs-based interventions of preventive or rehabilitative character. Allocation followed screening questionnaires, anamnesis and clinical examination. The selection of a preventive or rehabilitative measure appropriate to the needs of the patient followed screening questionnaires, anamnesis and clinical examination. Preventive offers can include back training courses, water gymnastics or stress management exercises. Rehabilitative measures can include 3-6 weeks in- or outpatient rehabilitation or one week intensive outpatient rehabilitation. The main outcome parameters were work ability and sick leave duration.
Results: At this time of the project included 1,547 participants, who applied voluntarily to enter the programme. The mean age of participants was 44.3 years (standard deviation (SD) 10.3 years), and 72.0% were female. Needs-based allocation to a prevention (n=1,218) or a rehabilitation group (n=329) was effective, and enabled formation of 2 groups with different needs. Overall, more than half of the employees participating in the programme reported sick leave within the last 3 months. Participants in the preventive measures group reported significantly lower duration of sick leave than those in the rehabilitation group. Employees in the rehabilitation group had significantly lower work ability (Work Ability Index (WAI) 30.4 vs 36.6), but higher effects at 6-month follow-up (WAI 33.4 (standardized effect size (SES) 0.51) vs 37.9 (SES 0.17)). In the prevention group mean sick leave reduced significantly from 1.9 to 1.3 weeks (p < 0.001) during the previous 3-month period, whereas in the rehabilitation group it reduced from 2.7 to 1.5 (p < 0.001) weeks.
Conclusion: Implementation of the comprehensive health programme was successful, using the multimodal infrastructure of a university hospital. Allocation to suitable interventions in occupational health programmes following screening, anamnesis and clinical examination is an appropriate way to meet participants’ needs. The programme resulted in improved work ability and less sick leave.
Occupational health programmes are important to improve and maintain employees’ health and work ability. Each employee has an individual need for measures, and meeting those needs can be the key to improving their situation. Allocation to different preventive or, if necessary, rehabilitative measures, in the comprehensive programme “Fit for Work and Life”, was performed by a doctor after obligatory consultation. This ensured the best possible effects of the invested resources. Participants allocated to rehabilitation measures had lower initial work ability and higher sick leave durations, but showed higher improvements in outcome parameters than participants in the preventive group.
Key words: vocational rehabilitation; employment; occupational health; preventive health programme; work-site intervention.
Accepted Mar 12, 2021; Epub ahead of print Mar 30, 2021
J Rehabil Med 2021; 53: jrm00199
Correspondence address: Christoph Korallus, Department of Rehabilitation Medicine, Coordination Centre for Rehabilitation Research, Hannover Medical School, Hanover, Germany. E-mail: korallus.christoph@mh-hannover.de
Doi: 10.2340/16501977-2822
Incapacity for work and work-related health problems have a high economic impact, in addition to affecting the overall quality of life of employees (1–3). In Germany, as in most western European countries, musculoskeletal conditions and mental health problems, in addition to acute airway and gastrointestinal disease, are the main causes of inability to work (4).
In Germany, pension insurance funds inpatient or outpatient rehabilitation programmes for patients with chronic health conditions. The prerequisite for assignment to such rehabilitation measures is a relevant restriction in occupational performance. This criterion restricts rehabilitation measures to employees with severe health problems and neglects the principle of early intervention. However, such early intervention is important to avoid the development of chronic (generalized) pain syndromes or mental health issues (5).
As the effects of inpatient rehabilitation programmes on return-to-work are limited (6), within the last decade so-called “medical-occupational rehabilitation programmes” have been developed and evaluated (6–8). Implementation of occupational interventions and job-oriented training leads to much better outcomes of rehabilitation programmes (8–11). However, even in the companies providing these programmes, no direct communication between the rehabilitation physicians or therapists and the doctors responsible has been established. Such communication was one of the core elements of the so-called JobReha programmes (JobReha represents the rehabilitative path of the current fit for work and life program)(12, 13).
With the goal of improving health and performance of employees of Hannover Medical School and to reduce their sick leave, the Department of Rehabilitation Medicine and the human resources department, with support from the regional Pension Insurance, developed a comprehensive health programme for employees of Hannover Medical School. In order to include preventive measures and to respond to mental health problems, the Departments of Sports Medicine and Psychiatry were included in the working group.
Based on previous projects (12, 14), a comprehensive programme to improve health and work ability was developed and implemented at Hannover Medical School (15, 16). Hannover Medical School is a university hospital at tertiary level of care, with approximately 7,500 employees in a wide range of jobs (science, medical care, teaching, technical jobs, service and others). As a medical university, it has various research laboratories and teaching departments. The hospital has approximately 1,500 beds and 450,000 outpatient contacts per year.
The main goals of the programme were:
This study sets out the results of the evaluation of the programme during the implementation phase.
“Fit for Work and Life” interventions
The programme called “Fit for Work and Life” (FWL) was designed with the following main principles:
The programme includes preventive and rehabilitative measures as well as fast-track physical therapy.
Participation in the programme is voluntary; there is an open invitation for participation to all employees, with information distributed via flyers, posters, the hospital website homepage, and e-mail.
Assignment to the different measures of the programme is coordinated and led by 2 specialized medical doctors: 1 from the Department of Sports Medicine and 1 rehabilitation specialist (based on assessment questionnaire and a clinical investigation).
All interventions aim at the employee remaining at the current workplace (participants have to commit themselves to this goal).
Mental health problems are taken into account (this also applies even if physical complaints are in the foreground).
Participants are motivated to continue preventive exercise after the end of the programme.
The programme combines specially designed interventions financed by the employer with standard interventions paid for by health and pension insurances.
Measures to improve working conditions are integrated into the programme (ergonomics, good leadership).
Participation in the programme is free of charge for participants; rehabilitative measures and therapies are accounted as working time; for preventive measures 50% are accounted as working time.
If general problems of work organization or team conflicts become evident, the problems will be discussed in a “trust board” with the participation of representatives of the management and of the employee representative committee.
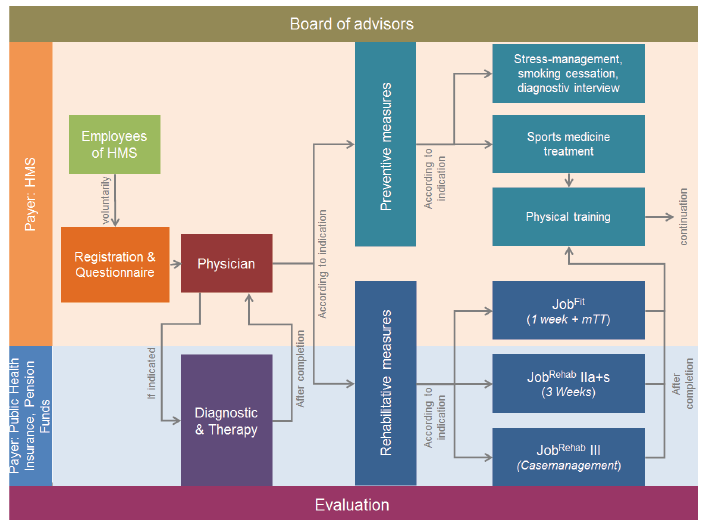
After registration in the programme, the participants have to complete a set of assessment questionnaires, including Work Ability Index (WAI) (17), Hospital Anxiety and Depression Scale (HADS) (18) and the 36-item Short-Form Health Survey (SF-36) (19). In a doctor’s consultation (physical and rehabilitation medicine (PRM) or sports medicine specialist), the decision is made whether the participant undergoes preventive or rehabilitation measures (Fig. 1). The decision is based on categories (“Poor work ability” 7–27, “Moderate” 28–36, “Good” 37–43, and “Excellent” 44–49) of the WAI screening questionnaire, while taking many other factors of anamnesis, clinical examination and goals into account. Participants with poor or moderate work ability are more likely to be assigned to rehabilitative interventions.
Rehabilitative measures include the following 3 options:
A 1-week outpatient prevention programme with rehabilitative elements (“JobFit”), consisting of, for example, exercise therapy, physiotherapy and occupational therapy with workplace analysis, psychological talks, aqua gymnastics and relaxation therapy, accompanied by team meetings (at the Department for Rehabilitation Medicine) (20).
A 3–4-week inpatient multimodal rehabilitation programme according to the standards of the German pension insurance fund (“JobReha”) (21) (at the Rehabilitation centres with collaboration agreement)
Individual case management according to the rules of the regional pension insurance fund (at the Deutsche Rentenversicherung Braunschweig-Hannover).
Preventive measures include the following options:
Physical exercise (at the Department of Sports Medicine).
Empowerment courses, stress compensation, diagnostic interviews (at the Department of Psychiatry).
Intervention for smoking cessation (at the Department of Psychiatry).
In case of acute musculoskeletal conditions, employees can contact a PRM physician in the Department of Rehabilitation Medicine directly. They undergo a medical examination and are treated as far as manual medicine and other PRM interventions are indicated. In addition, employees can receive physiotherapy and other physical modalities. In order to avoid any delays in treatment, fast-track registration is possible for employees with acute musculoskeletal problems. For employees with acute mental health problems, supportive and diagnostic sessions and, if needed, psychotherapy are provided by the Department of Psychiatry at short notice. In addition to all individual measures, it is also possible to take advantage of ergonomic consulting and coaching for executive personnel on a departmental basis.
“Fit for Work and Life” interventions
After registration in the programme, the participants have to complete a set of assessment questionnaires, including Work Ability Index (WAI) (17), Hospital Anxiety and Depression Scale (HADS) (18) and the 36-item Short-Form Health Survey (SF-36) (19). In a doctor’s consultation (physical and rehabilitation medicine (PRM) or sports medicine specialist), the decision is made whether the participant undergoes preventive or rehabilitation measures (Fig. 1). The decision is based on categories (“Poor work ability” 7–27, “Moderate” 28–36, “Good” 37–43, and “Excellent” 44–49) of the WAI screening questionnaire, while taking many other factors of anamnesis, clinical examination and goals into account. Participants with poor or moderate work ability are more likely to be assigned to rehabilitative interventions.
Rehabilitative measures include the following 3 options:
Preventive measures include the following options:
In case of acute musculoskeletal conditions, employees can contact a PRM physician in the Department of Rehabilitation Medicine directly. They undergo a medical examination and are treated as far as manual medicine and other PRM interventions are indicated. In addition, employees can receive physiotherapy and other physical modalities. In order to avoid any delays in treatment, fast-track registration is possible for employees with acute musculoskeletal problems. For employees with acute mental health problems, supportive and diagnostic sessions and, if needed, psychotherapy are provided by the Department of Psychiatry at short notice. In addition to all individual measures, it is also possible to take advantage of ergonomic consulting and coaching for executive personnel on a departmental basis.
Fig. 1. Flowchart of “Fit for Work and Life” programme at Hanover Medical School (HMS). Regular team meetings were held and the outcomes of the programme evaluated. JobFit:one week intensive outpatient rehabilitation; JobRehabIIa: 3-6 weeks outpatient rehabilitation; JobRehabIIs: 3-6 weeks inpatient rehabilitation; III: 3-6 weeks rehabilitation following a case management; mTT: medical training therapy.
Study design
As part of the registration process, all participants completed a screening questionnaire (baseline) regarding work ability (WAI) (17) in the official German translation (22), quality of life (SF-36) (19) and mental disorders (HADS) (18).
For the programme-related voluntary evaluation, questionnaires were sent to the employees 3, 6 and 12 months after the beginning of the intervention, to monitor quality of life (SF-36) and work ability (WAI).
In addition, the total number of weeks of sick leave in the previous 3 months was assessed in order to determine the change in participation in working life after interventions.
All subjects could take part in the programme only once and provided signed informed consent for use of their personal data. The study was approved by the clinical ethics committee of Hanover Medical School (vote number 6351).
Statistical analysis
The FWL programme and accompanying evaluation is ongoing. Therefore, only employees who started their intervention at least 6 months before the presented analysis were included in the data analysis. Data were analysed on an intention-to-treat basis. In case of missing values, the last observation was carried forward.
Sample characteristics were analysed by descriptive statistics. The accuracy of the patients’ referral to the intervention was evaluated by t-tests for independent samples or Pearson’s χ2 test, respectively. Differences between measurements at baseline and 6 months follow-up were compared using paired t-tests separately for the intervention and the rehabilitation group. Test statistics were regarded as significant if the two-sided p-value was less than 0.05.
To calculate intragroup effects, the mean differences in follow-up and baseline measurements were divided by the corresponding baseline SD (standardized effect size (SES)). SES were interpreted according to Cohen’s effect size conventions (SES ≥ 0.2: small; SES ≥ 0.5: medium; SES ≥ 0.8: large). (23) All analyses were conducted using SPSS version 25.0 (IBM, Armonk, NY, USA).
The programme started in July 2013. Until October 2018, 1,687 employees registered for the programme and agreed to participate in the accompanying evaluation (Fig. 2). A total of 1,547 persons started their preventive or rehabilitative measures at least 6 months before the presented analysis.
The sample characteristics for the total sample, as well as the 2 intervention groups, are shown in Table I. In the whole sample, 72.0% of participants were female and the mean age was 44.3 years (SD 10.3), while the hospital’s staff shows an overall proportion of 66.1% women. Approximately 16% of the participants were referred to the programme by the occupation integration management. Nearly half of employees reported sick leave within 3 months prior to the consultation, resulting in a mean sick leave of 2.1 weeks in the previous 3 months (SD 3.4). More than half of participants (51.2%) reported a low-to-moderate work ability.
Assignment to the intervention groups appears to be needs-based. Participants of rehabilitative measures reported a significantly higher rate of sick leave (68.3% or 2.7 weeks within the last 3 months vs 52.9% or 1.9 weeks within the last 3 months) and lower values on WAI (30.4 vs 36.6) than participants of preventive measures. The majority of employees (85.8%) who were assigned to rehabilitative measures showed a low-to-moderate work ability (Table I). Assignment to measures did not differ significantly between PRM and sports medicine specialists (p = 0.099).
Participants receiving preventive interventions reported statistically significant (p < 0.001) improvements in both outcomes: duration of sick leave and WAI, in the first 6 months (Table II). However, the changes did not exceed a small effect size (SES = 0.17–0.25).
Small-to-medium effect sizes could be shown for the rehabilitative measures. Participants improved significantly (p < 0.001) regarding work ability (SES = 0.51) and sick leave (SES = 0.43).
Fig. 2. Flowchart of participants. JobFit:one week intensive outpatient rehabilitation; JobRehabIIa: 3-6 weeks outpatient rehabilitation; JobRehabIIs: 3-6 weeks inpatient rehabilitation.
Table I. Sample characteristics at baseline
Table II. Outcomes at 6-month follow up
The main intention of the “Fit for work and Life” concept is to create an occupational health programme that offers needs-based interventions to the participants. Because of this individual support it should be highly attractive to the employees. Regarding the number of applications in the first period of implementation, we conclude that this kind of opportunity is well-appreciated by the employees. Assignment to preventive or rehabilitative measures follows a decision process, where, in addition to WAI, other factors, such as the complexity of the condition or the demand of multimodal therapy are included. The differences between the preventive and rehabilitative groups led to the conclusion that the process of assignment to the 2 groups was effective. Participants entering rehabilitative measures showed a low-to-moderate work ability in 85.8% of cases, while this applied to less than half of the participants in the prevention group. However, 14.2% of the participants in the rehabilitation group showed good work ability. This can be explained by other factors taken into consideration in the assignment process, such as the clinical examination, which could show the need for a multimodal approach as an example.
In previous projects, as for JobReha, there were difficulties in needs-based allocation, as the results indicated a definition of interventional need by physical demand of occupational activity, rather than by actual work ability (24).
The results for the main outcome parameters in this study, work ability and sick leave, show statistically significant improvements in working ability in both, prevention and rehabilitation group. In the rehabilitation group, especially, this leads to a medium effect size (SES=0.51). Taking into account the unknown minimal detectable change (MDC) and minimal clinical important difference (MCID) for the WAI, the analysis cannot currently be extended, but the significant reduction in sick leave is notable. Both the economic perspective and the reduction in sick leave support the value of this occupational health programme. Such programmes also promote participation across many other areas of life. A significant reduction in sick leave duration was found in both groups, with rather small effect sizes. Further studies will include consideration of the economic outcome. This is a key factor in establishing the concept as an integral component of long-term health strategies of our university hospital.
The next step in the current programme is to validate these data by collecting more long-term results and including a 12-month follow-up in the analysis.
Strengths and limitations
The current project received major financial support from our hospital, which provides a good deal of financial leeway and gives employees the feeling that their health is being taken seriously. However, the budget requirement makes it difficult to transfer the project to other companies. A further limitation of the current study is the asymmetrical allocation to interventions, which reflects the need of the employees, but also leads to a small number of participants in the rehabilitation group. The project is subject to a high level of data protection restrictions. In particular, collection of medical diagnoses, and processing of already collected findings from the patient archives or the workplace have been rejected by staff representatives. Therefore some results are not assessable, although the participants’ confidence provides the opportunity to receive the best possible impression of their needs. Extension of the current occupational health management programme is planned, in order to confirm these preliminary results.
This comprehensive health programme was successfully implemented using the multimodal infrastructure of a university hospital. The main factors in the success of this programme seem to be the voluntary nature of participation, and the integration of the programme into the company culture. Furthermore, the study shows the importance of assignment to preventive and rehabilitative measures, informed by assessment tools and clinical investigation. Clear goal-setting was used regarding staying at work (not only better general health). Finally, a main factor in reaching a large proportion of the employees was the opportunity for them to participate without financial contribution, based on combined financing from health insurance, pension insurance and the university itself. Overall, the programme resulted in improved work ability and less sick leave.


 Click to show fullsize
Click to show fullsize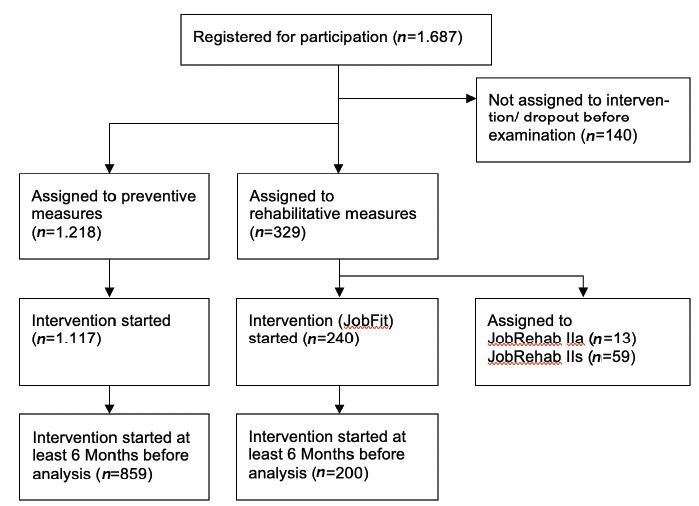 Click to show fullsize
Click to show fullsize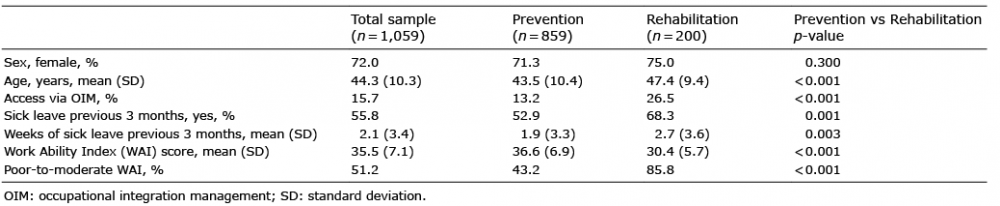 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize