
From the 1University of Ljubljana, Faculty of Medicine, 2Department of Neurology, General Hospital Celje, Celje, 3Neurorehabilitation Unit, Department of Neurology, University Medical Centre Ljubljana, 4University of Ljubljana, Faculty of Sport, 5Clinical Institute for Radiology, University Medical Centre Ljubljana, 6University of Ljubljana, Faculty of Electrical Engineering and 7Department of Neurology, University Medical Centre Ljubljana, Ljubljana, Slovenia
Background: There is insufficient knowledge about how aerobic exercise impacts the disease process of multiple sclerosis, which is characterized by accumulation of white matter lesions and accelerated brain atrophy.
Objective: To examine the effect of aerobic exercise on neuroinflammation and neurodegeneration by magnetic resonance imaging and clinical measures of disease activity and progression in persons with multiple sclerosis.
Patients and methods: An exploratory 12-week randomized control trial including an intervention group (n = 14, 12 weeks of aerobic exercise twice weekly) and a control group (n = 14, continuation of usual lifestyle). Primary outcomes were magnetic resonance imaging measures (lesion load, brain structure volume change), while secondary outcomes included disability measures, blood cytokine levels, cognitive tests and patient-reported outcomes.
Results: The effects of aerobic exercise on whole brain and grey matter atrophy were minor. Surprisingly, the observed effect on volume (atrophy) in selected brain substructures was heterogeneous. Putaminal and posterior cingulate volumes decreased, parahippocampal gyrus volume increased, thalamus and amygdala volume remained the same, and active lesion load and count decreased. However, apart from weak improvements in walking speed and brain-derived neurotrophic factor levels, there was no effect of aerobic exercise on other clinical, cognitive or patient-reported outcomes.
Conclusion: These results suggest that aerobic exercise in persons with multiple sclerosis has a positive effect on the volume of some of the substructures of the brain, possibly indicating a slowing of the neurodegenerative process in these regions, but a negative impact on the volume of some other substructures, with unclear implications. Further research is needed to determine whether the slight decrease in active lesion volume and count implies an anti- inflammatory effect of aerobic exercise, and the exact significance of the heterogeneous results of volumetric assessments.
Key words: multiple sclerosis; aerobic exercise; neuroinflammation; neurodegeneration; magnetic resonance imaging; brain atrophy; cognition; cytokines.
The aim of this study was to evaluate the effects of aerobic exercise (physical exercise in the form of aerobics) on people with multiple sclerosis who were being treated with fingolimod. Two groups of patients with multiple sclerosis were studied: an intervention group (n = 14) who undertook 12 weeks of exercise training, and a control group (n = 14) who continued with their usual lifestyle. Magnetic resonance imaging, bloodwork analysis and some other clinical assessments were performed before and after the 12-week period, and the patients completed several questionnaires about their wellbeing and accompanying symptoms of multiple sclerosis. The results suggest that aerobic exercise (combined with appropriate pharmacological treatment) can positively affect some of the brain regions in people with MS by reducing the rate of their degeneration and might decrease the inflammatory activity. However, longer and larger studies should be performed to evaluate whether such rehabilitation is effective and could, in the long-term, possibly slow down the rate of disability accrual.
Accepted Feb 16, 2021; Epub ahead of print Mar 19, 2021
J Rehabil Med 2021; 52: jrm00178
Correspondence address: Lina Savšek, General Hospital Celje, Celje, Slovenia. E-mail: lina.savsek@sb-celje.si
Doi: 10.2340/16501977-2814
Multiple sclerosis (MS) is a chronic immune-mediated disease of the central nervous system (CNS) that is incurable despite the availability of potent disease-modifying drugs (DMDs). Most of the currently available DMDs aim to limit the disease by controlling the inflammatory process in the CNS. However, less is known about how to directly target neurodegeneration, which is dominant in the progressive phase of MS, but can also be present early, in the context of clinically isolated syndrome, and is reflected by whole brain and regional atrophy (1). The aim of this study was to investigate the effect of physical activity in the form of aerobic exercise (AE) on neuroinflammation and neurodegeneration, by quantifying magnetic resonance imaging (MRI) biomarkers, along with clinical, cognitive and patient-reported outcome measures of disease activity and progression in persons with MS (pwMS).
Gerontology literature suggests that AE may decelerate age-related neurodegeneration in certain brain structures, which therefore remain responsive to such an intervention (2). Besides improvements in cardiac and immune function, mechanisms include alterations in trophic factor signalling, modifying the neuronal structure and function (3). However, a systematic review of research in pwMS concluded that there is no strong evidence that confirms a positive or negative effect of exercise on cytokine or adipokine profiles (4). Furthermore, studies on ageing in healthy subjects mostly demonstrate an inverse relationship between physical activity and inflammatory biomarkers (5), while a recent study in young adults found an exercise-induced pro-inflammatory response (6). Exercise in pwMS could thus exhibit disease-modifying effects (7), although there is a lack of data on this subject (8).
PwMS are less physically active than the general population (9), possibly due to disease-related physical disability; however, exercise is considered safe, well tolerated and effective in controlling various disease symptoms (9). For instance, exercise has been shown to reduce fatigue and improve mobility and health-related quality of life (HRQoL) of pwMS and has been found to be effective in improving aerobic capacity and muscular strength (7). Exercise training studies have typically included only pwMS with mild-to-moderate disability, although there is promising evidence for the benefits of exercise training in pwMS with severe mobility disability (10). Most exercise training programmes employed endurance and resistance training, while AE programmes mostly consisted of (treadmill) walking and bicycle training, all performed in a supervised environment (4, 7).
Research on the effects of physical exercise in pwMS has focused predominantly on outcomes such as physical fitness, walking mobility, balance, cognition, fatigue, depressive symptoms, and QoL (8). There are less data on the effects of exercise on MRI biomarkers, such as brain structures and lesions, apart from a few cross-sectional (11, 12) and case studies (13, 14) and a recent randomized control trial (RCT) of progressive resistance training (PRT) (15). The last suggests that PRT can counteract brain atrophy in pwMS, adding to the evidence that exercise might slow the progression of MS (9). Cross-sectional studies on pwMS show that objectively measured levels of physical activity and cardiorespiratory fitness are significantly correlated with volumes of whole brain grey matter (GM), white matter (WM) and deep GM structures, the last being involved in motor and cognitive functions in MS (11, 12). Some case studies (13, 14) have indicated that AE might increase hippocampal volume and integrity in pwMS. Emerging evidence thus indicates that exercise might promote neuroplasticity in pwMS.
The available DMDs each have a different effect on the immune system (16) and MRI parameters (17). Previous studies focusing on the effects of exercise on outcomes, such as cytokines, cognition, mobility, and MRI biomarkers in pwMS (15, 18, 19), have included participants irrespective of the type of DMD treatment they are undergoing, which could be an important confounding factor. To our knowledge, no study has yet investigated whether physical activity, combined with pharmaceutical treatment with a single DMD, might have a role in the management of MS.
The aim of this exploratory randomized controlled trial was to investigate whether AE, performed concurrently with fingolimod treatment, can beneficially modify the disease course in pwMS, by focusing primarily on MRI biomarkers of disease activity and progression, such as lesion load and change in brain structure volume. Secondarily, the impact of AE was evaluated through a comprehensive set of clinical, serological, cognitive and patient-reported outcomes (PROs).
Study design
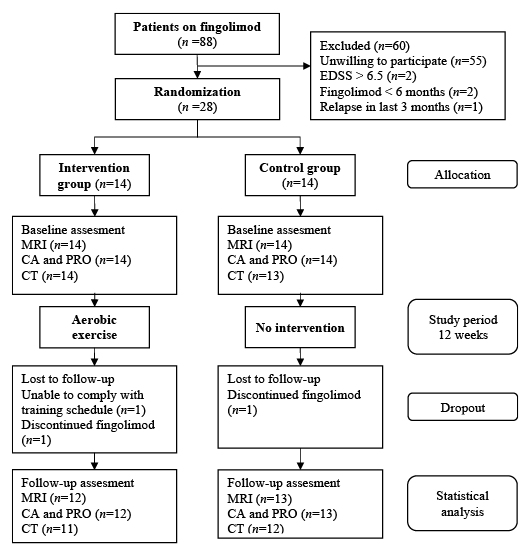
This study is reported in accordance with the CONSORT 2010 statement and CONSORT Extension for Randomized Trials of Non-pharmacological Treatment. It is a RCT with intervention and control groups, without crossover. The study was performed from February to June 2016, whereas the intervention (AE) was carried out from 1 March to 31 May 2016 (12 weeks). Participants were assessed within one month before the start of intervention (at baseline) and after the intervention ended (at follow-up). Evaluation of study participants consisted of a comprehensive set of clinical assessment, MRI, PROs, cognitive testing and blood sampling. The experimental design and participant allocation are shown in Fig. 1.
The study was approved by the Republic of Slovenia National Medical Ethics Committee (0120-660/2015-2).
Fig. 1. Flowchart of experimental design and patient allocation and assessment. EDSS: Expanded Disability Status Scale; n: number of subjects; MRI: magnetic resonance imaging; CA: clinical assessment; PRO: patient-reported outcomes; CT: cognitive testing.
Patients
Patients with MS treated at the MS Centre of the Department of Neurology at the University Clinical Centre Ljubljana were selected based on the following inclusion criteria: (i) relapsing-remitting MS; (ii) treatment with fingolimod ≥ 6 months; (iii) no relapse in previous 3 months; (iv) Expanded Disability Status Scale (EDSS) ≤ 6.5; (v) absence of concomitant disease (e.g. cardiopulmonary, musculoskeletal) or significant cognitive impairment that could affect their physical performance ability.
Patients were initially interviewed about participation in regular exercise. After the initial eligibility check and clinical assessment, a cohort of 28 patients were enrolled in the study and provided written informed consent. Participants were randomly assigned into 1 of 2 groups: an AE intervention (IG, n = 14) and control (CG, n = 14) group. Participants in the IG attended AE sessions (duration 60 min) twice weekly, while those in the CG were asked to continue with their normal daily routine.
Intervention: aerobic exercise
The intervention consisted of organized group AE, led by a certified experienced aerobics trainer. The IG participants performed aerobics twice weekly for 12 weeks, totalling 24 sessions. The duration of each exercise session was up to 60 min, consisting of a 6–10 min warm-up, 30–40 min performed at prescribed intensity, and a 6–10 min cool-down, involving gradual reduction in exercise intensity followed by static muscle stretching. Short 1–2-min individual breaks were taken during the session if needed (due to fatigue, loss of concentration, vertigo, etc.). Exercise intensity during aerobics was assessed using Polar heart rate monitors (Polar Electro, Kempele, Finland) with 24alife Live session software (Mikropis, Žalec, Slovenia) and by the subjective physical sensations as measured by the Borg Rating of Perceived Exertion (RPE) Scale. Participants’ heart rate and percentage of heart rate reserve were projected on a movie screen by 24alife Live session software, to be observed on-line by each participant and the trainer. The aim of the exercise was to train at a moderate intensity level, defined as 60–70% of individuals’ heart rate reserve (Karvonen formula) using age-predicted maximal heart rate, which is equivalent to “somewhat hard” rating on the Borg RPE Scale. With this set-up, the trainer was able to instruct individual participants to follow the prescribed exercise intensity. Several aerobics choreographies, based on simple stepping combinations and body rotations around a vertical axis, were applied to match the abilities of participants to maintain prescribed intensity. In addition to physical strain, such trainer-guided exercises also required cognitive strain; for instance, audio-visual attention, learning to ensure correct exercise execution and keeping pace with the rhythm of the music.
Primary outcome: magnetic resonance imaging and image analysis
Baseline and follow-up high-resolution 3D brain MRI scans were acquired on a 3T Philips Achieva scanner (Philips Healthcare, Best, Netherlands) at the University of Ljubljana, Faculty of Medicine, Infrastructural centre of MR imaging and spectroscopy. Imaging protocol included structural and gadolinium (Gd) enhanced T1 brain MRI scans to assess brain structure volumes and active (T1 Gd enhancing) inflammatory lesions, respectively, and fluid-attenuated inversion recovery (FLAIR) and dual inversion recovery (DIR) MRI scans to assess the respective T2 lesions in the WM and cortical lesions (CLs). Details are given in the Appendix SI, Table SI.
All MRI scans were quantified using MS Markers, an online automated image analysis software service (https://ms.quantim.eu/). The MS Markers extracted contours of WM, cortical and deep GM structures and active, T2 and CLs. Before lesion analysis, an experienced neuroradiologist with more than 10 years’ experience in reading MRI images of pwMS revised the contours in a blinded manner and, where required, manually updated the contours using interactive visualization and contouring tools. Then, volumes and counts and corresponding changes over time were computed for the active, T2 and CLs. Based on lesion masks, a lesion-filling algorithm was used to reconstruct normal-appearing tissue intensity on the pre-processed T1 image before running brain tissue segmentation. For brain volume change analysis, the baseline and follow-up pre-processed and lesion-filled T1 images were aligned using non-rigid registration. By integrating the Jacobian determinant of the obtained image deformation field across segmented brain regions the corresponding percentage changes over time were computed for the following structures: whole brain volume and grey matter, lateral ventricles, thalamus, the limbic lobe including the anterior, middle and posterior cingulate gyrus, basal ganglia (BG) including the nucleus accumbens, pallidum, putamen and caudate nucleus, and medial temporal lobe including the amygdala, hippocampus and parahippocampus. Details are given in Appendix SII.
Secondary outcomes
Clinical assessment and blood sampling. Clinical assessment at baseline and follow-up were performed by an experienced rater. Each assessment involved a neurological evaluation, including the EDSS rating.
A Timed 25-foot Walk Test (T25FWT) was performed to assess walking speed. The T25FWT correlates with disability and lower extremity function and has a strong reliability over both brief and long time-periods across a wide range of disability levels in pwMS. To capture treatment effects, a > 20% change in T25FWT is considered clinically meaningful (20).
Blood samples were collected in the morning from the antecubital vein while participants were in a resting state. Blood samples were centrifuged at 2,500 g for 5 min and the supernatant was stored at –20˚C until analysis.
Serum concentrations of soluble interleukin-2 receptor (sIL2R), interleukin-6 (IL6) and brain-derived neurotrophic factor (BDNF) were analysed using commercially available enzyme-linked immunosorbent assay (ELISA) kits for measurement of concentration of sIL2R and BDNF (R&D Systems, MN, USA) and IL-6 (Thermo Fisher Scientific, Waltham, MA, USA) according to the manufacturer’s instructions.
Cognitive testing. A standard battery of neuropsychological tests (Brief International Cognitive Assessment for MS; BICAMS (21)) was used to evaluate the psychomotor speed and attention, memory and executive function of the study participants. The battery consists of California Verbal Learning Test (CVLT-II), Symbol Digit Modalities Test (SDMT) and Brief Visual Memory Test (BVMT-R). Test application lasted approximately 15 min per participant. Details are given in Appendix SIII.
Patient-reported outcomes. To assess the levels of activities of daily living, as well as recreational and sport activities, and abilities, the Human Activities Profile (HAP) test (22) was used. The HAP test is a self-report questionnaire consisting of a sequence of 94 questions, ordered by progressively increasing estimated metabolic equivalent (MET) level. The HAP test yields 2 scores: maximum activity score (MAS) and adjusted activity score (AAS), with higher scores indicating higher levels of function. The former corresponds to the highest MET level activity a respondent can perform, while the latter reflects their mean activity level on a daily basis (22). Both MAS and AAS range from 1 to 94, reflecting activities requiring between approximately 1 and 10 MET, and score changes of 7.8 and 6.8 for MAS and AAS, respectively, are considered clinically significant (23).
Fatigue was assessed using the Modified Fatigue Impact Scale (MFIS), which captures the impact of fatigue on patient’s physical, cognitive and psychosocial functioning. MFIS has a score range of 0–84, with lower scores indicating less fatigue. Although widely used as a self-report measure of fatigue in patients with MS, a clinically relevant change has not yet been determined (24).
Beck Depression Inventory II (BDI-II) was used to test for depression, which can be a potential confounding factor when assessing MS-related fatigue (24). The maximum score on BDI-II is 63, with higher scores indicating more severe depressive symptoms and scores < 10 indicating no or minimal depression (25).
To assess patient’s health-related QoL (HRQoL) in multiple aspects, the Multiple Sclerosis Quality of Life-54 (MSQoL-54), a validated MS-specific instrument, was used (26). MSQoL-54 comprises 12 subscales and 2 single-item measures, and the subscales are summarized into 2 summary composite scores, i.e. Physical Health Composite (PHC) and Mental Health Composite (MHC). Scores on all scales range from a minimum of 0 to a maximum of 100, with higher scores indicating higher QoL.
Statistical analysis
This study focused primarily on the assessment of MRI-derived neurodegeneration; therefore, the sample size calculation was based on data regarding brain volume loss in pwMS, existing at the time of study design (i.e. 2015). With expected –0.40% brain volume loss in pwMS annually (control group assumption) and –0.20% in healthy adults (age 35 years), MRI-derived brain volume loss variability of 0.13% (27, 28), and a 2-tailed significance level of 5%, power 90% and dropout 10%, the minimal sample size was n = 11. Descriptive statistics were calculated to describe IG and CG groups in terms of baseline demographics, disease and treatment characteristics and clinical outcome scores. Cognitive test results were compared with corresponding age-matched norms for healthy subjects, and the predicted Z scores based on education level were calculated (29).
Linear mixed-effects models were used to estimate all outcomes: (i) adjusted least-squares means at baseline, (ii) least-squares means at follow-up; and (iii) treatment effect at follow-up. Group, EDSS at baseline, and baseline outcome value (except with MRI outcomes, which were inherently longitudinal) were modelled as fixed effects. Differences in the time window between baseline and follow-up outcome assessments (i.e. clinical, MRI, PRO, cytokine and cognitive testing) were modelled as random effects.
A complete case analysis was used with no imputations of missing data. For all estimates, bootstrap means and 95% confidence intervals (95% CIs) were calculated and reported. Statistical analysis was performed in R, version 3.4.0 (RStudio, v1.0.143; RStudio, Inc., 250 Northern Ave, Boston, MA 02210, USA).
Interpretation of the results was based on observing the effect size and direction and the confidence intervals (CIs). The effect was considered strong if the mean differences between groups at 3-month follow were large in magnitude and if the corresponding CI excluded the zero value, i.e. was occupied either on the positive or negative range. On the other hand, the effect was negligible if the effect magnitude was small and the CI symmetrically distributed around the zero value.
Patients
A total of 88 patients were screened for eligibility, of whom 60 were excluded because they met the exclusion criteria or declined to participate (Fig. 1). In total, 28 patients were included and randomized into IG (n = 14) and CG (n = 14). None of the patients were involved in prior regular exercise and none required physiotherapy during the study. Two female patients, one from each group, required pulsed intravenous corticosteroid therapy during the intervention period due to disease relapse and, afterwards, continued with the study as per the allocated plan.
Missing data, the number of dropouts and reasons for dropping out were somewhat unequally distributed between groups (Fig. 1); 1 patient in the IG group withdrew due to failure to comply with the training schedule, one patient from each group was excluded due to discontinuation of fingolimod (unrelated to disease activity). All remaining patients attended the follow-up MRI and clinical assessment and completed PROs; however, 1 patient in the IG did not attend the follow-up neuropsychological assessment.
Descriptive baseline characteristics for the IG and CG groups are reported in Table I.
Table I. Baseline characteristics
Primary outcome: magnetic resonance imaging
Changes in MRI measures of lesion volumes and counts and (regional) brain volumes between baseline and follow-up scans are shown in Table II. In general, the effects of AE on whole-brain and GM atrophy, and on atrophy of most selected substructures of the brain were negligible. The study found an effect of AE on some of the structures analysed (amygdala, putamen, posterior cingulate gyrus (PCG), parahippocampal gyrus (PHG) and thalamus), but the directions of the effect varied between the structures studied. AE was strongly associated with a reduction in putaminal volume and PCG volume. AE was strongly associated with an increase in PHG volume and had a preservation effect on thalamus and amygdala volume.
A decrease in active lesion count and load were also observed.
Secondary outcomes
Changes in clinical outcomes, cognitive outcomes and PROs, and cytokine levels between baseline and follow-up assessments in the IG and CG groups are reported in Table III. At follow-up, the EDSS was slightly reduced in the IG and there was also a weak effect of AE on walking speed, measured by T25FWT. No effects of AE on cognitive outcomes and PROs were observed, apart from a few negative effects seen among individual scores of MSQoL-54 (see Appendix SIV, Table SII). The analysis suggests a deteriorating effect on social functioning and a small negative impact of AE on energy levels in IG participants. However, the latter was not confirmed by MFIS results, which showed no effect. Although the levels of tIL2R and IL6 remained unchanged, a weak association was found between AE and increase in BDNF.
The immediate effect of AE in the IG was an increase in cardiorespiratory fitness, assessed using a step test. However, several IG participants (9/14) were unable to perform pre- and post-measurements due to organizational reasons, leading to incomplete measurements that were thus discarded from the analysis. The discarding had no effect on the rest of the results.
Table II. Estimated mean magnetic resonance imaging outcomes
Table III. Estimated mean clinical, cognitive and patient-reported outcomes
To our best knowledge, this is the first RCT investigating the impact of 12 weeks of AE in combination with fingolimod treatment on disease course in MS. The study primarily focused on MRI biomarkers of disease activity and neurodegeneration. The effect of AE on whole-brain and GM atrophy was minor; however, strong effects on particular brain structures were observed with rather heterogeneous effect directions. For instance, AE was associated with a decrease in putaminal and PCG volumes, while an increase in PHG volume and preservation of thalamus and amygdala volumes were observed. MRI also indicated a decrease in active lesion count and load. Among the secondary outcomes, walking speed and BDNF levels improved slightly in the IG, while other clinical, cognitive or PRO measures did not appear to have been affected by the AE.
Study groups were well matched with regards to baseline demographics. The range of baseline functional impairment was quite broad (EDSS 1.0–6.5), which, together with somewhat long mean disease duration, suggests that both study groups were already bordering on secondary progression. The reason is that, at the time of the study, fingolimod was used mainly as a second/third-line drug for MS. However, these patients had documented clinical or radiological disease activity and were all classified by their neurologists as relapsing-remitting MS.
Differences between study groups may arise despite random assignment and it is difficult to adequately control for such differences in the statistical analysis. For example, a difference was observed in baseline levels of BDNF (Table II). Study patients were not involved in regular exercise prior to the study start, and their mean baseline AAS score was lower than that of the general population (22). This is in line with previous reports of lower levels of physical activity in pwMS (9). Since physical activity has been shown to increase the expression of BDNF (30), the higher mean baseline BDNF in IG patients could indicate a higher level of physical fitness. However, the observed difference from the CG in mean baseline BDNF was approximately 10%, whereas differences > 30% are considered significant (31). At 3 months follow-up the respective mean BDNFs were at slightly higher levels than at baseline, but with similar relative difference. Therefore, the baseline differences in BDNF levels are considered not to have a major impact on other outcomes.
The primary outcomes of this study were MRI results indicating a decrease in active lesion load and count with a stable T2 lesion load, suggesting a possible anti-inflammatory effect of AE. No impact on whole-brain atrophy or GM atrophy was observed, probably due to the short observation window. The study also examined regional atrophy, for example, in the thalamus and BG and the temporal and limbic lobes due to their involvement in memory, cognition, emotion, behaviour and ambulatory capacity (11, 12, 32, 33). AE had rather heterogeneous directions of effect on brain structures in this study. A decrease in putaminal and PCG volumes was observed after AE, whereas, for the most of the BG and other selected structures in the temporal and limbic lobes, no effect of AE on associated volume or atrophy was observed. A stabilizing effect of AE on thalamus and amygdala volume and an increase in PHG volume were observed. Previous studies on the impact of exercise, both on elderly adults (34) and pwMS (11, 13, 14), focused primarily on the hippocampal area, showing a positive impact of exercise or aerobic capacity on hippocampal volume, but, to our best knowledge, there are no reports on the impact on PHG or amygdala volume in either patient population. The PHG is involved in the default-mode cortical network (DMN), which has been implicated in episodic memory function and appears particularly vulnerable to the detrimental effects of ageing and Alzheimer’s disease (35). The structural integrity and volume of the amygdala are correlated with experience of cognitive fatigue and impairment of social cognition in pwMS (36, 37). The current findings suggest a positive effect of AE on a DMN component, and a preserving effect on amygdala and thalamus volume in pwMS; however, the clinical implications of these findings remain unclear, since no correlating impact on cognitive outcomes or PROs was observed.
After 12 weeks of AE, the consistently lower T25FWT observed in the IG indicates mobility improvement, and the EDSS also reduced by –0.31 (–0.84, 0.22). This result seems promising, given that the EDSS is rather insensitive to change, especially over a short intervention period of 12 weeks. Furthermore, the current study participants had a wide range of functional impairment, while a recent RCT (38) suggests that the effects of exercise in pwMS with substantial mobility disability predominantly affect walking endurance over walking speed, as measured by T25FWT. Patients with moderate to substantial mobility disability may be less prone to the positive effects of exercise on cognitive processing speed (CPS) (8, 19). The current study population’s mean EDSS score suggests a moderate walking impairment. This could explain why the current study did not observe a more substantial change in walking speed or cognitive performance.
The AE intervention did not exhibit an effect on resting cytokine levels in pwMS. Regular exercise is known to temporarily increase BDNF levels and supposedly mediates the effect of exercise on cognition (39), but there is a small effect on resting- state BDNF levels (30). Fingolimod could be a confounding factor, as it has been shown to increase BDNF levels (40). Nevertheless, we replicated the results of previous studies (41, 42), which showed no exercise-induced changes in resting levels of Th-1-, Th-2- or Th-17-associated cytokines. BDNF polymorphism, while not assessed in the current study, modulates the effect of physical exercise on neuroplasticity (30) and was implicated in preservation of GM volume and CPS in pwMS (43), therefore it could have contributed to the MRI results in the current study.
Review studies (8) highlight inconsistent findings regarding the effect of exercise on mood and HRQoL in pwMS. In the current study, the MSQoL-54 results indicate deterioration in social functioning and possible reduction in energy levels in the IG, which was not corroborated by the MFIS results. A certain level of negative social interactions was observed among the IG participants during the study, possibly contributing to the decrease in certain HRQoL scores. Namely, some IG participants reported perceived peer-pressure during AE, mainly related to the level of their (dis)ability. Secondly, some IG participants reported a high organizational burden of incorporating exercise into their daily schedule and committing to regular visits. Instead of fitting into the physical HRQoL dimension of the MSQoL-54, in the Slovenian population the energy subscale fits more into the mental dimension (26), which could explain the observed reduction in energy level.
Study limitations
This exploratory study has several limitations. The generalizability of the results may be limited by the included participants being pwMS who were willing to participate in a 12-week RCT study, and, to avoid potential DMD-related confound, were being treated with fingolimod. An important limitation of this study is the small sample size (n = 28, 14 per group), increasing the risk of type II error. The prior sample size calculation, based on MRI-derived brain volume change data from the research literature existing at the time when the study was conceived, indicated an optimal sample size of 11 per group. However, a revised sample size calculation (27, 28) indicates that a higher number of participants, at least 24 or more per group would be required. The number is probably even higher according to the observed confidence intervals of lesion and brain structure changes in Table II, possibly owing to the impact of various confounding factors, such as hydration, ageing, etc. (44). Furthermore, the study duration was relatively short and does not allow us to detect major changes.
Future research
Future studies of longer duration and larger sample size with inclusion of other DMDs are needed to either confirm or refute these findings and further elucidate the role of AE as an adjunctive treatment option to pharmacological intervention in the management of pwMS. Furthermore, to reduce the organizational burden for the participants, a community- or teleconference-based exercise intervention could prove more beneficial in this regard and would allow changes to be observed over a longer time-window. To avoid ethical dilemmas about not including the control group in an activity that is considered beneficial, a cross-over study would be preferred.
Conclusion
The results of this exploratory study on the impact of AE in pwMS treated with fingolimod show a positive effect of AE on the preservation of several regional brain volumes, possibly indicating a slowing of the neurodegenerative process in pwMS. Whether the observed slight decrease in active lesion load and count in addition to a stable T2 lesion load could suggest a possible anti-inflammatory effect of AE remains to be determined by further studies.
The authors would like to thank Anita Pirečnik Noč, Nives Matko and Andreja Emeršič for their help with blood sample collection and preparation of samples for further analysis.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Funding and declarations of interest
LS reports personal fees (speaker honoraria and travel expenses) from Merck, Novartis, Teva, Biogen, Sanofi-Genzyme, Krka, Lek, Roche, Bayer, Boehringer-Ingelheim and Pfizer, outside the submitted work.
VS reports grant from the Slovenian Research Agency Project group number P5-0142, during the conduct of the study.
ŽŠ reports grant from the Slovenian Research Agency Project group numbers J7-6781 and J2-2500, and personal fees (speaker honoraria) from Biogen, Novartis and Sanofi-Genzyme, all outside the submitted work.
SŠJ reports personal fees (speaker honoraria and travel expenses) from Merck, Novartis, Teva, Biogen, Sanofi-Genzyme, Roche and Bayer, outside the submitted work.


 Click to show fullsize
Click to show fullsize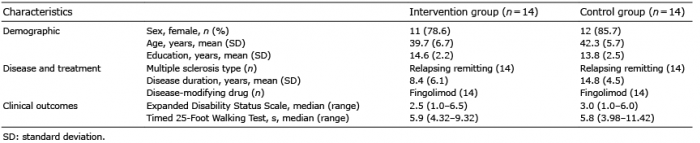 Click to show fullsize
Click to show fullsize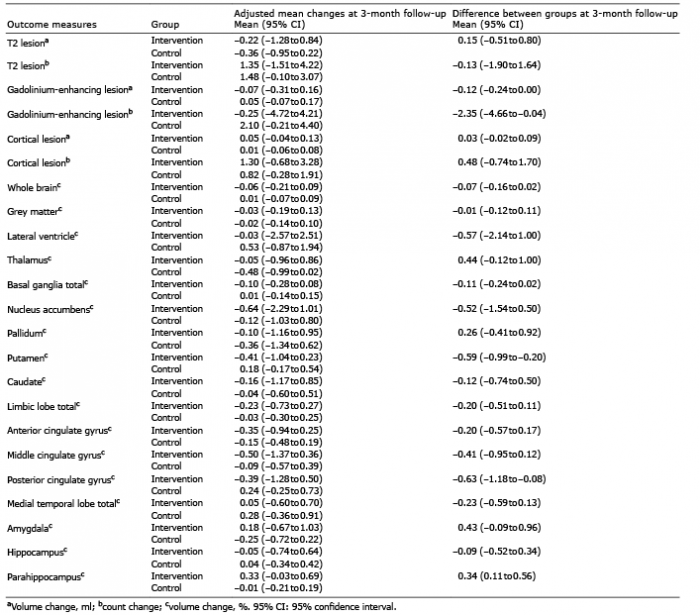 Click to show fullsize
Click to show fullsize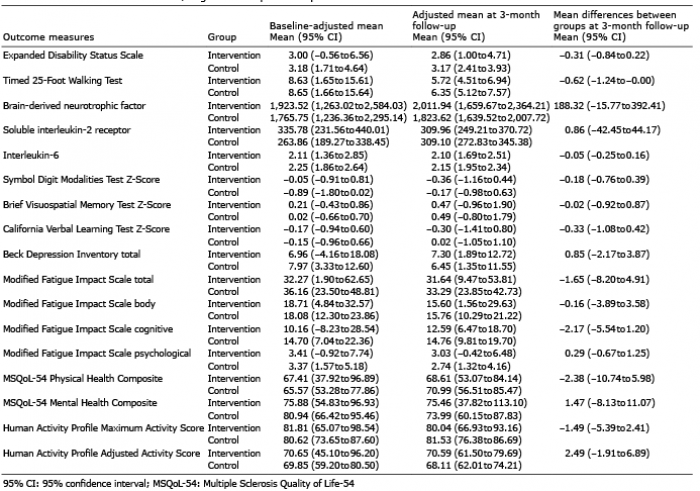 Click to show fullsize
Click to show fullsize