
From the 1Department of Geriatric Medicine, Oslo University Hospital, 2Institute of Clinical Medicine, University of Oslo, Oslo, 3Department of Internal Medicine, Bærum Hospital, Vestre Viken, 4Department of Neurology, Oslo University Hospital, 5Department of Physiotherapy, Oslo University Hospital, Oslo, Norway, 6Department of Internal Medicine, Central Hospital, 7Department of Neurology, Central Hospital, Karlstad, and 8School of Medical Sciences, Örebro University, Örebro, Sweden
Objective: To evaluate the prevalence of cognitive and emotional impairments one year after first-ever mild stroke in younger patients.
Design: Prospective, observational, cohort study.
Subjects: A consecutive sample of 117 previously cognitively healthy patients aged 18–70 years with mild stroke (National Institutes of Health Stroke Scale score ≤ 3) were included in 2 hospitals in Norway during a 2-year period.
Methods: At 12-month follow-up, patients were assessed using validated instruments for essential cognitive domains, fatigue, depression, anxiety, apathy and pathological laughter and crying.
Results: In total, 78 patients (67%) had difficulty with one or a combination of the cognitive domains psychomotor speed, attention, executive and visuospatial function, and memory. Furthermore, 50 patients (43%) had impairment in either one or a combination of the emotional measures for anxiety, depressive symptoms, fatigue, apathy or emotional lability. A total of 32 patients (28%) had both cognitive and emotional impairments. Only 21 patients (18%) scored within the reference range in all the cognitive and emotional tools.
Conclusion: Hidden impairments are common after first-ever mild stroke in younger patients. Stroke physicians should screen for hidden impairments using appropriate tools.
Key words: mild stroke; younger patients; cognitive impairment; depression; anxiety; apathy; fatigue; hidden impairments.
Accepted Oct 13, 2020; Epub ahead of print Nov 4, 2020
J Rehabil Med 2021; 53: jrm00135
Correspondence address: Georgios Vlachos, Georgios Vlachos, MD, Stroke Unit, Department of Neurology, Oslo University Hospital, Postbox 4956 Nydalen, 0424 Oslo, Norway. E-mail: georgios.vlachos@ous-hf.no
Doi: 10.2340/16501977-2764
Many patients with minimal or no apparent neurological deficits after stroke may experience cognitive and emotion-al symptoms. The quality of life and functioning of these patients may be reduced. Our research group studied 117 previously cognitively healthy patients aged 70 years or younger with mild stroke 12 months after the stroke event. They were assessed for cognitive and emotional impairments using validated tests for cognitive function, fatigue, depression, anxiety, and apathy. Only 21 patients (18%) scored within the normal range in these tests. In conclusion, “hidden impairments” are common among younger stroke patients. It is important for patients, their surroundi-ngs and stroke physicians to be aware that such difficulties can occur after even a mild stroke.
Outcome after stroke has improved remarkably over recent years due to better prevention and improved acute treatments in the stroke units (1) and by reperfusion therapy (2).
Still, independently of age and lesion size, cognitive and emotional impairments after stroke are common, with a prevalence of dementia of up to 20% and of mild cognitive impairment (MCI) of 38% in a general stroke sample one year after onset of symptoms (3), and a prevalence of depression and anxiety reaching 30% and 20–25%, respectively (4). However, the number of cognitive and emotional impairments detected after stroke vary due to heterogeneity in the cognitive instruments, used diagnostic criteria and demographic factors, such as educational level, vascular risk factors and comorbid-ity. Since even first-ever stroke can lead to cognitive deficits in patients who are previously cognitively intact, it has been suggested that future research on post-stroke cognitive deficits should focus on this patient group (5).
Persons with minimal neurological deficits after stroke are often discharged shortly after admittance, with the observation that “everything seems to be alright”. However, on return to their everyday lives, they may realize that their quality of life and functioning has changed. These patients may face difficulties affecting their memory, concentration, attention, and commonly experience fatigue (6). Pendlebury et al. (7) showed that, in a sample of patient with minor stroke, 8.2% were diagnosed with dementia one year after stroke, which was significantly higher than for an age-matched general population. Emotional impairments, such as anxiety, depression and apathy, can also occur (6, 8). It has been suggested that younger persons are at particular risk of developing dis-abling cognitive and emotional impairments after stroke (9).
As a consequence, patients with stroke, stroke patients’ organizations, and health professionals have introduced the concept of “hidden impairments” (10). The syndrome of hidden impairments is proposed to include cognitive and emotional impairments that are not revealed through neurological examination or cognitive and emotional screening instruments used in clinical daily routine (10). Hidden impairments may include executive dysfunction, memory impairment, language difficulties, reduced psychomotor speed, fatigue, pathological laughter and crying, anxiety, depression, and apathy. The aim of this prospective, observational, cohort study was to evaluate the prevalence of hidden impairments 12 months after first-ever mild stroke in patients aged 70 years or younger.
Population
From December 2014 until December 2016, patients with first-ever ischaemic or haemorrhagic stroke admitted to the acute stroke units of Oslo University Hospital and Bærum Hospital were consecutively included in the study. Inclusion criteria were: patients aged 18–70 years, who had had mild strokes, defined as a National Institutes of Health Stroke Scale (NIHSS) (11) score ≤3 at discharge (12).
Patients with pre-stroke cognitive decline as indicated by a score > 3.2 on the short form of the Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE) (13), patients who did not speak Norwegian, and patients with known psychiatric disease were not eligible for inclusion. Patients who experienced a new stroke during the first year after discharge from the stroke unit were not invited to follow-up.
Diagnostic evaluation
The diagnosis of stroke was based on the history of symptoms, the findings on the neurological examination, and the findings of an acute infarction or haemorrhage on cerebral computed tomography (CT) or magnetic resonance imaging (MRI) scans. Patients with no acute haemorrhagic or ischaemic lesions on CT or MRI, but with neurological deficits compatible with cerebrovascular disease lasting more than 24 h, were considered to have an ischaemic stroke (14).
Ischaemic strokes were classified according to the Trial of ORG 10172 in Acute Stroke Treatment (TOAST) (15), and the Oxfordshire Community Stroke Project (OCSP) classifications (16).
Assessments
Vascular risk factors, including hypertension, hyperlipidaemia, coronary heart disease, atrial fibrillation, cigarette smoking and diabetes mellitus, were recorded, and body mass index (BMI) calculated. A diagnosis of atrial fibrillation required electrocardiogram (ECG) confirmation pre-stroke or during the hospital stay.
Neurological impairments were assessed with the NIHSS (11) at admission and discharge by a stroke physician or a stroke nurse. Patients were screened for pre-stroke cognitive impairment with the 16-question version of the IQCODE (13), which was completed by first-degree relatives or another next-of-kin. Due to the younger age and high educational level of included patients, a cut-off of 3.2 was used to minimize the probability of including patients with a pre-stroke cognitive impairment. Patients who had previously been diagnosed with dementia or mild cognitive impairment were not included.
Activities of daily living (ADL) were assessed with the Barthel ADL index (17) and general functional level with the modified Rankin Scale score (mRS) (17) at discharge and at 12-month follow-up.
All participants were invited to a 12-month follow-up at the Stroke Outpatient Clinic. The duration of the sessions was at most 2 h. Pauses during the tests were allowed if needed. The cognitive and emotional assessments were performed by either stroke physicians (authors GV and HI-H), occupational therapists, or by a nurse in the stroke units and the stroke outpatient clinics. The professionals carrying out the tests had been trained by physicians with wide experience in that field. The choice of the cut-offs was discussed with neuropsychologists.
Cognitive and emotional assessment
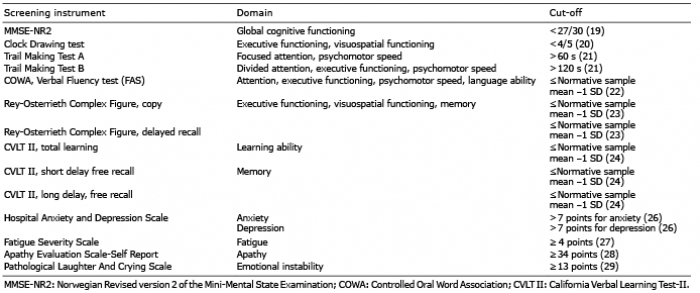
At the 12-month follow-up cognitive and emotional domains were evaluated using the tests shown in Table I.
Table I. Used tests, domains tested, and cut-off values at the 12-month follow-up
The Mini Mental State Examination Norwegian Revision 2 (MMSE NR2) (18) is a global screening test of cognitive functioning. Optimal cut-off values vary with age and educational level. A relatively high score (< 27 points) was chosen as a cut-off, since most patients were younger than 70 years and well educated (19).
The Clock Drawing test (20) is sensitive for visuospatial and executive functions. Patients who scored < 4/5 points in the Clock Drawing test were considered cognitively impaired.
The Trail Making Tests (TMT) A and B (21) were used to assess psychomotor speed and focused or divided attention. In addition, TMT B is sensitive for executive functioning. A cut-off between normal and pathological functioning was chosen as correct administration of the TMT A within 60 s, and the TMT B within 120 s. The TMT B was interrupted after 5 min (300 s) if the participant was not able to complete it during that time.
The Controlled Oral Word Association (COWA) Verbal Fluency test (22) evaluates language ability, psychomotor speed, attention and executive functioning. Patients name as many words beginning with letters F, A, S as possible within one min for each letter.
The Rey-Osterrieth Complex Figure Test (ROCF) (23) requires subjects to copy a complex figure, and then reproduce it after 20 min. This tests memory as well as visuospatial and executive functions.
For assessment of learning ability and memory, the California Verbal Learning Test II (CVLT II) (24) was used where patients try to learn a 16-word list, and to recall it after 20 min.
Due to the evidence for age-related and, in some tests, sex-related differences on cognitive test scores, raw scores were converted into standardized scores (mean 50; standard deviation (SD) 10) separately for each sex and age category for CVLT II, for age for ROCF, and for age and education level for COWA and the Trail Making tests. Impairment of each cognitive domain was defined as a score of at least 1 SD below appropriate normative sample according to the test manuals used at The Memory Clinic of the Department of Geriatric Medicine at Oslo University Hospital. According to the International Society for Vascular Behavioral and Cognitive Disorders (VASCOG) criteria (25) for the diagnosis of cognitive impairment, mild cognitive disorder can be present when the performance on objective validated cognitive tools in one or more cognitive domains (attention, processing speed, executive function, learning and memory, language, visuocontructional-perceptual ability, praxis-gnosis-body schema, social cognition) is in the range 1–2 SD below appropriate norms. A cut-off of –1 SD below appropriate norms was chosen due to the patients’ younger age (≤70 years) and high educational level.
The presence of anxiety and depression symptoms was evaluated with the 14-item Hospital Anxiety and Depression Scale (HADS) (26). The cut-off was > 7 points for each of the 2 domains depression and anxiety.
Post-stroke fatigue (PSF) was defined as the well-established cut-off of ≥ 4 points on the 9-item Fatigue Severity Scale (FSS) (27), which is a widely used instrument in stroke studies.
The 18-item Apathy Evaluation Scale-Self report (AES-S) (28) was used to assess the presence and severity of post-stroke apathy (PSA). Patients with a score ≥ 34 points were classified as having clinically relevant apathy.
The Pathological Laughter and Crying Scale (PLACS) (29) was used to assess the presence of emotional lability, character-ized as uncontrolled laughter or crying in appropriate situations. The cut-off was ≥ 13 points.
Cognitive impairment was considered to be present whenever a patient had a score outside the reference range on at least one of the cognitive tests, and an emotional impairment whenever a patient scored outside the reference range on at least one emotional instrument.
Statistical analysis
Statistical analyses were performed with the Statistical Package for Social Sciences (SPSS), version 25.0, using descriptive statistics. Data are presented with means and SD for continuous variables, and with proportions and percentages for categorical variables. The rating scale scores are represented with median, where the data distribution was skewed, and range.
Ethics
The study was approved by the Regional Committee for Ethics in Medical Research (register number 2014/1268), and by the Hospital’s Data Protection Authority. All patients gave their written informed consent before inclusion.
In total, 127 patients with first-ever ischaemic or haemorrhagic stroke admitted to the acute stroke units of Oslo University Hospital (99 patients) or Bærum Hospital (28 patients), were included. Mean age was 55.7 years (SD 11.3; range 30–70 years), and 98 (77%) were male. Of the included patients, 119 (94%) had an ischaemic and 8 (6%) had a haemorrhagic stroke. Mean education length was 15.3 years (SD 3.6 years). One included patient had expressive aphasia at discharge diagnosed by a speech therapist.
The clinical characteristics of all patients at admission are shown in Table II.
Table II. Baseline characteristics of all patients
12-month follow-up: cognitive and emotional assessments
At the 12-month follow-up, 117 patients (92%) were available. During the first post-stroke year, 4 patients had a new stroke and were not invited to the follow-up, one patient died from cardiac disease and 5 patients did not wish to complete the follow-up period.
Table III shows the results of the cognitive and the emotional instruments used at 12-month follow-up.
Table III. Cognitive and emotional functioning 12 months after stroke.
Cognitive assessments
On the MMSE, the Clock Drawing test and the TMT A, most patients scored within the normal range, whereas on the TMT B, 11% of male and 8% of female patients had a score > 120 s. Applying a strict cut-off of ≤ –1SD below the appropriate norms, 43% of male and 30% of female patients had a score below cut-off on the COWA Verbal Fluency test. For the ROCF delayed recall, 31% of male and 22% of female patients scored below a cut-off of ≤ –1SD.
In total, only 33% of the patients scored within the reference range on all tests; the remaining patients had scores outside the reference range on 1–8 tests (see Fig. 1). This means that, according to the VASCOG criteria (25), 67% of patients 70 years and younger at stroke onset, might have a cognitive impairment 12 months after first-ever mild stroke.
Fig. 1. Distribution of patients with cognitive test results outside reference range 12 months after stroke.
Emotional assessments
A total of 18 patients (15%) had a high score on the anxiety scale, and 15 patients (13%) on the depression scale. A total of 15 patients (13%) had an elevated score for the combined anxiety-depression scale. The prevalence of anxiety was 30% for women and 11% for men, while 22% of women and 10% of men had symptoms of depression. Analyses of FSS showed that 38 patients (33%) reported elevated scores. The prevalence among women was 56%, while it was 26% among men. Furthermore, 29 patients (25%) had a score ≥ 34 points on AES-S. Concerning pathological laughter and crying tested by the PLACS, the prevalence of a score above cut-off for women was 11%, while it was low for men (1%) as well as for the whole sample (3%).
In total, 43% had a score outside the reference range on at least one emotional instrument (see Fig. 2).
As illustrated in Fig. 3, 18% of the total sample had neither cognitive nor emotional deficits that were detectable with the instruments used at one year after stroke. At 12-month follow-up 39% of the sample had only cognitive deficits, 15% had only emotional deficits, while 28% had both cognitive and emotional deficits.
Fig. 2. Distribution of patients with emotional test results outside reference range 12 months after stroke.
Fig. 3. Frequency of cognitive and emotional impairments 12 months after stroke.
This study indicates that one year after stroke, approximately 2 out of 3 patients aged 30–70 years, and with mild neurological symptoms may have difficulties with cognitive functions, such as psychomotor speed, attention, executive function, visuospatial function or memory, either alone or in combination with each other. Nearly every second patient may have impairment in either one or a combination of the emotional domains anxiety, depressive symptoms, fatigue, apathy, or emotional lability. Only one out of 5 could be considered as not having any cognitive or emotional impairments that were detectable with our instruments 12 months after stroke. This is in line with our clinical experience from the stroke outpatient clinic, based on the cognitive and emotional symptoms patients report at routine follow-up during the first year after stroke.
As also reported by others (10), this study found that the MMSE was insensitive to detect impairment of global cognitive functioning in patients with mild neurological impairments, despite the fact that a high cut-off (< 27/30) was used. We assume that this result is related to the younger age and high educational level of our patients (19). In addition, the MMSE does not capture executive functioning or psychomotor speed at all (30). More sensitive tests, such as the Clock Drawing Test, the TMT A and B, the ROCF, the Verbal Fluency test and the CVLT II, are necessary in order to evaluate cognitive domains, such as executive and visuospatial functioning, psychomotor speed, attention, memory, and learning and language ability. The test results indicate that psychomotor speed, attention, executive functioning, visuospatial function, language ability, and memory were affected in both sexes, while the prevalence of impaired learning ability was higher in women. There were more men who took over 120 s to administer the TMT B. Just one patient took over 60 s to administer the TMT A. We believe that this was due to the young age and high educational level of the included patients. MMSE was used as this was the standard cognitive tool at the 2 study sites during the study period. However, due to its wider spectre of covered domains we now recommend the Montreal Cognitive Assessment (MoCA) (31) for post-stroke follow-up, both in clinical and research settings.
Other studies (32) have shown a 12-month prevalence of depression of up to 36%. The prevalence of symptoms of anxiety and depression in the current sample was lower, probably due to low presence of known risk factors, such as diabetes, female sex and severe stroke (32). Fatigue is a common hidden impairment after stroke and the one-year prevalence in previous studies has been reported to be 30–60% (27). In the current study, the prevalence of FSS score ≥ 4 points was 33% for the whole sample. Likewise, 25% of all patients reported symptoms of apathy. This is similar to rates reported in other studies (33).
The concept of cognitive domains may be challenging, since domains often interact and overlap. Cognitive tests are most often sensitive to alterations in more than one cognitive domain, e.g. the Clock Drawing test, which assesses both visuospatial ability and executive function-ing, or the verbal fluency tests that evaluate language abilities, executive functioning and processing speed (34). Executive functioning is, by definition, thought to involve multiple cognitive domains in a hierarchical manner, where intact executive functions “control” other cognitive abilities. Still, in order to conceptualize cognitive functioning through cognitive assessment in clinical practice, test results, in a diagnostic process, need to be translated into cognitive domains. The 5th edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) criteria supports the assessment of different cognitive domains, but with no strict recommendation for preferred tests (35). Although the validity of cognitive domains may be questioned, we have chosen to relate cognitive tests to cognitive domains in accordance with clinical practice (34).
During the last decade it has been discussed whether the presence of depression may enhance or even cause cognitive impairment (36). Conversely, cognitive impairment seems to be associated with emotional symptoms (37). The current study found that 28% of patients had a combination of both cognitive and emotional symptoms one year after stroke.
A stroke can change the life of patients in several ways; physically, cognitively and emotionally (9). In clinical practice, an exact diagnosis of specific symptoms may be difficult to establish, since cognitive and emotional symptoms often overlap. A feeling of general “slowness” after stroke may, for instance, be caused by executive dysfunction, fatigue, apathy, or depression, either isolated or in combination. It may be difficult, or in many cases even irrelevant, to distinguish the different cognitive and emotional symptoms from each other, since the patients’ most important experience and complaint often is a “feeling of being different” from their premorbid state.
Some of the study patients who completed the 12-month follow-up reported memory, attention and concentration difficulties, which led to bad mood, tiredness, and exhaustion. On the other hand, some patients reported that fatigue also resulted in such difficulties. Almost all patients who completed the 12-month follow-up were free of obvious focal neurological deficits, and their functional level according to the mRS and Barthel Index was high. Cognitive and emotional deficits were not visible, or, in other words, they were hidden for the patients’ surroundings. One in 3 patients had both cognitive and emotional impairments at the same time one year after stroke. Since it is difficult to determine the order of their appearance, we consider that such deficits have to be seen, not only separately, but also as an entity. Like other authors (10), we consider the concept of the “syndrome of hidden impairments” is the best way to define the combination of these invisible stroke sequelae.
Today, very few stroke units and outpatient clinics utilize diagnostic, therapeutic or rehabilitation options for patients with mild or no visible impairments after stroke. It is likely that future stroke units will need to broaden the focus, and acquire competence that is relevant even for patients with mild impairments (38).
Study limitations and strengths
One of the inclusion criteria for this study was that patients should be cognitively healthy pre-stroke. This information was obtained through asking patients, their dependents, and their family doctors, or by reviewing patients’ hospital medical records. Thereby, a possible under-reporting of cognitive symptoms before stroke might bias the results. We therefore chose to screen cognitive function in all the stroke patients 70 years or younger admitted to our 2 stroke units by asking their dependents to complete the 16-item IQCODE. A limitation is that this questionnaire is validated for an elderly population (13).
Strengths of the present study are the consecutive inclusion of patients with a clear diagnosis of a first-ever stroke and the application of an extensive battery of instruments covering relevant cognitive and emotional domains. The choice of such a wide panel of cognitive tests was eligible for diagnosing mild cognitive disorder due to the VASCOG criteria (25). By choosing a cut-off of –1 SD below appropriate norms, and without correction for multiple tests, mild cognitive disorders might have been overdiagnosed in some cases.
Three out of 4 study participants were male. This high proportion of male patients is in accordance with known stroke epidemiology (39). The research team evaluated all the patients aged 18–70 years admitted to the 2 stroke units during the inclusion period. Only 2 patients did not wish to participate. Another strength of the study is the low attrition bias, since only 5 of the included patients declined to complete the follow-up period.
In conclusion, younger patients with stroke, but without obvious neurological symptoms and findings, frequently have hidden impairments, such as subtle cognitive decline, fatigue, and emotional symptoms one year after first-ever stroke. It is important to offer an eval-uation of their cognitive and emotional status by using a wide screening battery up to 12 months after stroke. The focus on patients with mild impairments needs to be strengthened in stroke units and stroke outpatient clinics. Further studies should focus on identifying cognitive and emotional instruments to use in the clinical routine follow-up of these patients, and how such identified impairments may affect patients’ social and family life
The authors thank the patients who participated in the study. In addition, we thank the physicians, nurses, physiotherapists and occupational therapists in the stroke units and the stroke outpatient clinics at Oslo University Hospital and Bærum Hospital for their contribution in selecting, examining, and following up the included patients. Occupational therapists Elisabeth Kjelgaard, Sonja Aune, Karla Ascencio (Oslo University Hospital) and nurse Anne-Mette Brenden (Bærum Hospital) contributed by performing cognitive and emotional assessments. Sources of funding. Department of Geriatric Medicine, Oslo University Hospital.
The authors have no conflict of interests to declare.


 Click to show fullsize
Click to show fullsize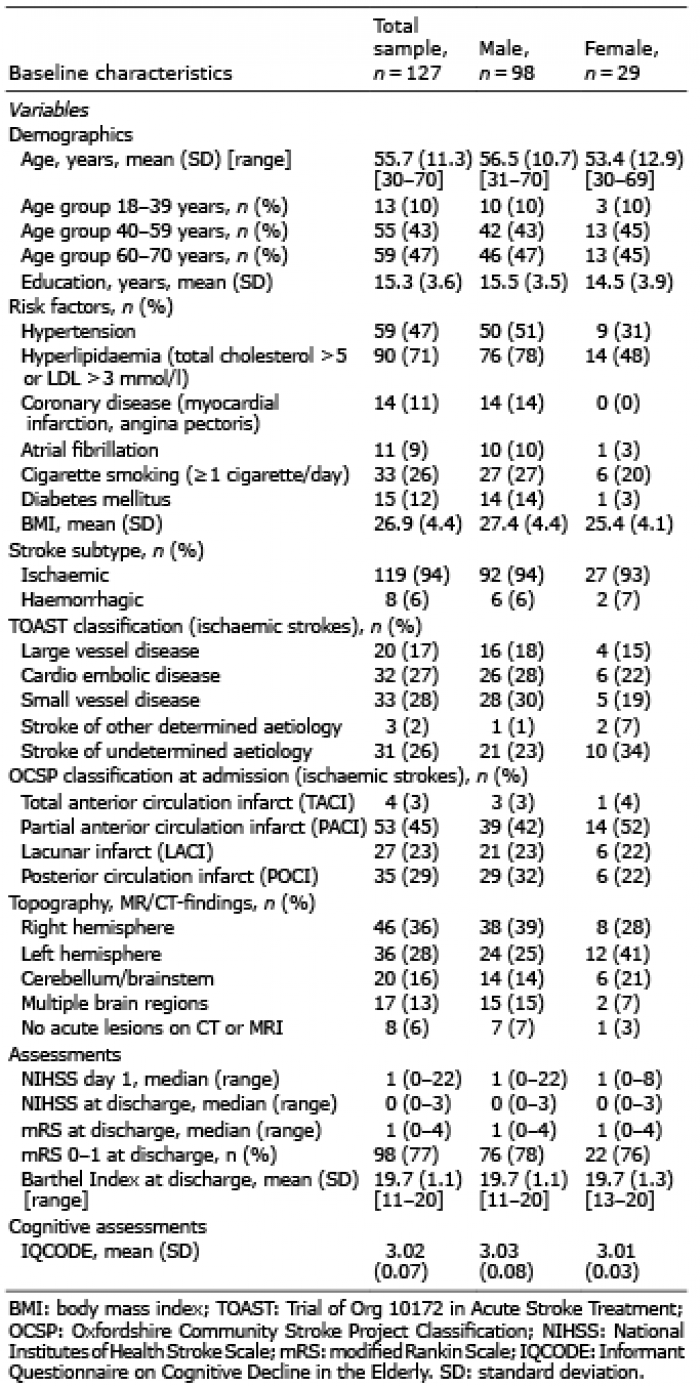 Click to show fullsize
Click to show fullsize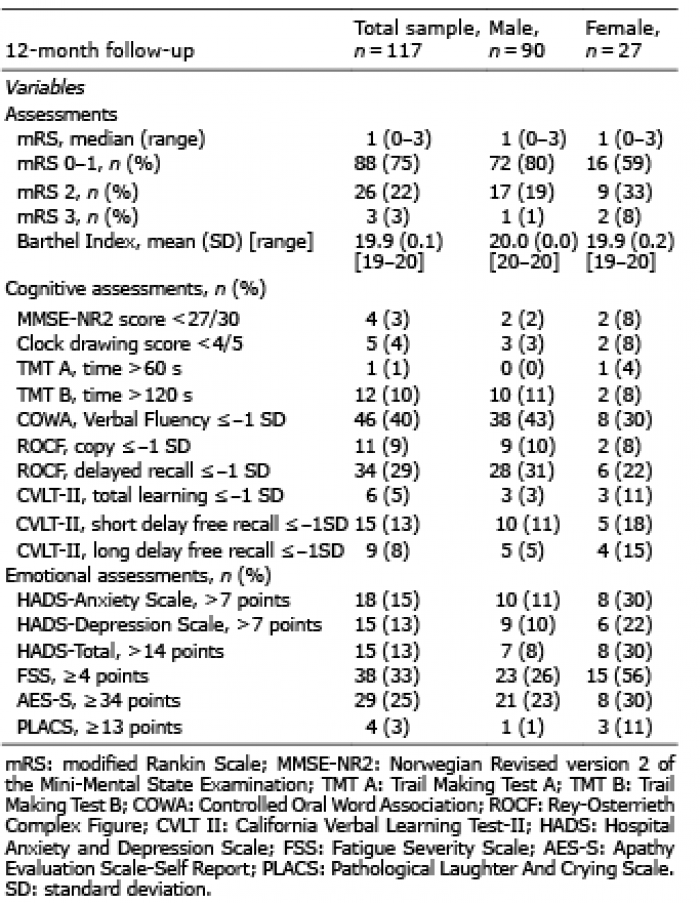 Click to show fullsize
Click to show fullsize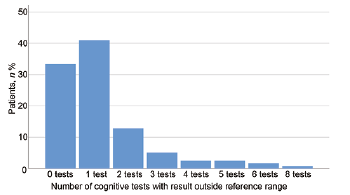 Click to show fullsize
Click to show fullsize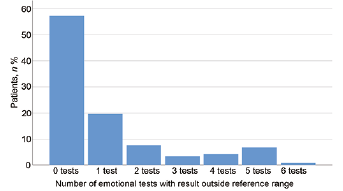 Click to show fullsize
Click to show fullsize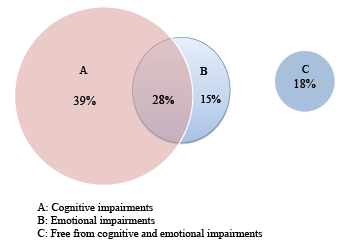 Click to show fullsize
Click to show fullsize