
From the 1Speech and Language Therapy, Swiss Paraplegic Centre, 2Intensive Care Medicine and Respiratory Rehabilitation, Swiss Paraplegic Centre, 3Spinal Cord and Rehabilitation Medicine, Swiss Paraplegic Centre, and 4Swiss Paraplegic Research, Nottwil, Switzerland
Objective: We present a case report that complements the conclusion of Stam et al. in their call to rehabilitation facilities to anticipate and prepare to address post intensive care syndrome in post-
Covid-19 patients.
Methods: The case report presented here provides insight into treating mechanically ventilated post-Covid-19 patients.
Results: Early intervention with dysphagia therapy and speech therapy and ventilator-compatible speak-ing valves, provided within an interprofessional collaborative team, can mitigate the potentially negative consequences of prolonged intubation, long-term use of cuffed tracheostomy, and post intensive care syndrome resulting from Covid-19.
Conclusion: Such a treatment approach can be used to address what is important to patients: to be able to speak with family and friends, eat what they want, and breathe spontaneously.
Key words: Covid-19; post intensive care syndrome; speech and language therapy; swallowing; rehabilitation; tracheostomy management; speaking valve.
Accepted Aug 28, 2020; Epub ahead of print Sep 3, 2020
J Rehabil Med 2020; 52: jrm00100
Correspondence address: Irene Buss, Speech and Language Therapy, Swiss Paraplegic Centre, Nottwil, Switzerland. E-mail: irene.buss@
paraplegie.ch
doi: 10.2340/16501977-2735
This case report aims to complement the conclusion of Stam et al. in their call to rehabilitation facilities to anticipate and prepare to address post intensive care syndrome in post-Covid-19 patients. The case report provides insight into treating mechanically ventilated post-
Covid-19 patients. Early intervention for swallowing and with speech therapy and the use of ventilator-compatible
speaking valves, provided by an interprofessional collaborative team, can reduce the potentially negative consequences of prolonged invasive ventilation and post intensive care syndrome resulting from Covid-19. Most importantly, such a treatment approach can be used to address what is important to patients: to be able to speak with family and friends, eat what they want, and breathe spontaneously.
We read with interest the call for action by Stam et al. (1), for rehabilitation facilities to anticipate and prepare to address post intensive care syndrome (PICS) resulting from SARS-CoV2 (Covid-19). Stam et al. emphasized the importance of adequate screening and early intervention for mechanically ventilated post-Covid-19 patients. As clinicians in speech and language therapy (SLT) and respiratory medicine, we would like to complement their conclusions by reporting insights from our experience treating this patient population in a rehabilitation facility for spinal cord injury/disorders and weaning centre.
As part of the response to the Covid-19 pandemic, a separate ward was set up for post-Covid-19 patients in the Swiss Weaning Centre at the Swiss Paraplegic Centre (SPC), Nottwil, Switzerland. This post-Covid-19 designated ward is exemplary of how intensive care medicine and interprofessional rehabilitation can be combined to provide an effective and efficient care unit. From 15 April to 17 June 2020, this 6-bed interprofessional unit treated 4 female and 13 male patients, ranging from 33 to 75 years of age. The mean length of stay was 20.3 days (range 10–30 days). More than 50% of the patients received complete mechanical ventilation, while the remainder received partially mechanical ventilation combined with spontaneous breathing. All patients were transferred to the SPC for weaning, as the weaning failed in the referring hospitals. More than 60% of the patients had severe critical illness polyneuropathy, and all experienced moderate-to-severe dysphagia and pronounced multifactorial sarcopaenia. Furthermore, a commonality in all patients was the presence of hyperactive (predominately) to mixed delirium. By the end of June, 1 patient was still in a critical condition, 2 had died, 13 had been discharged to standard rehabilitation in the SPC or another rehabilitation hospital, and 1 was transferred back to the psychiatric ward of the originally referring hospital. The patients who recovered were completely oriented, decannulated, and fully oralized (able to eat, drink and swallow medication without increased risk of aspiration).
The following crucial treatment elements were able to expedite improvement in the 17 patients:
This case report aims to highlight that the early application of ventilator-compatible speaking valves is an essential therapeutic and rehabilitative intervention for Covid-19 patients, based on our experience treating patients in the Covid-19-designated ward at the SPC.
Patients who experience severe Covid-19 symptoms due to extremely limited lung functioning often cannot be extubated, indicating the need for a tracheostomy. This was the case for all 17 patients treated in the post-Covid-19 designated ward at the SPC. Mechanical ventilation using a cuffed tracheostomy tube (an inflated balloon surrounds the tube) omits the use of an orotracheal tube in the pharynx and larynx, forcing inspiration and expiration to take place completely through the tracheostomy tube. This results in a continued lack of airflow through the upper respiratory tract, with serious consequences for the patient’s ability to communicate and swallow. For example, without airflow through the larynx, pharynx, mouth, and nose, the production of voice and speech, as well as reflexive and/or voluntary throat-clearing and coughing as important salivation and phlegm clearing functions are impossible. Furthermore, the collection of saliva resulting from deficient clearing functions can lead to long-term desensitization of the pharynx, larynx and the area of the trachea above the cuff, as well as increased aspiration of saliva up to the cuff at least. Consequently, desensitization of the upper respiratory tract organs “trains” dysphagia in patients, which can lead to silent aspiration with potentially life- threatening pneumonia, even on the ward. Moreover, studies have shown that long-term cuffed tracheostomy tubes negatively affect the overall rehabilitation process (2–8).
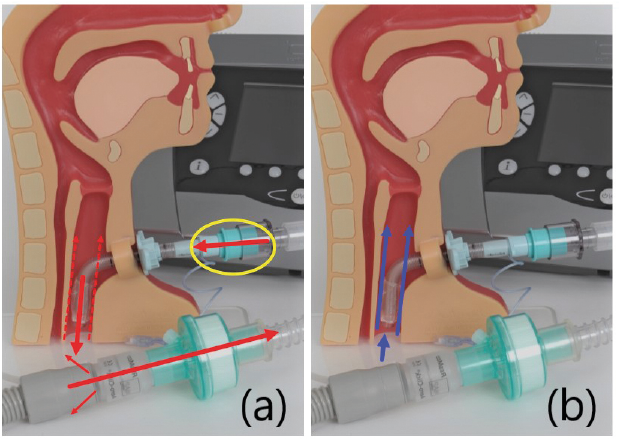
The inability to communicate verbally has huge negative consequences for a person’s mental health and quality of life, often coupled with misunderstandings and frustration (10–12). For Covid-19 patients, this is exacerbated by the absence of face-to-face contact with friends and family. In order to facilitate verbal communication and oral food intake in fully ventilated patients in its intensive care unit (ICU), SPC generally uses ventilator-compatible speaking valves as soon as the positive end-expiratory pressure (PEEP; i.e. the pressure given at the end of the exhalation phase of a respiratory cycle that allows increased time for oxygen exchange) (13) is <8 cmH2O. The cuff of the tracheostomy tube must be completely deflated before the valve can be inserted. Furthermore, the treatment team must ensure that the exhaled air can pass alongside the tracheostomy tube (as seen in Fig. 1). Making sure that there is sufficient space between the tracheostomy tube and the trachea is essential to safe-guard the patient from suffocating and to ensure that the serum CO2 level does not increase. Therefore, the outer diameter of the tracheostomy tube needs to be selected to suit the anatomy of the patient’s trachea. This is essential for safe use of the speaking valve. Also key to safe use is a well-trained treatment team regarding the use of ventilator-compatible speaking valves. Moreover, a closely collaborating interprofessional team can immediately address any potential patient safety issues, tipping the balance toward benefits over the risks of using ventilator-compatible speaking valves.
Fig. 1. Inserted ventilator-compatible speaking valve (PMV® 007, Passy-Muir, Inc., Irvine, California (USA)) during ventilation. (a) Airflow during inspiration, and (b) during expiration (9). There must be sufficient space next to the empty cuff for the exhaled air.
The SPC has approximately 20 years of positive experience with this interprofessional approach to early valve use. The earlier the patient is able to physiolog-ically exhale, at least intermittently, the greater the likelihood that desensitization and dysphagia can be avoided and the earlier these problems can be treated, if necessary. Moreover, there is some evidence that the use of speaking valves decreases the respiratory rate and the amount of CO2 in exhaled air (EtCO2) (14). It is important to note, however, that since the approach of deflating the cuff and deployment of a ventilator-compatible speaking valve with Covid-19 patients is considered an aerosol-generating measure, the decision to employ this treatment approach must weigh the health risks to the interdisciplinary team members vs the patient benefits. In light of the risk–benefit considerations, SPC decided to employ this approach with Covid-19 patients with strict adherence to the established precautionary protection measures and optimal use of personal protective equipment (PPE). There has been no evidence of virus transmission from patient to staff resulting from this approach at SPC.
An example of employing ventilator-compatible speaking valves in the treatment of Covid-19 patients is a 62 year-old man who was admitted to SPC with severe acute respiratory distress syndrome due to Covid-19. With no relevant pre-existing conditions, he presented with critical illness polyneuromyopathy, ventilator-associated diaphragm dysfunction, weaning failure, tracheotomized, and completely mechanically ventilated with inflated cuff. He was completely nourished through a nasogastric tube. Due to the cuffed tracheostomy tube that was inserted 6 weeks prior to admission, the patient was unable to inform the treatment team of his needs or express his fears and experience of pain. Furthermore, it was impossible for him to (video) call with his family, and he was unable to write messages due to his tetraplegia. During a time of a serious health crisis and uncertainty about the patient’s prognosis, the inability to communicate, coupled with the impossibility of receiving visits from family (as part of the Covid-19 precautionary protection measures) implies for the patient unimaginable isolation, a feeling of being trapped, stress, psychological burden and, ultimately, physical burden. Interventions to restore the ability to communicate verbally are therefore essential.
In close collaboration between the SLTs and intensive care nurses, a ventilator-compatible valve could be inserted for the first time in this patient. Initially he struggled with accumulated pharyngeal secretion, but with some compression of the abdomen, he was able to cough it up. This led to an improvement in airflow in the upper respiratory tract and the first step toward enabling vocalization. After the second attempt, he was successful in speaking with the speaking valve, and a higher frequency of swallowing was observed. The patient was even able to swallow, albeit hesitantly, the first bolus of food (raspberry sorbet), which he clearly enjoyed, verbally commenting “it is good”; a small step towards normalcy. After 2 weeks of intensive functional dysphagia therapy, he was able to eat soft food with supervision while breathing spontaneously with the speaking valve. However, due to limited pharyngeal/laryngeal sensitivity and the associated risk of saliva aspiration, and weak voluntary coughing (200 L/min), tracheal suctioning was required. Moreover, his lungs were severely strained by Covid-19. To avoid unnecessary complications due to aspiration, the SLTs conducted frequent clinical evaluations of swallowing functions, and together with the ear-nose-throat (ENT) physician, performed fibreoptic endoscopic evaluation of swallowing to monitor swallowing. Four weeks after admission to the ICU, it was possible to safely remove the patient’s nasogastric and tracheostomy tubes. Interprofessional tracheostomy management enabled the patient to communicate verbally with his family, express his feelings about his dramatic experience with Covid-19, and eat and enjoy his favourite foods.
Speaking and swallowing are major milestones in a patient’s rehabilitation, as evidenced by this case report. The authors have observed that improvement in these aspects of functioning have an anti-delirogenic effect, and can be a motivator for patients to be more actively involved in their rehabilitation. We postulate that early intervention with dysphagia therapy and speech therapy and the use of ventilator-compatible speaking valves provided within an interprofessional collaborative team can mitigate the potential negative consequences of prolonged intubation followed by long-term use of cuffed tracheostomy, and extensive ICU-acquired weakness or PICS resulting from Covid-19. Furthermore, the early application of ventilator-compatible speaking valves supports weaning off mechanical ventilation (14–16). The authors recognize that this approach may be difficult to implement in some acute settings; nevertheless, the benefits to patients warrant the attempt. Specifically, such an intervention approach can improve verbal communication and help patients to regain their sense of taste and smell (if not damaged by Covid-19) and considerably contribute to patients’ overall well-being and early restoration of quality of life.
The authors have no conflicts of interest to declare


 Click to show fullsize
Click to show fullsize