
From the 1Department of Cardiovascular Rehabilitation, National Cerebral and Cardiovascular Center, Osaka, 2Department of Internal Medicine and Rehabilitation Science, Disability Science, Tohoku University Graduate School of Medicine, Sendai, 3Department of Nursing, National Cerebral and Cardiovascular Center and 4Department of Cardiovascular Medicine, National Cerebral and Cardiovascular Center, Osaka, Japan
Objective: This study elucidated the effects of exercise training on physical activity, 6-min walk distance, and all-cause hospitalization rates in patients with chronic heart failure, and evaluated factors contributing to changes in physical activity.
Design: Prospective cohort observational study.
Patients and methods: Patients (n =62) who completed an exercise training programme after implantable cardioverter-defibrillator or cardiac resynchronization therapy treatment between May 2017 and May 2018 were included. Patients exercised for 20–50 min 3–5 times weekly for 3 months and were assigned to the active (≥ 10 min/day) or non-active (< 10 min/day) group based on changes in walking times between baseline and 3 months, as assessed by the International Physical Activity Questionnaire.
Results: The 6-min walk distance improved in both groups with exercise training. Physical activity level did not increase in some patients, despite improvements in exercise tolerance. Depression improved significantly in the active group, but no correlation was found with physical activity. Factors contributing to physical activity changes were not identified. The all-cause hospitalization rate was lower in the active group during follow-up (mean 10.5 months).
Conclusion: Exercise training effectively increased 6-min walk distance regardless of physical activity. Non-active patients experienced increased all-cause hospitalizations. Increasing physical activity improves patient outcomes.
Key words: exercise; defibrillator; heart failure.
Accepted Aug 6, 2020; Epub ahead of print Aug 24, 2020
J Rehabil Med 2020; 52: jrm00111
Correspondence address: Masahiro Kohzuki, 1-1 Seiryo-cho, Aoba-ku, Sendai 980-8574, Japan. E-mail: kohzuki@med.tohoku.ac.jp
Doi: 10.2340/16501977-2728
Patients who completed an exercise training programme after implantable cardioverter-defibrillator or cardiac resynchronization therapy treatment in our institution between May 2017 and May 2018 were included. The aim of this study was to determine the effects of exercise training on walking time, 6-min walk distance, and hospitalization rate. Patients exercised for 20–50 min 3–5 times weekly for 3 months. Training helped patients with implantable cardioverter-defibrillator or cardiac resynchronization therapy improve the 6-min walk distance, regardless of changes in physical activity. However, the non-active group had higher rates of all-cause hospitalization. Increasing physical activity improves patient outcomes.
Patients with heart failure (HF) experience ventricular tachycardia or ventricular fibrillation with a recurrence rate of 10–20% (1). Implantable cardioverter-defibrillator (ICD) and cardiac resynchronization therapy (CRT) defibrillator (CRT-D) are highly effective for decreasing mortality from ventricular tachycardia or ventricular fibrillation (2, 3). CRT is a highly effective treatment for drug-refractory systolic heart failure (HF) patients with a wide QRS complex (3, 4). Treatment with CRT results in left ventricular (LV) reverse remodelling, based on the findings of a decrease in LV size and/or increase in LV ejection fraction (LVEF), which reduces morbidity and mortality (3). However, studies have shown that clinically significant anxiety disorders and depressive symptoms are prevalent among patients with ICD and CRT defibrillator (CRT-D) (5, 6).
Decreased physical activity (PA) is common, regardless of shock exposure, among patients with ICD and CRT-D (7–9). After ICD or CRT treatment, exercise training (ET) has been reported to improve exercise capacity without adverse events (4, 10–12). In addition, reports suggest that this improves the patients’ prognosis. Increased PA in patients with ICD or CRT-D is associated with decreased HF hospitalization and mortality rates (13, 14). However, the effects of ET on PA in patients with ICD and CRT-D are unclear. There-fore, this study aimed to elucidate the effects of ET on PA and 6-min walk distance (6MWD) or all-cause hospitalization, and to clarify factors contributing to the change in PA in chronic HF patients with ICD or CRT.
Ethical considerations
This study was conducted in accordance with ethical standards on human experimentation and with the Declaration of Helsinki 1975, revised 1983. In particular, the study protocol was approved by the ethics committee of the National Cerebral and Cardiovascular Center (approval number M26-015), where the study was performed. All patients provided written informed consent.
Study design and participants
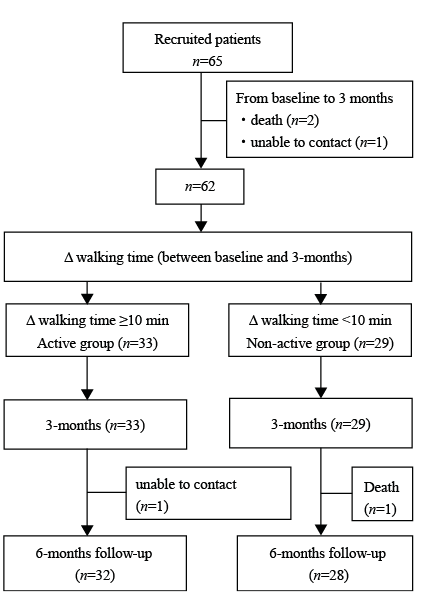
This prospective observational cohort study included patients who completed a 3-months ET programme after ICD, CRT-pacemaker (CRT-P) or CRT-D treatment at our institution between May 2017 and May 2018. Patients were eligible for the ET programme if they met any of 3 criteria (LVEF ≤ 40%, percent predicted peak oxygen uptake ≤ 80%, and B-type natriuretic peptide level ≥ 80 pg/ml) and had been referred to the programme at their physicians’ discretion. Between May 2017 and May 2018, 65 patients met the inclusion criteria. Two patients died, and 1 did not complete the questionnaire; thus, 62 participants were included in the analysis. Treatment for HF was tailored to all patients based on current guidelines, which were consistent throughout the study period (15). HF patients treated with an ICD or CRT were evaluated in prospective observational studies at baseline (at the beginning of the ET programme), 3 months (at the end of the 3-months ET programme), and 6 months (3 months after the end of ET programme).
After 3 months of ET, participants were categorized into 2 groups according to the walking time assessed by the International Physical Activity Questionnaire (IPAQ). Based on the change in walking time between baseline and 3 months, patients who walked ≥ 10 min/day were allocated to the “active group” (n = 33) and those < 10 min/day were allocated to the “non-active group” (n = 29, Fig. 1), based on a study that reported a 10-min increase in PA reduced HF hospitalization risk by 4% (13). After identifying the 2 groups, baseline data were analysed retrospectively.
Fig. 1. Study design flowchart.
Exercise programme
A description of the exercise protocol has been published previously (4). The 3-months ET programme began with supervised in-hospital sessions consisting of walking, bicycle ergometer, and low-intensity resistance training for 20–40 min sessions 3–5 times per week, followed by home ET combined with once- or twice-weekly supervised in-hospital ET sessions. The duration increased to 30–60 min, and the intensity of the endurance exercise was determined individually at a heart rate corresponding to 40–60% of the heart rate reserve (maximum heart rate minus resting heart rate), anaerobic
threshold level obtained on baseline cardiopulmonary exercise testing, or at level 12–13 (“a little hard”) of the 6–20 scale perceived rating of exercise (original Borg scale). All patients were encouraged to continue home ET with an individualized exercise prescription, based on the cardiopulmonary exercise testing or 6-min walk test results at baseline and 3 months. Individualized exercise prescriptions were tailored throughout the study period based on current guidelines (16).
Physical activity
PA was assessed using the IPAQ score and step count. IPAQ has high reliability and validity when monitoring PA across diverse populations (17) and has, therefore, become the most widely used questionnaire to assess PA. In addition, the reliability and validity of the Japanese version have been verified (18). This study used the IPAQ short form, and activities of different intensities were reported for each domain. Domains were divided into vigorous PA, moderate PA, and walking. Weekly duration estimates for vigorous and moderate PA were calculated by multiplying the time spent performing the activity in a typical day by the number of days in the past week spent performing that activity. Weekly durations were then multiplied by metabolic equivalent (MET) values for the different activities to calculate MET-minutes per week for each intensity level. To determine sedentary time, patients were instructed to think about the time they spent sitting or lying at work, at home, while doing course work, and during leisure time. Time spent sleeping was excluded from sedentary time. Then they were asked to estimate the total number of h and min per day they spend sitting or lying within a day. IPAQ values were used to determine the walking time. Walking time was calculated as time (min) × frequency (times/week)/7. Participants were interviewed immediately after completing IPAQ to prevent recall bias.
A description of the step count protocol has been published previously (19). Briefly, all patients wore a triaxial accelerometer (AM500N; Acos Co. Ltd, Nagano, Japan) 24 h a day for 8 days, except while bathing and sleeping (19). Continuous data from the final 7 days of the 8-day collection period were used to assess daily patient PA (19). Step counts were recorded after age, sex, height, and weight were entered for each patient. In addition, the active MET was set to 2.8, according to a previous study on the activity amount targeting the device (18, 20). The active step count was steps at 2.8 METs, and the active activity time was the activity time at 2.8 METs. IPAQ and step counts were assessed at baseline. Furthermore, IPAQ findings and step counts were assessed at the 3rd (from 8 days before the end of the 3-months period to the end of the 3-months period) and 6th months (from 8 days before the end of the 6-months period to the end of the 6-months period) follow-up examinations.
Physical performance
This study followed a previously published protocol for measuring isometric knee extensor muscle strength (IKEMS) (4). In summary, IKEMS was measured using the μ-Tas MF-1 assembly (Anima Co. Ltd, Tokyo, Japan) (21) at baseline and after 3 months of ET. A 6-min walk test was also performed at baseline and after 3 months of ET. Participants were asked to walk continuously for 6 min with maximum effort, and the distance was recorded.
Depression and quality of life
Symptoms of depression were measured using the Patient Health Questionnaire-9 (PHQ-9), with items mirroring the diagnostic criteria for major depressive disorders (22). Patients were asked to rate items on the questionnaire on a scale from 0 (not at all) to 3 (nearly every day) according to their symptoms during the past 2 weeks (22, 23). Scores in the PHQ-9 range from 0 to 27, and a cut-off score >10 was used to detect patients with clinically relevant levels of depression (23, 24).
Quality of life (QOL) was assessed using the Japanese version of the Medical Outcomes Study 36-Item Short-form Health Survey (SF-36) questionnaire (25–27). The SF-36 consists of a physical component summary (PCS), mental component summary (MCS), and role component summary (RCS) score. The final score (range 0–100) was calculated according to recommendations from the SF-36 guidelines, with higher scores representing a better QOL (25–27). The patient PHQ-9 and SF-36 data were evaluated at baseline and at 3 and 6 months.
Statistical analyses
Data are expressed as mean and standard deviation (SD) unless otherwise stated. Categorical variables were compared using Fisher’s exact test. Comparisons between groups were analysed using the unpaired Student’s t-test or Wilcoxon rank-sum test, depending on normality of distribution. Comparisons within groups were analysed using the paired t-test or Wilcoxon signed-rank test. Based on a study by Abraham et al. (28), that used increases in the 6MWD to determine sample size, a sample size of 20 was required to detect an increase of 53 m in the 6MWD in patients with HF after CRT, with a standard deviation of ±66 m, power of 0.80, and α value set at p < 0.05 (2-tailed). Analysis of covariance (ANCOVA) was used to examine changes during the 3-months ET programme with the corresponding baseline measurement used as a covariate. Spearman’s rank correlation coefficients were used to evaluate the relationships between change in walking time and other variables of interest. Differences of all-cause hospitalizations, HF hospitalization, and ICD therapy (excluding CRT-P) in the active and non-active group were compared using Kaplan–Meier survival curves and compared using the log-rank test. All statistical analyses were performed using JMP Pro version 14.2.0 (SAS Institute, Cary, NC, USA). For all tests, p < 0.05 was considered statistically significant.
Attendance at the supervised in-hospital ET sessions during the 3-months ET programme was similar in the 2 groups (active group: mean 16 (SD10), non-active group: mean 16 (SD 9), p = 0.887). Fourteen participants (42%) in the active group completed < 12 sessions of the supervised in-hospital sessions. Among the remaining participants, 2 (6%) completed all 36 sessions; 6 (18%) completed 24–36 sessions. In the non-active groups, 10 of the 29 (34%) completed < 12 sessions of the supervised in-hospital sessions. In the remaining participants, 2 (7%) completed all 36 sessions; 2 (7%) completed 24–36 sessions.
During the 3-months ET programme, there were no exercise-related adverse events, such as ventricular tachycardia, ventricular fibrillation, the occurrence of anti-tachycardia pacing or shock, lead dislocation, deterioration of the surgical wound site, or device malfunction.
Patient characteristics
There were no significant differences in patient characteristics between the active and non-active groups (Table I). In both, active and non-active groups, the number of patients receiving CRT was 19.
Table I. Patient characteristics
Changes during the 3-months exercise training programme
There was a significant improvement in 6MWD in both groups (p < 0.01). However, the PHQ-9 score significantly improved only in the active group (p < 0.01). The active group also showed significant improvement in IKEMS, sedentary time, walking according to the IPAQ, walking time, step count, PCS, and RCS (p < 0.01) (Table II).
Table II. Changes in variables during the 3-months exercise training programme
In the non-active group, walking according to the IPAQ and walking time decreased significantly (Table II). However, RCS improved significantly.
Significant differences were found between the groups. The sedentary time, walking, walking time according to the IPAQ, active step count, PHQ-9, and PCS were better in the active group than in the non-active group (Table III).
Table III. Adjusted mean difference in outcomes after exercise training
Follow-up and adverse events
The mean PHQ-9 of the active group was significantly worsened between 3 and 6 months (3.0 (SD3.4) to 4.0 (SD 3.8), p = 0.037). There was a significant increase in walking according to the IPAQ in the non-active group from 3 to 6 months (mean 379 MET-minutes/week (SD 443) to 768 MET-minutes/week (SD 765), p < 0.001). Other factors did not change significantly. There were no significant differences in HF hospitalization or ICD therapy (4 active (4 from anti-tachycardia pacing) vs 6 non-active (3 from anti-tachycardia pacing)) between the active and non-active groups. However, during a mean follow-up of 10.5 months, the number of all-cause hospitalizations was higher in the non-active group than that in the active group, with 13 (11 from cardiac causes) and 6 (4 from cardiac causes) all-cause hospitalizations, respectively (p = 0.037) (Fig. 2A–C). No significant differences in all-cause hospitalizations were shown among patients in the ICD and CRT groups in the active and non-active groups.
Univariate analysis of change in walking time by exercise training between baseline and 3 months with clinical characteristics
Change in walking time was significantly related to walking (r = –0.28; p = 0.031) and walking time (r = –0.28; p = 0.029) according to the IPAQ at baseline (Table IV). However, the correlation coefficient was low. Other factors were not significantly related (Table IV).
Table IV. Univariate analysis of change in walking time by exercise training (ET) between baseline and 3 months with clinical characteristics
Fig. 2. Kaplan–Meier curves for all-cause hospitalizations, heart failure (HF) hospitalization, and implantable cardioverter-defibrillator (ICD) therapy in the active and non-active groups. The rate of all-cause hospitalization is significantly higher in the non-active group (2A). Heart failure hospitalization (2B) and defibrillation therapy events (2C) do not show any significant difference.
Results from patients who were treated with CRT or ICD and completed ET showed that the PA level did not increase in some patients, despite improvements in exercise tolerance associated with ET. To our knowledge, this is the first study to report changes in the PA of patients receiving CRT who completed ET.
Gad et al. reported that 3 months after CRT treatment without ET, patient step counts were significantly reduced (29). Furthermore, it has been reported that the PA of HF patients after ICD and CRT treatment without ET increased, but the measuring device used in the studies was a single-axis accelerometer (13, 14). Therefore, it is difficult to compare the results of the studies with those of the present study, because a tri-axial accelerometer and a different measurement algorithm were used. Nonetheless, a 10-min increase in PA among ICD or CRT-D patients resulted in decreased HF hospitalization and mortality rates (13, 14). However, it remains unclear whether exercise tolerance or daily step count is a prognostic indicator in HF patients after ICD and CRT treatment. To date, exercise tolerance has often been used as a prognostic indicator. In this study, patients treated with CRT or ICD who completed ET showed a significant increase in 6MWD. Therefore, it has been shown that completing this ET may contribute to improving their prognosis. Furthermore, the active group also showed significant improvement in IKEMS, sedentary time, walking according to the IPAQ, walking time, step count, PCS, and RCS (p < 0.01). A recent study reported that daily step counts objectively measured by an accelerometer may be a prognostic indicator of mortality rather than peak oxygen uptake in Japanese outpatients with HF who did not receive ICD or CRT treatment (19). Therefore, these results reveal why the all-cause hospitalization rate was lower in the active group.
In this study, the non-active group had higher rates of all-cause hospitalization than the active group. No patients in either group experienced exercise-related adverse events, including ICD therapy and HF hospitalization, similar to the findings of previous reports (4, 10). Steinhaus et al. reported that 16% of patients with ICD or CRT-D implants who participated in ET had ICD therapy during follow-up (12). In this study, 17.5% of all patients at 12.2 months had adverse events unrelated to ET, including ICD therapy. However, despite the improvement in exercise tolerance, the non-active group had significantly more all-cause hospitalizations. Izawa et al. reported that a reliable indicator of mortality among patients with HF was daily step count, with a cut-off of 4,889 steps/day (19). The step count was lower than the cut-off value in the non-active group. Furthermore, the American Heart Association recently released a Science Advisory that highlighted the deleterious association between sedentary behaviour and cardiovascular disease morbidity and mortality (30). In this study, sedentary time did not significantly improve in the non-active group; hence this group was considered to have a poorer prognosis, with a higher risk of all-cause hospitalization. However, it remains unclear whether hospitalization decreases due to longer increments of PA or if patients with lower levels of PA are more susceptible to re-admission.
Among patients with ICD and CRT-D, clinically significant anxiety disorders and depressive symptoms are prevalent (5, 6). Moreover, with no relation to shock exposure, low PA has been described (7, 8). Using PHQ-9 in this study, the active group showed significant improvement from baseline to 3 months, whereas the non-active group tended to deteriorate. Therefore, we surmised that changes in PA and depression were related. However, no correlation was found between PA and depression, possibly because the baseline score was higher than that in a previous report (31).
Borland et al. reported that group-based exercise did not improve the PA level in patients with chronic heart failure and comorbidity (32). Our results show that the PA level did not increase in some patients, despite improvement in exercise tolerance associated with ET. In the future, it is important to construct a programme to increase PA that differs from conventional cardiac rehabilitation methods. For example, home-based training guided by the telemonitor has been reported to improve exercise tolerance safely by reducing the levels of anxiety and depression; an increase in PA is also expected with this training (33).
This study had some limitations. First, this study lacked a control (non-exercise) group from a single institute. Secondly, it included a small number of patients from a single centre. Moreover, an accelerometer could not be obtained in all patients. However, a study assessing PA in patients undergoing CRT had a similar sample size (29). This study had a small sample size, and therefore shock and anti-tachycardia pacing treatments in ICD therapy were not delineated. Thirdly, the participation rate of supervised ET was low in the active and non-active groups; however, there was no difference between the 2 groups. Therefore, the impact on PA was small. Finally, it was difficult to calculate the sample size between groups, and the study may thus have been underpowered.
In conclusion, patients who underwent ET after CRT or ICD treatment showed a significant increase in 6MWD regardless of the change in PA. Nevertheless, the non-active group had higher rates of all-cause hospitalization than the active group. Future studies should focus on constructing exercise programmes to decrease hospitalization risk for patients, especially for those who do not show increased PA.
The authors acknowledge the support of Mieko Akachi, Yukihiro Shimada, Noriyuki Fukui, and Taiki Sato in preparing this manuscript.
Funding. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize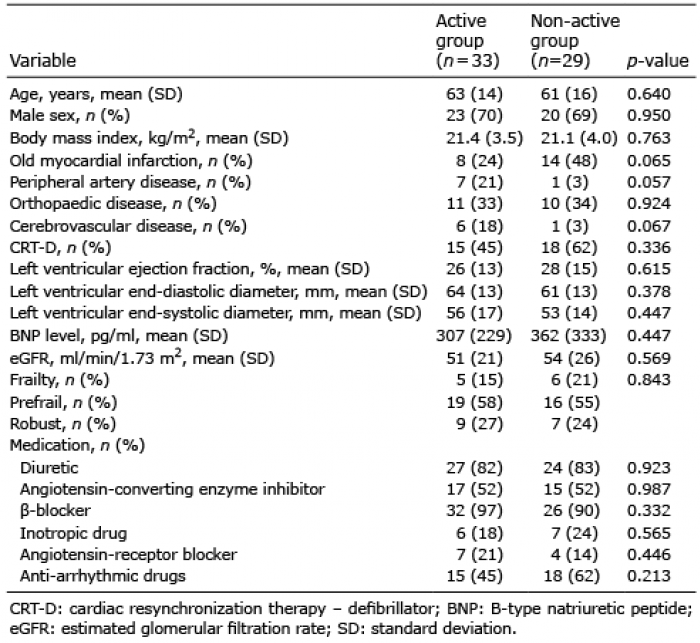 Click to show fullsize
Click to show fullsize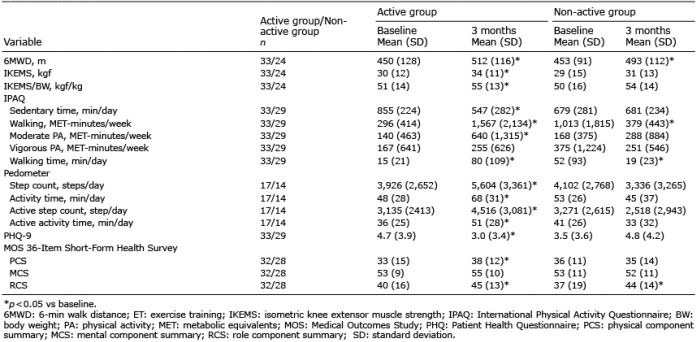 Click to show fullsize
Click to show fullsize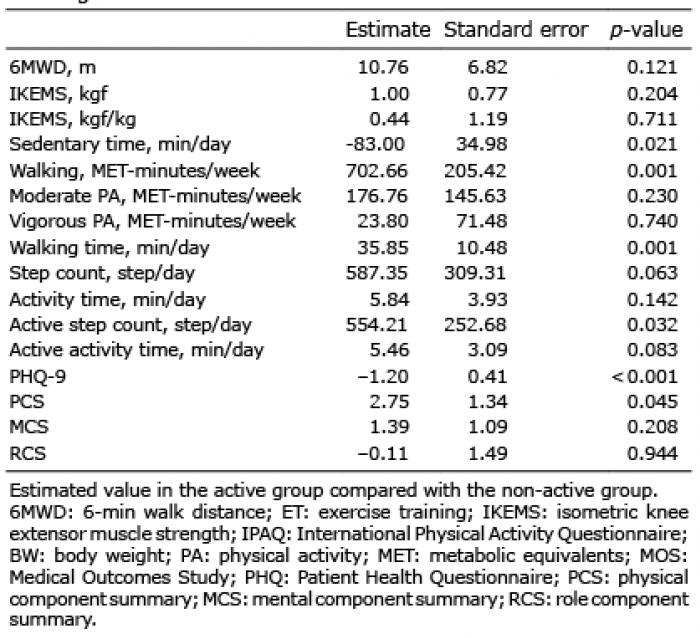 Click to show fullsize
Click to show fullsize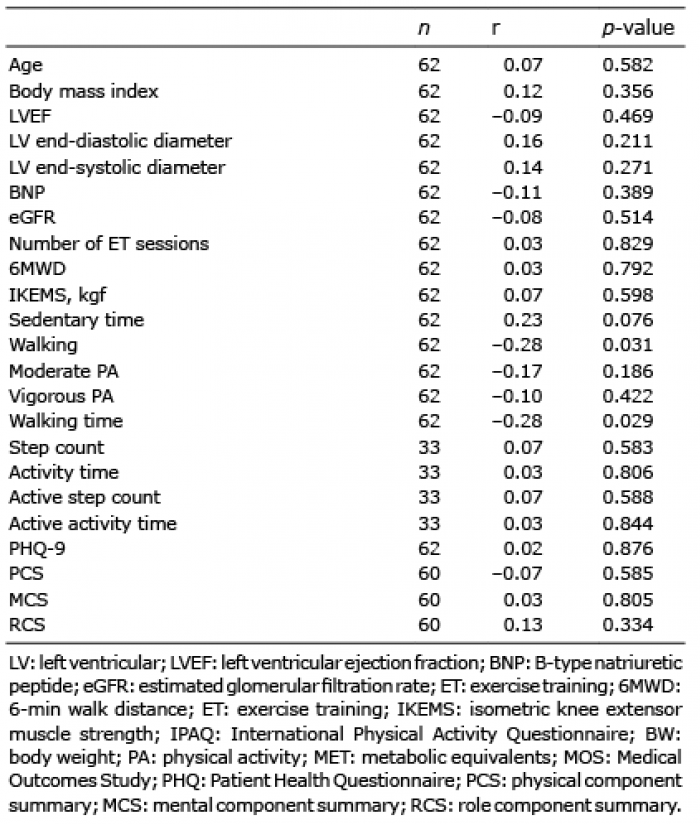 Click to show fullsize
Click to show fullsize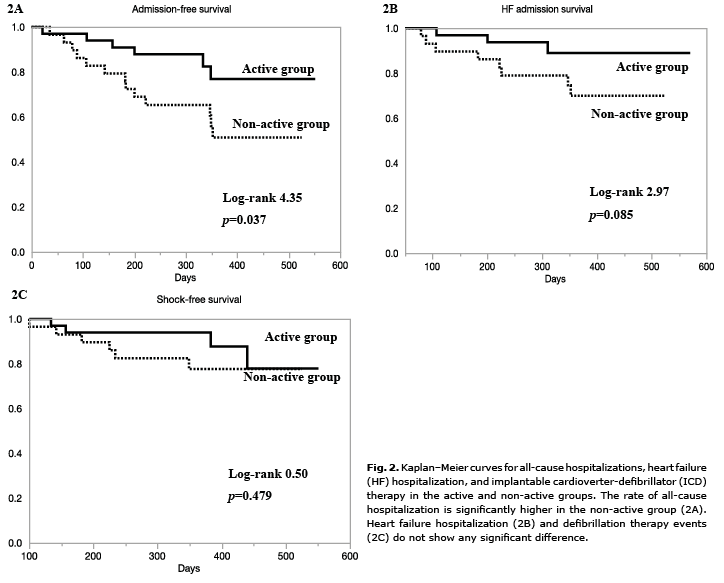 Click to show fullsize
Click to show fullsize