
Objective: To evaluate the effectiveness of non-surgical interventions for rotator cuff calcific tendinopathy.
Data sources: Medline, EMBASE, CINAHL, Cochrane Register of Clinical Trials, PEDro and SPORTDiscus from inception to March 2018, and accompanying reference lists. Peer-reviewed randomized clinical trials of non-surgical interventions for adults with rotator cuff calcific tendinopathy were included.
Data extraction: The same 2 reviewers independently evaluated eligibility, extracted data and evaluated risk of bias of the included randomized clinical trials. A system to resolve any disagreements was established a priori. Short-term, medium-term and long-term outcomes for pain, shoulder function and calcific morphology related to rotator cuff calcific tendinopathy were extracted. Due to diversity in outcome measures a meta-analyses was not conducted.
Data synthesis: Of the 2,085 articles identified, 18 met the inclusion criteria, all of which had high risk of bias. Five non-surgical interventions were identified (extracorporeal shockwave therapy, ultrasound-guided percutaneous intervention, pulsed ultrasound, acetic acid iontophoresis, and transcutaneous electrical nerve stimulation).
Conclusion: There was moderate evidence for the benefit of high energy extracorporeal shockwave therapy over low energy extracorporeal shockwave therapy for pain and function between 3 and 6 months follow-up, and benefit over placebo for improved function at up to 6 months follow-up. There was moderate evidence for the benefit of ultrasound-guided percutaneous intervention over medium/high-energy extracorporeal shockwave therapy for reduced pain and calcific morphology when followed up over a one-year period. Methodological concerns preclude definitive recommendations.
Key words: tendinopathy; shoulder; high-energy shock waves; ultrasound-guided fine needle aspiration; calcification; rotator cuff; barbotage.
Accepted Aug 3, 2020; Epub ahead of print Aug 18, 2020
J Rehabil Med 2020; 52: jrm00119
Correspondence address: Mitchell Simpson, Melbourne Medical School, University of Melbourne, Parkville, Victoria, Australia. E-mail: mitchell.simpson92@gmail.com
Doi: 10.2340/16501977-2725
Calcific tendinopathy of the shoulder is a relatively common condition, characterized by the presence of calcium deposits in the shoulder tendons, which may be associated with shoulder pain and dysfunction. To help guide the most appropriate treatment and future research in the area, a thorough review of the best available research was conducted. Overall, it was found that there is a lack of high-quality research in this area. Based on the current research, high-energy shockwave therapy and ultrasound-guided needling appear to be the best treatment options available for reducing shoulder pain, improving shoulder function and reducing the size of calcium deposits in the shoulder tendons. However, without further high-quality research in this area, it is not possible to inform people seeking care which is the best management option.
Rotator cuff calcific tendinopathy (RCCT) involves the deposition of calcium within the rotator cuff tendons of the shoulder. Calcification may be present without symptoms, but, when symptomatic, the condition is associated with shoulder pain and dysfunction. A definitive explanation as to why some people remain asymptomatic and others experience severe symptoms, as well as the mechanisms(s) for the experience of pain, remain elusive.
The observation of calcific deposits is a common radiographic and ultrasonographic finding (1–4). It has been observed in 7.8–13.6% of people not reporting shoulder symptoms (3, 4), and in 33.3–42.5% of people with symptoms (3, 4). When both symptoms and imaging calcification are present, it is diagnosed as RCCT. The condition manifests most frequently in middle-aged adults (4–7) and presents more commonly in women (8). The reasons for these observations are uncertain.
When symptoms are present, observed RCCT is associated with tenderness near the greater tuberosity of the humerus, nocturnal discomfort, and reduced shoulder range of motion (ROM) (5, 9, 10). Three stages of the condition have been defined (pre-calcific, calcific and post-calcific), with symptoms thought to peak during the calcium resorption that occurs in the latter phases of the calcific stage (11). Radiological studies have also attempted to classify calcific morphology (e.g. size, density, shape of deposits), but have not attempted to correlate morphology with symptoms (5, 6, 12, 13). The pathoaetiology of RCCT remains equivocal and may be self-limiting (10, 11). Non-surgical intervention is typically recommended as the first stage of management for RCCT (8, 11).
Most non-surgical interventions focus on reducing pain and increasing shoulder function irrespective of the calcifications present (14, 15). These include; rest, non-steroidal anti-inflammatory drugs (NSAID), subacromial steroid injections (SAI), strengthening based exercise programmes, transcutaneous electrical nerve stimulation (TENS), acetic acid iontophoresis (AAI) and pulsed ultrasound (US) (14–16). For patients with more prolonged or severe symptoms, a number of non-surgical interventions aim at reducing the calcium deposit, with an assumption that by reducing the calcification, pain and shoulder function will improve (17). These minimally invasive non-surgical interventions include ultrasound-guided percutaneous irrigation of the calcific deposits (US-PICT), such as needling and lavage (barbotage), and extracorporeal shockwave therapy (ESWT), and have been recommended (16, 18–20). Technique selection is complicated by the substantial variation between and within available modalities. For example, ESWT has different energy outputs, application type, frequency of treatment, and duration of sessions, making comparisons between interventions challenging.
Four systematic reviews have relatively recently synthesized research in this area (15, 16, 18, 19). However, by not including all non-surgical interventions, defining potential therapeutic interventions as placebo and the possibility of a delayed treatment effect influencing a subsequent treatment may have introduced considerable uncertainty in the conclusions reached. The most recent systematic review (18) was limited to ultrasound-guided lavage trials and did not compare interventions with placebo. Since the last systematic review (16), additional non-surgical randomized clinical trials (RCTs) have been conducted (21, 22), highlighting the need to update existing reviews and consider the influence of potential confounding issues regarding recommendations for the management of RCCT. Furthermore, previous reviews have highlighted the need to develop a consensus on the most effective treatment protocol for each non-surgical intervention technique (15).
The primary aim of this review was to evaluate the effectiveness of non-surgical interventions on pain and function in adults with RCCT. This review included all non-surgical interventions and included combined interventions (e.g. US-PICT plus SAI). The secondary aims of the review were to examine the outcomes of intra-modality non-surgical protocols, and to identify whether evidence exists for non-surgical interventions to reduce the presence of calcification in adults with RCCT. The combined aim was to provide guidance, based on a synthesis of the literature, on the best non-surgical intervention for RCCT.
The review protocol was registered a priori with PROSPERO the International Prospective Register of Systematic Reviews (registration number: CRD42018089996). Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and Cochrane Collaboration guidelines were followed (23, 24).
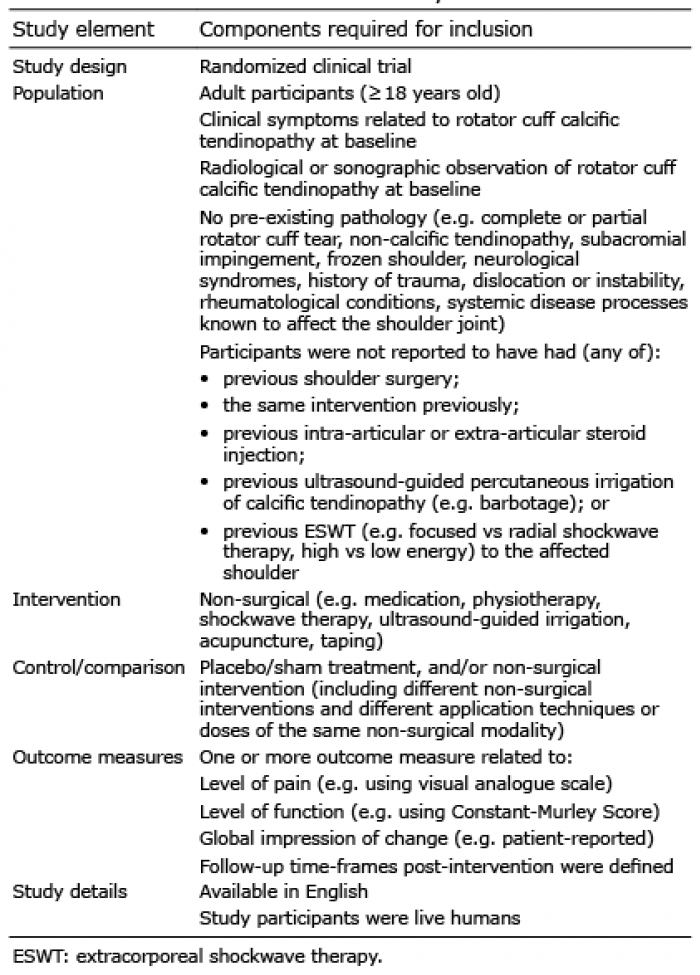
Studies were eligible for inclusion if they complied with all decision rules outlined in Table I.
Table I. Decision rules for inclusion in systematic review
Population
Adult participants (≥ 18 years) diagnosed with symptoms related to RCCT (tenderness near the greater tuberosity of the humerus, nocturnal discomfort and reduced shoulder ROM), confirmed by radiological or sonographic imaging of rotator cuff calcifications (25) were included. Studies were excluded if they reported other pathologies that may confound the aim of the review (e.g. complete or partial rotator cuff tear, non-calcific tendinopathy, subacromial impingement, frozen shoulder, neurological syndromes, history of trauma, dislocation or instability, rheumatological conditions, systemic disease processes known to affect the shoulder joint). Previous shoulder surgery, intra-articular or extra-articular steroid injection, US-PICT (e.g. barbotage), ESWT, or the same intervention modalities applied previously to the affected shoulder were also reasons for exclusion. This was done to include a “naïve” population and to reduce the possibility of delayed effects from previous interventions (Table I).
Intervention/control
Only RCTs of non-surgical interventions were included. This included all uni-modal non-surgical interventions (e.g. ESWT alone) or bi-modal non-surgical interventions (e.g. US-PICT with SAI; ESWT with exercise therapy and NSAIDs) as this reflects common clinical practice (14). Studies that compared different techniques within the same treatment modality (e.g. high-energy ESWT or low-energy ESWT; single or double needle US-PICT) were also included, in order to determine the most effective treatment parameters within each non-surgical modality. Studies including surgical interventions were excluded.
Outcomes
Studies must have reported at least one outcome for pain (e.g. visual analogue scale; VAS) or shoulder function (e.g. Constant-Murley Score; CMS) at any point following intervention.
Data sources
The entire holdings of EMBASE (Ovid), Medline (Ovid), CINAHL (EBSCOhost), Cochrane Register of Clinical Trials, PEDro and SPORTDiscus were searched from inception until 14 March 2018 by 2 independent reviewers (MS and SW). No language, date or publication restrictions were applied. A combination of medical subject headings and free-text were used for the following concepts: calcific tendinopathy, rotator cuff and non-surgical treatments. The medical subject headings used included “calcific”, “calcinosis”, “tendinopathy”, “tendon injuries”, “shoulder”, and “rotator cuff”. The search terms “calcific”, “tendinopathy”, “rotator cuff”, “non-surgical treatment”, “shockwave”, “ultrasound-guided”, “physiotherapy” and their expansions combined in algorithms were also used (Appendix S1).
The reference lists of retrieved articles (including previous systematic reviews) were reviewed for additional studies titles and relevant publications not identified in the search.
Study selection
For final inclusion, articles had to fulfil all the decision rules outlined in Table I. Eligibility was determined independently by 2 reviewers (MS and SW), with differences rectified via consensus discussion or a third independent reviewer (TC), if required. Where full-text manuscripts were not accessible, the corresponding authors were contacted. If there was no reply after 3 attempts, or the full-text was not available, the study was excluded from the review. Where full-texts were not available in English, attempts were made to acquire manuscript translation through the relevant Cochrane Collaboration country branch. If the English translation was not available, the study was also excluded. Following these processes, 3 studies were excluded from the review: full-text only available in German (26); full-text only available in Spanish (27); no full-text available (28).
Data extraction
Data were independently extracted by 2 reviewers (MS and SW) based on the Cochrane data extraction form for RCT intervention reviews (29), and similar data extraction tables used in previous reviews on calcific tendinopathy interventions (16, 19). The study characteristics extracted included information on the target population (age, sex, inclusion and exclusion criteria, sample size), interventions used, outcome measures, study limitations and conclusions (Appendix S5). Follow-up time post-intervention was defined as short-term (ST, 0–12 weeks), medium-term (MT, 13–52 weeks) or long-term (LT, ≥ 1 year) (30). Baseline and follow-up calcific morphology data were also extracted (Gärtner radiological classifications of calcification type 1=clearly circumscribed and dense, formative; type 2 = clearly circumscribed, translucent, cloudy and dense; type 3 = cloudy and translucent, resorptive) (12). Outcomes for participant’s global satisfaction with the intervention were extracted to address the reviews combined aim. Any discrepancies in this process were resolved by discussion between the 2 reviewers, followed by reassessment of the data. A system to resolve any disagreements was established a priori via discussion with a third reviewer (TC), but no such discrepancies occurred.
Risk of bias assessment
Risk of bias was assessed by 2 independent reviewers (MS and SW) using the domain-based Cochrane tool to assess risk of bias for RCTs. This tool has been described previously (31) and was used recently in a rotator cuff related systematic review (30) and frozen shoulder systematic review (32). Domains including random sequence generation, allocation concealment, effective blinding, and whether outcomes were pre-specified, analysed and reported appropriately. Additional methodological issues, such as sample size, co-interventions and compliance relevant to validity or generalizability were also evaluated. Each domain was scored as “yes”, indicating there was evidence to support inclusion of the domain, “no” if this was not included and “unclear” if any uncertainty pertaining to the inclusion of the domain was determined by both reviewers. A score of “yes” was evaluated as low risk of bias, whereas, “no” and “unclear” were evaluated as possible high risk of bias. Each domain was scored independently by both reviewers (MS and SW) and 4 discrepancies emerged that were resolved by discussion. Further discussion with a third reviewer (TC) was not required.
Data extraction and risk of bias assessment procedures were pilot-tested by MS and SW on 3 similar articles prior to the formal review process (33). A Cohen’s kappa coefficient was used to assess inter-rater reliability for judgement of high and low risk of bias for each criterion. The number of agreements was 41/45 (91.1%) with a kappa score of 0.82, and thus the level of agreement was considered strong (34).
Data synthesis
Due to heterogeneity (treatments, dosages, frequencies and outcomes) in the included studies a meta-analysis was not performed. Data were analysed using a best-evidence synthesis (30, 35, 36) and was based on the quality of the included studies. Determination of study quality was decided a priori and was based on previous publications (30, 35, 36).
If the reported findings were consistent across multiple high-quality RCTs the level of evidence would be categorized as strong. If there were consistent findings in one high-quality RCT plus one or more low-quality RCTs, or across multiple low-quality RCTs, the level of evidence would be categorized as moderate. If the reported findings were derived from one RCT (of high or low quality) or were inconsistent across multiple RCTs, the level of evidence would be categorized as limited or conflicting. If there were no RCTs reporting evidence, the level of evidence would be categorized as no evidence.
To provide guidance for clinical practice and inform shared decision-making, the findings of the included studies were grouped as follows; placebo trials (comparisons between non-surgical intervention and placebo/sham), inter-modality comparisons (comparisons between different non-surgical interventions), and intra-modality comparisons (comparisons of the same modality when different parameters; dose, duration, frequency, techniques were investigated).
The electronic database search identified 2,085 articles (Fig. 1). Searches of relevant reference lists did not identify any further articles. After deletion of duplicates, 1,192 articles remained, from which 1,148 were excluded based on title and abstract using the selection criteria. The remaining 44 articles were obtained and read in full; 26 failed to meet the selection criteria (Appendix S2), leaving a total of 18 articles included in the systematic review (Appendix S3).
Fig. 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of study selection.
Characteristics of included studies
Table II details the characteristics of included studies. No studies that investigated exercise therapy for this condition were identified. There were over 1,600 adults diagnosed with RCCT exhibiting symptoms, for a mean between 7 (37) and 33 (38) months, in the included studies. Five different non-surgical interventions for RCCT were investigated: ESWT (low, medium and high-energy flux densities), US-PICT (lavage, puncture, aspiration), pulsed US, AAI and TENS. Study outcomes included; pain, shoulder function, calcific morphology and global satisfaction. The most common outcome measures used were; VAS (39) for pain, and the CMS (40) for shoulder function.
Table II. Characteristics of included studies
Table II. cont.
Table II. cont.
Table II. cont.
Assessment of bias
Fig. 2 presents the overall assessment of the risk of bias and Fig. 3 presents the assessment of the risk of bias for the individual studies (Appendix S41). All 18 papers were assessed as having a high risk of bias. Three of the 18 studies were assessed as high risk of bias for 9 or more of the 15 criteria, while only 3 studies were assessed as high risk for less than 4 of the criteria. The most prevalent shortcomings were found in the items relating to blinding (patient, care provider, outcome assessor), allocation concealment, intention to treat and power analysis.
Fig. 2. Risk of bias graph.
Fig. 3. Risk of bias summary.
Placebo trials
Six studies (41–46) investigated the effectiveness of non-surgical interventions compared with placebo or a control group (Table III). Four of the 6 studies (41, 42, 44, 46) compared non-surgical interventions with a placebo therapy identical in set-up to the intervention group, but without the machine turned on or without gel to conduct the ultrasound waves. One study (45) compared the non-surgical intervention with natural recovery, while one study (43) compared the non-surgical intervention with a control group. This control group received the same baseline therapy (NSAIDs, hotpack, TENS and US) as the intervention group, but did not receive ESWT.
There was moderate evidence (from 2 high-risk of bias trials) to suggest a statistically significant benefit of high-energy ESWT over sham intervention for shoulder function in the short to medium term (42, 46). There was limited evidence (from one high-risk of bias study) favouring the use of pulsed US over placebo for improving pain, function and calcific morphology in the short term (41), and limited evidence (from one high-risk of bias study) showing no benefit of pulsed US in the medium term for pain or function over placebo (41). There was limited evidence (from one high-risk of bias study) showing no benefit of AAI alone (44) or with pulsed US (45) compared with placebo for pain, function or calcific morphology in the short term.
Inter-modality
Three studies (47–49) compared effectiveness between non-surgical treatment modalities (Table III).
There was moderate evidence (from 2 high-risk of bias trials) to suggest a benefit of US-PICT over medium/high-energy ESWT for reduction in pain and calcification size in the long term (47, 48). There was limited evidence (from one high-risk of bias study) favouring the use of ESWT over TENS for pain, function and calcific resorption in the short term (49).
Intra-modality
Ten studies (21, 22, 37, 38, 46, 50–54) evaluated the effectiveness of different intra-modality techniques of non-surgical interventions for RCCT. Seven studies (21, 37, 38, 46, 50, 51, 53) evaluated differences in ESWT techniques, while 3 studies (22, 52, 54) evaluated US-PICT techniques (Table III).
For ESWT, technique variation included: energy flux densities (low-energy < 0.08 mJ/mm2, medium-energy = 0.08–0.28 mJ/mm2, high-energy = 0.28–0.6 mJ/mm2); localization of the transducer (maximum tenderness vs Lithotrack); transducer type (radial vs focused); position of the shoulder during treatment (neutral vs hyperextended and internally rotated); number of impulses; length of treatment session; number of treatment sessions; and co-interventions used (e.g. subcutaneous anaesthetic). There was moderate evidence (from 3 trials of high-risk of bias) to suggest a significant benefit of higher energy ESWT over lower energy ESWT for pain and function in the medium term (37, 38, 46). There was limited evidence (from one high-risk of bias study) favouring radiographically guided ESWT localization (Lithotrack system, Storz Medical Products, Tägerwilen, Switzerland) over using the point of maximal tenderness for pain, function and calcific resorption in the short term (51). There was limited evidence (from one high-risk of bias study) suggesting no difference between 3 sessions of low-energy ESWT and 2 sessions of medium-energy ESWT (50).
Technique variation for US-PICT included: lavage (barbotage) vs puncture; puncture only vs puncture and aspirate; single vs double needle; warm vs room temperature saline; and co-interventions used (e.g. subacromial steroid injection). There was limited evidence (from one high-risk of bias study) to suggest no difference between single- or double-needle US-PICT on clinical outcomes, occurrence of post-procedural bursitis, ease of calcium dissolution, and overall procedure duration (22). There was limited evidence (from onehigh-risk of bias study) showing no difference between puncture-aspiration or puncture only US-PICT on pain in the short and medium term (54).
Side-effects of each modality were minor and infrequent, with the most common being haematomas with higher energy ESWT treatment (42, 46), and up to 5% of vagal reactions with US-PICT (22, 47, 52).
Table III. Results of best-evidence synthesis
Other findings
There is conflicting evidence (from 6 trials of high-risk of bias) for a relationship between calcification size and patient symptoms (pain and function) (37, 42, 47, 50, 52, 53). Del Castillo-Gonzalez et al. (47), Sabeti et al. (50), and Tornese et al. (53) reported greater improvement in pain and function for those who had greater resorption of calcification. Conversely, studies by Hearnden et al. (42), Ioppolo et al. (37) and Sconfienza et al. (52) reported no correlation between calcific morphology and symptoms at follow-up.
The primary aim of this review was to evaluate the effectiveness of non-surgical interventions on pain and function in adults with RCCT. This review revealed moderate evidence that high-energy ESWT was favoured over placebo for shoulder function in the first 6 months (37, 38, 46). There was moderate evidence that higher energy ESWT was favoured over lower energy ESWT for pain and function between 3 and 6 months of treatment. There was moderate evidence that US-PICT was favoured over medium/high-energy ESWT for reduction in pain and calcification size over a 1-year period. Conflicting evidence was found regarding the relationship between calcific morphology and symptoms (pain and function). The outcome measures used in the included RCTs varied between trials and are detailed in Table II.
Regarding pain and function, the results of this review support conclusions reported by Wu et al. (16) and Louwerens et al. (15), that high-energy ESWT is more effective than low-energy ESWT. However, we suggest that, based on the available research, the level of evidence to support this, is moderate. In contrast to systematic reviews by Arirachakaran et al. (19) and Wu et al. (16), no strong evidence was found to support any single non-surgical intervention over another. Instead, the current findings reflect low-quality evidence similar to those reported by Louwerens et al. (15) and Lafrance et al. (18), which synthesized data using direct comparisons between interventions .
Variability within ESWT therapy techniques makes it difficult to determine best-treatment parameters for ESWT with confidence. From the evidence synthesized in this review, higher-energy ESWT (up to 0.44 mJ/mm2) may be more effective than lower-energy ESWT, however this may come with a greater risk of pain and haematomas during and immediately after the procedure (42, 46, 49). Patient expectation of recovery may be associated with the subjective experience of the treatment, taking into account symptoms felt as a direct result of the treatment, such as pain and bruising. Shoulder positioning and techniques for localising the ESWT transducer have also been investigated, but only by individual studies that were deemed high-risk of bias. A hyperextended and internally rotated shoulder position in supine may be more favourable than a neutral shoulder position (53), and ESWT transducer positioning may best be performed using radiographically guided computer technology (Lithotrack System) to target the calcium deposit (51). None of the included studies directly compared focused vs radial ESWT. This is the only systematic review to have compared the different technique protocols used within each intervention modality.
The reported benefit of US-PICT over ESWT for pain and calcification reduction in the long term requires replication in further high-quality studies. Large variations in US-PICT techniques also exist and US-PICT is yet to be compared with placebo. A possible study design could include a blinded placebo group that underwent the same ultrasound-guided needle insertion process without performing irrigation. There appears to be no clinical difference between single- and double-needle lavage, warm and room temperature saline, or between puncture-aspiration and puncture alone. The more minimally invasive techniques of single needle and no aspiration may be preferred. Patients undergoing US-PICT should be monitored for mild vagal reactions, which may occur in up to 5% of patients (47).
There is currently limited evidence to support the use of pulsed US over placebo, and no evidence to support the use of AAI or TENS in the treatment of RCCT. Exercise therapy and physiotherapy-based interventions may be effective; however, they are yet to be examined extensively in the literature. Physiotherapists, doctors and other health professionals currently manage this condition with limited evidence on which to base their management choices. Most of the available research compares minimally invasive interventions, such as ESWT and US-PICT, without considering the place of exercise therapy or natural recovery.
The findings are based on a limited number of low-quality studies. Factors affecting the quality of these studies included: heterogeneity of the studies populations, outcome measures used, follow-up timeframes, and different intervention techniques within each modality; poor methodology and high risk of bias; and the lack of placebo comparison within most studies.
There were substantial differences in the outcome measures used between studies. Twelve of the 18 studies reported data on pain, with 9 using VAS (39). However, only 2 of the 9 studies using a VAS were comparable at the same time-point (37, 50). Similarly, 14 of the 18 papers reported data on shoulder function, 10 used CMS (40), but only one pair of studies could be compared at any given time-point. Furthermore, although both VAS and CMS are validated scoring scales (55, 56), they have acknowledged limitations (40, 57–59).
There was large variation in baseline population characteristics (e.g. duration of symptoms, Gärtner classification and previous intervention exposure). This review attempted to account for previous intervention exposure by excluding studies that reported populations previously exposed to ESWT, US-PICT, steroid injections or surgery. Subjects previously exposed to these treatments may have delayed effects from treatment or present with more resistant forms of RCCT. It is possible that the conclusions of other reviews may have been influenced by including studies in which the participants received additional previous interventions.
Limitations of this review include the potential for publication and language biases. Despite a thorough search of published literature, a search of grey literature was not performed. Studies were required to be available in the English language, either in publication or after attempts to contact authors and relevant Cochrane Collaboration branches for English translation. In addition, since we excluded papers that reported previous exposure of participants to steroid injections, US-PICT, and ESWT, papers where population details were poorly reported may have been included, while papers that more accurately reported previous interventions were left out. Findings from this systematic review should be considered with understanding that there are limitations in both the quality of evidence and the amount of evidence available at present. Clinical interpretation of findings should consider that there are potentially other non-surgical interventions suitable for the treatment of RCCT than those mentioned or examined in detail in this systematic review.
Future research
There is a substantial need for high-quality natural history, clinical, laboratory, imaging and qualitative research to better understand the pathoaetiology of RCCT, relationship between calcification and symptoms, personal impact, and the most effective non-surgical intervention for RCCT. To determine the most effective non-surgical interventions, rigorous RCTs that investigate different applications, doses, frequencies and combinations of interventions for RCCT are needed. Trials must include appropriate placebo and natural history studies.
Recently, a Delphi study was conducted to identify a battery of standardized outcome measures for researchers to include when investigating symptoms associated with tendinopathy (60). Adopting such an approach when investigating RCCT would facilitate a better understanding of effect interventions and permit an appropriate meta-analysis of the results across trials. Until this is available, a minimum set of outcome measures for researchers to consider could include: broad demographic data, the Quick-Dash and/or the Shoulder Pain and Disability Index (61), psychosocial factors including self-efficacy (62), analgesic use, effect on sleep, pain (day, night, duration, intensity, behaviour, region), active and passive shoulder range of movement, strength-resistance tests, co-morbidities and imaging findings.
Conclusion
There was substantial heterogeneity, compounded by poor methodological quality, in the studies that have investigated the effectiveness of non-surgical interventions for RCCT. No strong evidence in favour of any non-surgical intervention was identified. Based on the available research, there is no current evidence for the use of exercise therapy in the management of RCCT. High-energy ESWT appears to be the most effective non-surgical intervention compared with placebo for improving shoulder function in the first 6 months. The use of US-percutaneous irrigation of the calcific deposits may be superior to ESWT for pain and calcification reduction in the long term; however, US-PICT is yet to be compared adequately with placebo. The true effectiveness of non-surgical interventions is difficult to evaluate, due to the lack of placebo comparisons, studies of high risk of bias, and clarity around the large variability in intervention techniques used between studies. Based on our findings there is no certainty that a definitive non-surgical management option currently exists for RCCT. This needs to be carefully and sensitively communicated to those people seeking care whose symptoms are thought to be related to observed calcification in the tendons.


 Click to show fullsize
Click to show fullsize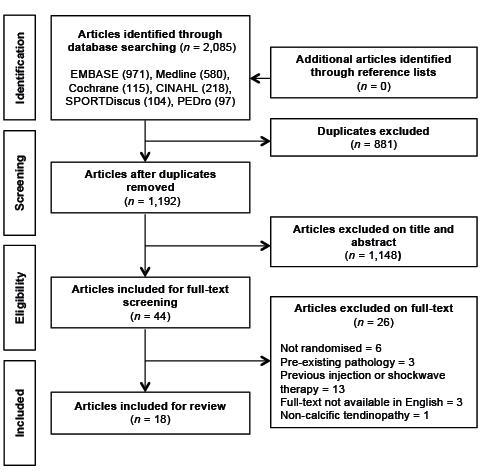 Click to show fullsize
Click to show fullsize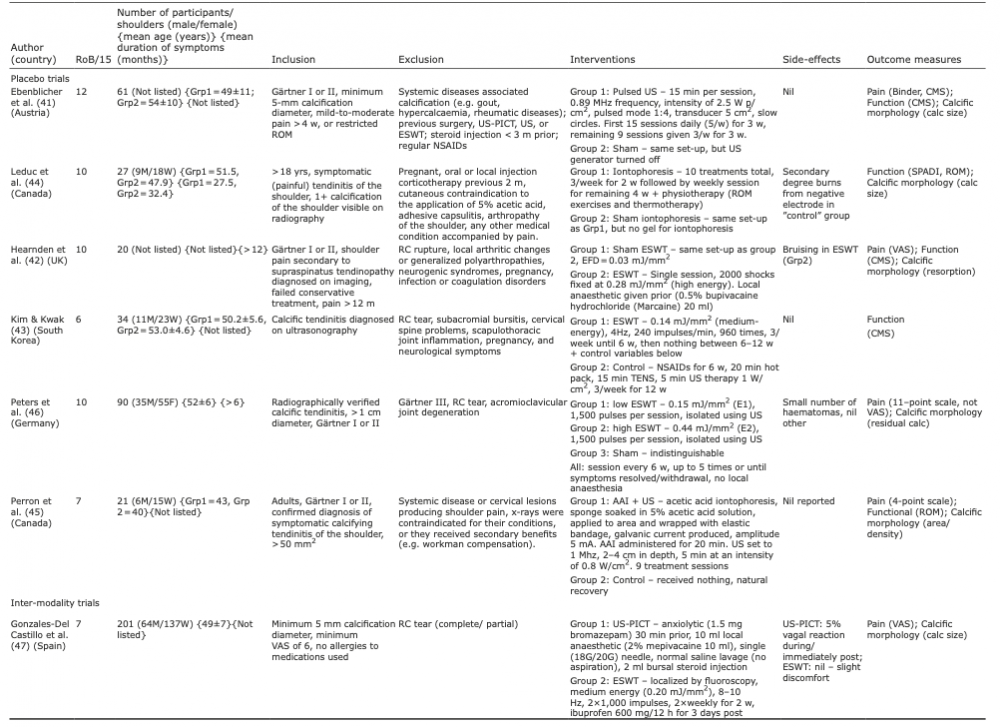 Click to show fullsize
Click to show fullsize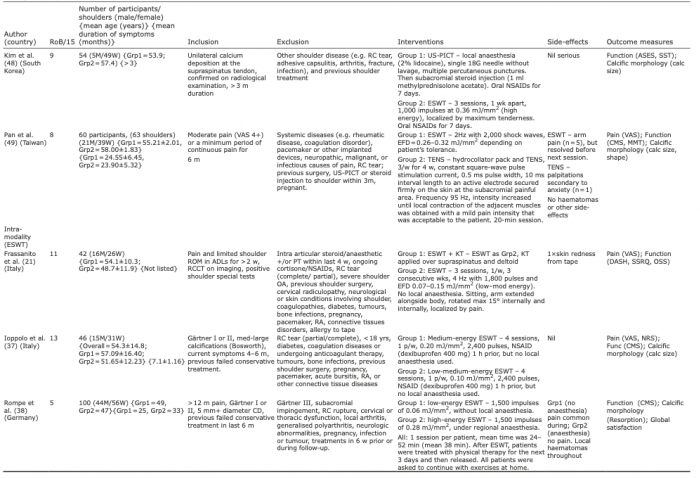 Click to show fullsize
Click to show fullsize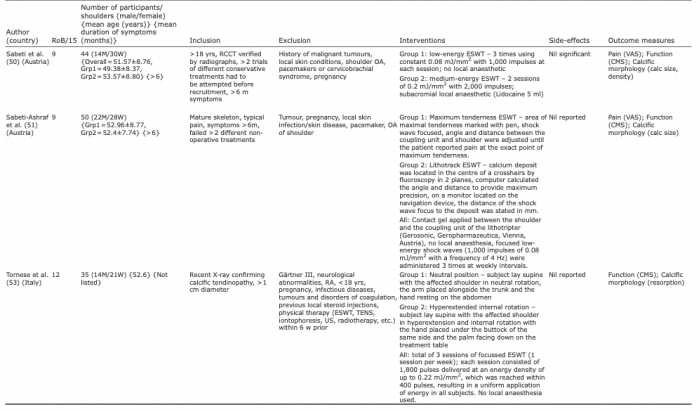 Click to show fullsize
Click to show fullsize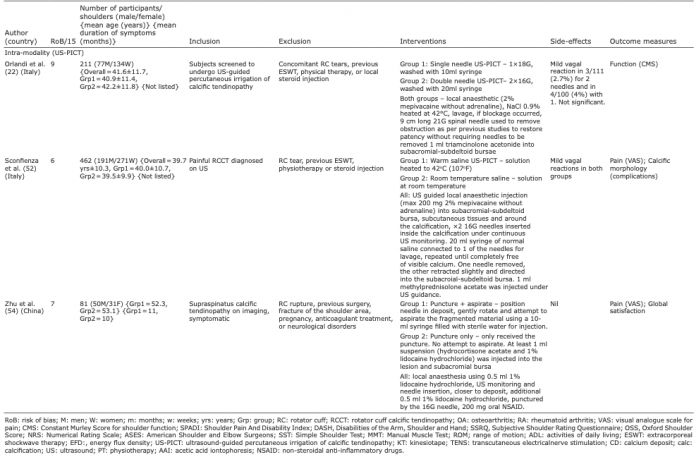 Click to show fullsize
Click to show fullsize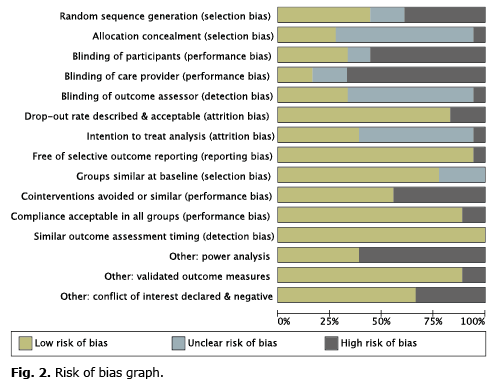 Click to show fullsize
Click to show fullsize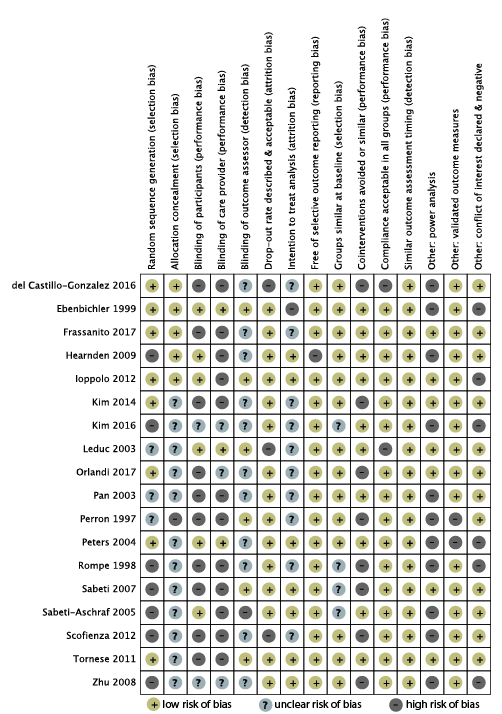 Click to show fullsize
Click to show fullsize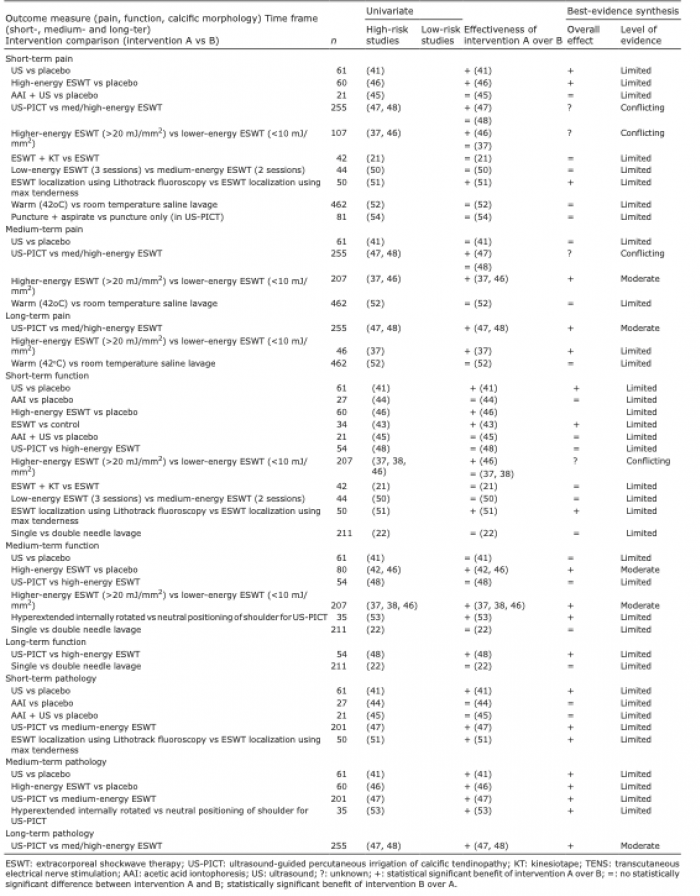 Click to show fullsize
Click to show fullsize