
From the 1Mehiläinen Ympyrätalo, 2National Institute for Health and Welfare, Centre for Health and Social Economics, Helsinki, 3Home Care Physician Services at City of Helsinki, 4National Institute for Health and Welfare, Centre for Health and Social Economics, and Department of Health and Social Management, University of Eastern Finland, Kuopio, Finland
Objective: To compare the costs and monetary benefits of non-pharmacological interventions for patients with Alzheimer’s disease in real-world settings.
Methods: A systematic review was performed to determine the most effective treatment strategies for being able to stay at home for patients with Alzheimer’s disease. Care-management, family support, and multidisciplinary rehabilitation were identified as effective interventions applicable in the Finnish healthcare setting. Data on medical and social service costs, and the costs of residential care for all patients newly diagnosed with Alzheimer’s disease in 2 major cities in Finland were analysed in a 4-year follow-up study. The potential cost savings of the different treatment strategies were assessed.
Results: The annual cost increased from €9,481 to €28,400 (mean per patient) during the 4-year follow-up. Cost savings were achieved in care-management, family support programmes, and rehabil-itative cognitive and social activation if the patients’ transition to long-term care was delayed by 2.8, 1.8 and 43.0 days, respectively.
Conclusion: Care-management and informal caregiver support for patients with Alzheimer’s disease may benefit patients and result in concurrent cost savings. Delaying the decline in cognitive and social functioning through rehabilitation is indicated for more severe phases of Alzheimer’s disease, and the costs appear to be compensated by savings in the cost of long-term care.
Key words: Alzheimer’s disease; care-management; family support; rehabilitation; systematic review; economic analysis.
Accepted Jul 10, 2020; Epub ahead of print Aug 6, 2020
J Rehabil Med 2020; 52: jrm00106
Correspondence address: Antti Malmivaara, Centre for Health and Social Economics, National Institute for Health and Welfare, Mannerheimintie 166, 00270 Helsinki, Finland. E-mail: antti.malmivaara@thl.fi
Doi: 10.2340/16501977-2722
Alzheimer’s disease is the most common reason for institutionalized long-term care in Europe and the USA. The aim of this study was to compare the costs and monetary benefits of non-pharmacological interventions for Alzheimer’s disease in real-world settings, by analysing comprehensive 4-year follow-up data for all new patients with Alzheimer’s disease in the 2 largest cities in Finland. In this systematic review care-management, family support, and multidisciplinary rehabilitation were identified as effective interventions for patients with Alzheimer’s disease. These interventions were found to be cost saving if patients’ transition to long-term care was delayed by 2.8, 1.8 and 43.0 days, respectively. Care-management and informal caregiver support for patients with Alzheimer’s disease appear to benefit patients and result in cost savings for society. Multidisciplinary rehabilitation is indicated for more severe phases of Alzheimer’s disease, and the costs appear to be compensated by monetary savings in long-term care.
Alzheimer’s disease is a major health issue worldwide. It is the most common reason for institutionalized long-term care in Europe and the USA (1, 2). The economic burden of Alzheimer’s disease is estimated to be over 600 billion US dollars worldwide. The majority of costs are typically attributed to long-term care. Alzheimer’s disease and associated behavioural (neuropsychiatric) symptoms may also lead to considerable expense for home-dwelling patients (3–5). Adequate medical treatment can delay transition to institutionalized care (6). However, there is little evidence about the costs and benefits of numerous non-pharmacological treatment strategies that are regularly used to tackle the overwhelming challenge of Alzheimer’s disease.
In Alzheimer’s disease pharmacological treatment (AChE inhibitors and/or memantine) is recommended and can have an effect both on quality of life and the time the patient can stay at home before long-term institutionalized care is necessary (6). Some supervision is always needed when medical treatment is used. If the objective of non-pharmacological treatments is to increase the time spent at home, the focus should be on interventions that are targeted not only at the patient, but also at caregivers and family. Such interventions, even when used for a short time, may bring long-lasting effects. Interventions targeted at the patients themselves can produce long-lasting effects only if the interventions are continuous, since Alzheimer’s disease is progressive, from mild cognitive memory problems to severe dementia (7). Hence, in patient-targeted interventions the most cost-effective way is to combine several interventions during a long time-span. The possibility for caregivers to choose and be actively involved in the interventions seems to be a feature that distinguishes effective non-pharmacological interventions from ineffective ones (8). In addition to the delay in the start of long-term care, other factors, such as quality of life of the patient and caregivers should also be considered in cost-comparison or cost–benefit analyses.
To our knowledge there are no studies comparing the costs and benefits of evidence-based non-pharmacological interventions for home-dwelling patients with Alzheimer’s disease using individual-level data that documents the use of all primary and secondary medical care services and social services.
The aim of this study was to use collected data on the use of health and social care services in Finland by patients with Alzheimer disease, and to estimate potential cost savings as a function of delayed transition to long-term care facilities. Specifically, economic break-even points were estimated for 3 non-pharmacological treatment strategies.
A systematic review was performed to identify treatment strategies that show effectiveness in delaying the need for long-term institutional care. For studies documenting the effectiveness of interventions targeted at patients, clinically relevant outcome measures (i.e. cognition, functional capacity, behavioural symptoms) were sought.
The distribution of medical and social service resource use and costs among patients being diagnosed with Alzheimer’s disease during a 4-year follow-up period were assessed using individual-level data. A dataset that merges the costs of health and social care use among patients diagnosed with Alzheimer’s disease in 2006 in 2 major cities in Finland was used. After evaluating the costs of health service use and long-term care, the cost consequences of the treatment strategies were modelled.
Systematic review
A systematic literature review was performed to identify interventions that would be effective and feasible for use in the Finnish healthcare system. Randomized trials and observational effectiveness studies that had recruited home-dwelling patients with Alzheimer’s disease undergoing non-pharmacological interventions, were included.
Searches were performed for systematic reviews, modelling studies, studies on trends, scenarios and simulations concerning Alzheimer’s disease, dementia, memory disorders and memory impairment. The search strategy included any therapeutics or treatments (pharmacological as well as non-pharmacological) for which the effectiveness of the intervention was evaluated. The databases used were: Health Technology Assessment (HTA); NHS Economic Evaluation Database (CLEED); Database of Abstracts of Reviews of Effects (DARE); Cochrane Database of Systematic Reviews (COCH); CINAHL; PsycInfo; Medline®; OVID 1946 – September week 4 2014; PubMed; and PubMed pubstatusaheadofprint. After removing duplicate results, a total of 2,015 articles/abstracts were analysed.
The abstracts were manually screened for those fulfilling the inclusion criteria. A total of 34 full-text publications were selected from the abstracts and scrutinized in detail. The interventions and outcome measures of these 34 publications were examined. A final total of 3 original studies (10–12) and 4 systematic reviews (8, 13–15) were selected that fulfilled the inclusion criteria. The patient inclusion criteria, interventions, control interventions, outcomes and results of the 3 original studies are shown in Table SI1.
The quality (risk of bias) of the chosen randomized controlled trials (RCTs) was assessed according to the recently updated methodological guidelines of the Cochrane Back and Neck group (16) (Table SII1). The generalizability of the findings was appraised according to previous recommendations (17). The risk of bias in the 2 RCTs (Eloniemi-Sulkava et al. 2009 (10), Pitkälä 2013 (11)) was considered to be low. The risk of bias in the 2008 benchmarking controlled trial by Andren et al. (12) was considered to be high. However, the selection of patients was meticulously described in the study, enabling a good overview of the study populations in the intervention and control groups. The generalizability of findings in all 3 studies (Eloniemi-Sulkava et al. 2009 (10), Andren et al. 2008 (12), and Pitkälä et al. 2013 (11)) was hampered by a lack of reported data on perceived outcomes (Table SIII1).
Real-world data
Study cohort. A cohort of people with Alzheimer’s disease was defined by including all persons who received a clinically verified diagnosis of Alzheimer’s disease in 2006 and, at the time of diagnosis, lived in the cities of Helsinki or Espoo, Finland.
Identification of persons with Alzheimer’s disease was based on 2 criteria; first, the Finnish Special Reimbursement Register maintained by the Social Insurance Institution of Finland was used to identify persons with Alzheimer’s disease. The Special Reimbursement Register contains records of all persons eligible for higher reimbursement due to certain chronic diseases. To be eligible for reimbursement of medicines for Alzheimer’s disease, the diagnosis must be made according to specific criteria (9), and people with a diagnosis of Alzheimer’s disease must have at least some functional impairment due to this memory disease. The medical certificate must have been submitted to the Social Insurance Institution by a physician specialized in neurology or geriatrics. Secondly, the Finnish Social Insurance Institution’s pharmaceutical register was used to verify that the patient had purchased dementia medication. The follow-up period begins on the day of first purchase of dementia medication.
To document the distribution of resource use and costs across different types of residential care services among patients diagnosed with Alzheimer’s disease, unique personal identifiers were used (pseudonymized social security numbers) to link: (i) drug purchases with (ii) the Finnish hospital discharge register, (iii) the Finnish register for income support, (iv) Statistics Finland death register, and (v) the municipalities of Helsinki’s and Espoo’s outpatient registers for medical and social care services.
The ethics committee of the Finnish Institute for Health and Welfare approved the register study.
Modelling
The monetary costs of implementing the following 3 interventions: care-management (10); cognitive, physical and social activation (11); and structured family support programme (12) were evaluated. The distribution of resource use among patients with Alzheimer’s disease in the cities of Helsinki and Espoo was then documented. The data were used to compute a weighted mean daily cost for patients with Alzheimer’s disease who were being treated in long-term care institutions. Finally, the costs and benefits were compared by estimating the costs of implementing the selected non-pharmacological treatment strategies as a function of delay in transition to long-term care. In particular, economic break-even points were estimated for the selected interventions in terms of necessary delay in transition to long-term care, given the real use of medical and social services among patients with Alzheimer’s disease. Cost estimates were based on the Finnish unit cost data for health and social care services in 2011.
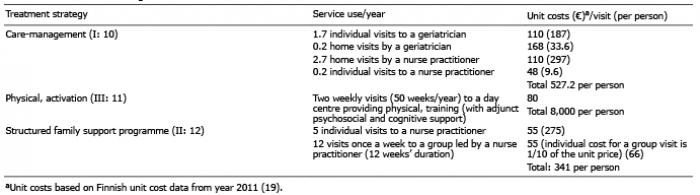
Table I shows the service use and unit costs attributed to the identified treatment strategies. This information was used to estimate the total costs of implementing these selected treatment strategies. Consequently, the estimated annual cost of the care-management programme is €527 per patient, the estimated annual cost of physical, cognitive and social activation is €8,000 per patient, and the estimated annual cost of structured family support programme is €341 per patient.
Table I. Treatment strategies evaluated
Table II shows the categorization used for residential care institutions, services provided in each type of service unit, and the unit costs associated with these service units. Unit costs and the number of days spent in different service categories were used to estimate the residential costs of patients with Alzheimer’s disease at the time of diagnosis and during a 4-year follow-up.
Table II. Services offered and unit costs
Patient characteristics, service use and costs
Patients’ baseline characteristics are shown in Table III. A total of 924 patients had a diagnosis of Alzheimer’s disease. Their mean age at time of diagnosis was 80 years. There were substantially more women (68.2%) than men (31.8%) in the patient population. A minority of patients (38.2%) were living with a partner at time of diagnosis. The most common co-morbidities were arterial hypertension (65.4%) and clinical depression (34.3%).
Table III. Baseline characteristics of the studied patient population
Fig. 1 shows the distribution of service use during the 4-year follow-up period. At the time of diagnosis, 71.9% of patients lived at home without any health-related services being provided at home. One year after diagnosis this proportion had decreased to 52.7%, and the decrease continued throughout the follow-up period. The second largest category of patients at time of diagnosis was home-dwelling patients who received some health services at home. At the time of diagnosis, 17.9% of patients lived at home and received medical care from visiting nurses. This proportion increased rapidly after diagnosis, but remained relatively constant in subsequent years. The proportion of patients living in sheltered housing was relatively small at the time of diagnosis (4.7%), but increased rapidly during the 4-year follow-up. Likewise, the number of patients living in institutionalized care homes was relatively small at the time of diagnosis (4.8%), but increased rapidly during the 4-year follow-up.
Fig. 1. Distribution of use of residential service at the time of Alzheimer’s disease diagnosis and during a 4-year follow-up.
The absolute mean costs of residential service use among patients with Alzheimer’s disease steadily increases over time (Fig. 2). In particular, Fig. 2 shows that the mean costs of residential care among the patients with Alzheimer’s disease were €9,481 at the time of diagnosis and €28,400 4-years after the diagnosis. The increase in the absolute mean costs of residential care among the patients with Alzheimer’s disease was approximately €5,000 per year. The rate of increase stayed relatively steady over time.
Fig. 2. The absolute mean costs of residential service use among patients with Alzheimer’s disease at the time of diagnosis and during 4-year follow-up.
Newly diagnosed patients with Alzheimer’s disease reside in different types of residential settings. Given the documented service use and costs attached to the various services, a weighted mean cost was computed for daily residential care service use among patients with Alzheimer’s disease residing in long-term care facilities (sheltered housing with 24-h assistance, institutionalized care or long-term care in primary healthcare units). The potential cost savings due to implementation of a non-pharmacological treatment strategy were computed by subtracting the cost of implementing the selected non-pharmacological treatment strategy from the total avoided cost of residential care that was obtained by multiplying the mean cost of residential care by the number of days in residential care. Fig. 3 shows the potential annual cost savings per patient with Alzheimer’s disease as a function of delayed transition to long-term care facilities. The programmes for care-management, structured family support programme, and cognitive and social activation achieve economic break-even points if a patient’s transition to long-term care is delayed by 2.8 days, 1.8 days, 43.0 days, respectively.
The number of days reported above are the base estimates for potential cost savings, based on unit costs data and real service use among patients with Alzheimer’s disease (Fig. 3). Sensitivity analyses were performed (see Fig. S11 and Fig. S21), in which the costs of implementing the selected treatment strategies were either halved or doubled. For example, it was observed that doubling the costs of implementing the care-management programme would increase the necessary delay to achieve cost neutrality from 2.8 to 5.6 days.
Fig. 3. Potential annual cost savings or increases per patient with Alzheimer’s disease for selected non-pharmacological treatment strategies as a function of delayed transition to long-term care facilities.
This systematic review shows that care-management, family support, and multidisciplinary rehabilitation (physical, cognitive and social activation) result in better functioning among patients with Alzheimer’s disease. These findings indicate that the interventions help patients and their relatives to adapt to disabilities caused by Alzheimer’s disease.
The modelling performed in this study indicates that the costs of both family support and care-management are minor in comparison with the overall health and social care costs related to Alzheimer’s disease. A delay of more than 3 days in transition to long-term care would reduce the costs (per treatment year) to the health and social care system. The more costly multidisciplinary rehabilitation will be cost neutral if the delay is approximately 45 days per treatment year.
Treatment interventions targeting patients alone may not achieve sustainable results in dementing diseases, due to patients’ decreased memory function and impaired learning abilities. Interventions targeting the patients’ environment and caregivers may have longer lasting effects (10).
Strengths and limitations
Systematic review. Studies that were considered generalizable to the Finnish social and healthcare setting were included in this review. The risk of bias in the 2 RCTs (10, 11) was considered to be low. In the benchmarking controlled trial by Andren et al., 2008, the risk of bias was considered to be higher. However, the selection of patients was well described in this study, allowing good insight into the patient populations in the intervention and control groups. The generalizability of the findings of all 3 studies (10–12) was hampered by the lack of reported data on perceived outcomes. Despite these limitations, the evidence base from these studies was considered appropriate for the purposes of the current review.
Cost analysis. It was possible to access all data on the costs of primary, secondary and tertiary healthcare, as well as social care, in a population consisting of a cohort of all patients diagnosed with Alzheimer’s disease in the 2 largest cities in Finland, with a comprehensive follow-up of costs and service use.
Data regarding primary healthcare services and social care services were obtained directly from the administrative registries of the 2 cities. Data on secondary and tertiary healthcare services were obtained from the Finnish Hospital Discharge Register (FHDR). The coverage and validity of the FHDR data is good (18), while no validation of the administrative data for the 2 cities has been undertaken. The monetary valuation of the 3 interventions was based on a national reference study of various costs within health and social care. This cost valuation reference has been used, for example, in randomized controlled trials conducted in Finland (19).
The analyses in the current study were based on actual use of services. No assumptions were needed. In case of any lack of healthcare data, the actual number of days at home needed to compensate for the costs of interventions would probably be smaller than we have shown.
Clinical, health policy and scientific implications
Early diagnosis and the use of treatments based on current best evidence to maintain functional level and wellbeing of patients and their relatives is the main goal of interventions for patients with dementing diseases. Most patients prefer to live at home, but this should not be at the expense of decreased quality of life. Effective interventions may decrease the need for residential care. These findings of our systematic review indicate that case management and family support interventions could be offered at an early phase of Alzheimer’s disease. Multidisciplinary rehabilitation could be chosen for patients with more advanced disease.
The cost-neutrality method used here is intended for decision-makers to identify interventions that benefit patients and provide economic benefit to society. The method combines evidence of effectiveness from systematic reviews with a cost-comparison analysis.
Further cost comparison analyses, using local register data, are needed. The register data would preferably include clinical baseline information; in particular, data on the severity of Alzheimer’s disease and the proportion of patients obtaining the recommended interventions.
Conclusion
Based on our systematic review, care-management or structured family support may lead to a better quality of life for patients with Alzheimer’s disease and their families, and save health and social care resources. Our economic analysis indicates that widespread implementation of care-management and family support programmes for patients with Alzheimer’s disease and their families may result in substantial savings for society. Increasing cognitive and social functioning is indicated for more severe phases of Alzheimer’s disease, and the costs seem to be compensated by economic benefits in long-term care.
The authors thank Ritva Miikki for performing the literature search. The study was supported by the Finnish Ministry for Social and Health Affairs.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize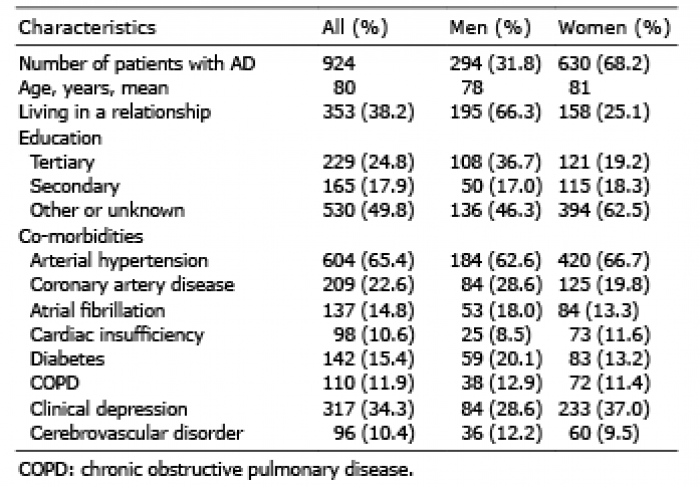 Click to show fullsize
Click to show fullsize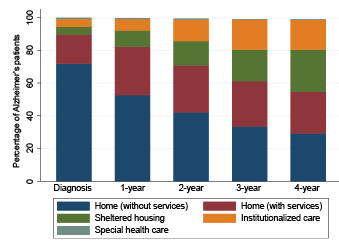 Click to show fullsize
Click to show fullsize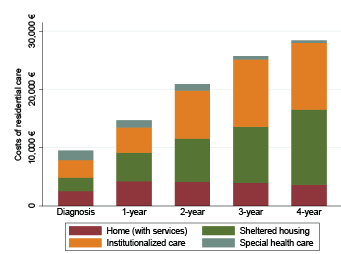 Click to show fullsize
Click to show fullsize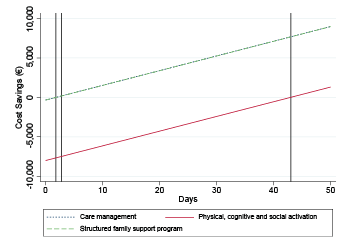 Click to show fullsize
Click to show fullsize