
From the 1Department of Rehabilitation and Functional Recovery, 2Department of Cardiothoracic and Vascular Diseases, 3IRCCS San Raffaele Scientific Institute, 4Department of Neurosurgery and Gamma Knife Radiosurgery, IRCCS San Raffaele Scientific Institute, Vita-Salute San Raffaele University, 5Department of Neurology and Clinical Neurophysiology, IRCCS Ospedale San Raffaele e University “Vita e Salute” San Raffaele, Milan, Italy
Objective: The COVID-19 pandemic has caused significant motor, cognitive, psychological, neurological and cardiological disabilities in many infected patients. Functional rehabilitation of infectious COVID-19 patients has been implemented in the acute care wards and in appropriate, ad hoc, multidisciplinary COVID-19 rehabilitation units. However, because COVID-19 rehabilitation units are a clinical novelty, clinical and organizational benchmarks are not yet available. The aim of this study is to describe the organizational needs and operational costs of such a unit, by comparing its activity, organization, and costs with 2 other functional rehabilitation units, in San Raffaele Hospital, Milan, Italy.
Methods: The 2-month activity of the COVID-19 Rehabilitation Unit at San Raffaele Hospital, Milan, Italy, which was created in response to the emergency need for rehabilitation of COVID-19 patients, was compared with the previous year’s activity of the Cardiac Rehabilitation and Motor Rehabilitation Units of the same institute.
Results: The COVID-19 Rehabilitation Unit had the same number of care beds as the other units, but required twice the amount of staff and instrumental equipment, leading to a deficit in costs.
Discussion: The COVID-19 Rehabilitation Unit was twice as expensive as the 2 other units studied. World health systems are organizing to respond to the pandemic by expanding capacity in acute intensive care and sub-intensive care units. This study shows that COVID-19 rehabilitation units must be organized and equiped according to the clinical and rehabilitative needs of patients, following specific measures to prevent the spread of infection amongs patients and workers.
Key words: COVID-19; rehabilitation; clinical organization; pandemic.
Accepted Jun 8, 2020; Epub ahead of print Jun 9, 2020
J Rehabil Med 2020; 52: jrm00073
Correspondence address: Elise Houdayer, Department of Rehabilitation and Functional Recovery, IRCCS San Raffaele Hospital, via Olgettina 60, 20132, MI, Milan, Italy. E-mail: houdayer.elise@hsr.it
Many patients admitted to hospitals for Coronavirus Disease 2019 (COVID-19) can suffer from various disabilities, such as cardiorespiratory, motor, cognitive, psychological or neurological. These patients need to benefit from rehabilitation during their hospital stay, even when they are still presenting clinical signs of the infection. It is thus of high importance to set-up specialized rehabilitative units for COVID-19 patients. The San Raffaele Hospital of Milan (Italy) created a Unit for rehabilitation of infectious COVID-19 patients. Here, we described the organization needs and costs of such Unit and compared it with the organization and costs of two other rehabilitation Units, already previously in place in the hospital: the Cardiologic and the Motor Rehabilitation Units. We showed that the COVID-19 Rehabilitation Unit had as many care beds as the other units but required twice the amount of workers and equipment, leading to a cost twice superior to the other Units.
The pandemic of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), also termed coronavirus 2019 (COVID-19), has created a new group of patients with specific medical issues. World healthcare systems are concentrating their efforts on intensive care units (ICU) and sub-intensive medical care. However, more than 20% of sub-intensive and 50% of ICU patients require respiratory, motor or cognitive rehabilitation after the acute stage of the disease (1–7). Moreover, patients can still present with positive swabs from 15 to 40 days after the onset of symptoms (1). Thus, several hospitals, including our institution (San Raffaele Scientific Institute, Milan, Italy), started creating COVID-19 rehabilitation departments. It has been estimated that approximately 30% of hospitalized COVID-19 patients need rehabilitation for functional impairment (2). Advanced age and pre-existing conditions are risk factors for this functional decline (1, 2, 8). COVID-19 rehabilitation units can help to increase the number of hospital beds for post-acute care, and thus free up acute beds in intensive or semi-intensive care units for the treatment of COVID-19 or non-COVID-19 patients (in the descending phase of the infection) (3, 4, 8).
Rehabilitation of infectious patients who are still positive for COVID-19 requires complex management regarding hospital facilities, the configuration of medical and nursing staff, together with the availability of personal protective equipment (PPE) (3–11). Since the beginning of the clinical emergency, the functional rehabilitation of COVID-19 patients, especially those admitted to the ICU, has shown the need for a very high level of clinical assistance. Indeed, these patients do not present only with respiratory dysfunctions, but also with cardiological, nutritional, internal and neurological impairments, together with motor difficulties caused by prolonged immobilization (3, 5, 6, 9, 10). Many patients have dysphagia after protracted intubation. Electromyography, pulmonary and heart ultrasound should be performed to monitor the evolution of the disease (3, 5, 8, 12).
To prevent COVID-19 patients from being rehabilitated in many different hospital departments, a COVID-19 Disease Unit was established at San Raffaele Hospital, Milan, Italy (5, 9).
Despite the criteria described above, there is no organizational and cost-analysis description of the infectious COVID-19 rehabilitation units. The aim of this study is to analyse these aspects by comparing the 2-month activity of the newly created COVID-19 rehabilitation unit with 1-year with the previous year’s activity (2019) activity of the Cardiac Rehabilitation and Motor Rehabilitation Units of San Raffaele Scientific Institute, Milan, Italy.
The Italian health system and the Lombardy region recognize 3 different types of rehabilitation, according to the intensity of care, with related economic reimbursement to the hospital facilities: (i) high-complexity rehabilitation treats neurological disorders, such as post-stroke, traumatic brain injury, or spinal cord injury; (ii) medium-complexity rehabilitation treats cardiological, orthopaedic and post-infectious patients; (iii) low-complexity rehabilitation treats chronic conditions. COVID-19 rehabilitation units are classed as medium-complexity units.
The San Raffaele Scientific Institute has several multidisciplinary functional rehabilitation wards, including a Motor Rehabilitation Unit, a Cardiac Rehabilitation Unit and a Specialized Rehabilitation Unit. During the COVID-19 pandemic, the institute transformed the Specialized Rehabilitation Unit into an infectious COVID-19 Rehabilitation Unit. Admission criteria for the COVID-19 Rehabilitation Unit were: positive SARS-CoV-2 testing; low flow oxygen therapy (2–4 l/min); absence of fever for at least 4 days; and a functional motor score showing areas of dependence (Functional Independence Measure, FIM, score < 100).
When patients became non-infectious during their stay in this unit (2 negative swabs at 24 h intervals), they were either transferred to another rehabilitation unit (COVID-19-free) or discharged home, depending on their clinical status and need for continuing rehabilitation.
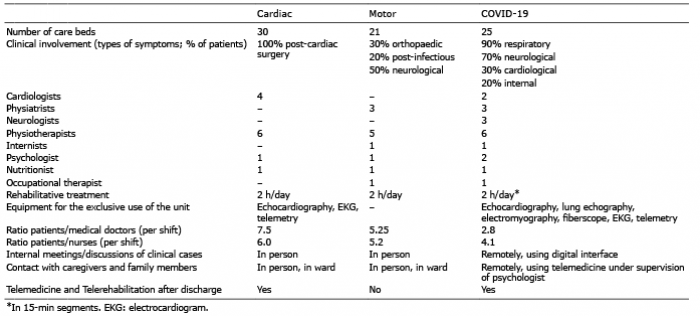
To maintain isolation from each other and from the non-COVID-19 patients, patients were kept in individual rooms, in a single ward comprising 25 beds (4). To provide diagnostic facilities dedicated to COVID-19 patients only, and to prevent continuous transfers within the hospital, the COVID-19 Rehabilitation Unit was supplied with an ultrasound machine (to perform echocardiography and pulmonary echography), an electromyography device, and a fiberscope to test swallowing function (see Table I).
As a consequence, in this new ward dedicated to rehabilitation of infectious COVID-19 patients, all diagnostic equipment required for patients’ testing was kept in the ward and carefully desinfected after each use. Instruments were used at patient’s bedside according to patients’ needs and symptoms.”. No statistical analyses were performed. This is a descriptive report.
Table I. Summary of the organization of the 3 rehabilitation units. Clinical involvement represents patients’ symptoms, expressed as a percentage of the total of patients admitted to the rehabilitation unit. Rehabilitative treatment includes motor, cognitive and speech rehabilitation
The COVID-19 Rehabilitation Unit comprised a higher number of healthcare professionals and a lower number of beds than the other rehabilitation units in the pre-COVID-19 period. The staff was organized to respond to the needs of these patients, and comprised a multidisciplinary team of 3 neurologists/neurosurgeons, 3 physiatrists, 2 cardiologists, 2 medical internists, 2 psychologists, 6 physiotherapists, 1 nutritionist, and 1 occupational therapist (3, 5). Due to the high nursing load in caring for COVID-19 patients, 6 nurses per shift were needed (for 12 h shifts). All members of staff were dedicated full-time to this unit to prevent workers moving between units, and hence reduce the risk of contamination. As in the Cardiac and Motor Rehabilitation Units, patients underwent physiotherapy for 2 h a day, divided into 15-min segments due to the patients’ poor tolerance of physical stress.
By comparison, the Cardiac Rehabilitation Unit consisted of 30 care beds, with 4 cardiologists, 6 physiotherapists, 1 psychologist, and 1 nutritionist. The Motor Rehabilitation Unit consisted of 21 beds, with 4 physiatrists, 5 physiotherapists, 1 psychologist, 1 nutritionist, and 1 occupational therapist. All medical, physiotherapy, and nursing staff were equipped with adequate PPE for each shift (4).
The mean duration of hospital stay was similar between the 3 units (15 days for the COVID-19 Rehabilitation Unit vs 12 and 14 days for the Cardiac and Motor Rehabilitation Units, respectively). No statistical analyses were performed.
The Motor and Cardiac Rehabilitation Units reported a 2019 a positive budget marin of +20.72% and +22.5%, respectively. Conversely, in the first 2 months, the COVID-19 Rehabilitation Unit presented a deficit of –51.8%. The the largest items of expenditure consisted of the medical/nursing staff and the diagnostic tests. The cost analysis is summarized in Table II.
Table II. Cost analysis of the 3 rehabilitation units
The rehabilitation of infectious COVID-19 patients represents a new clinical and organizational type of rehabilitation. From the clinical viewpoint, rehabilitation of COVID-19 patients requires critical medical assistance, and these patients have higher diagnostic and therapeutic needs than non-COVID-19 rehabilitative patients (3, 5, 6, 9, 10, 12 ,13). Regarding the organizational issues of managing these patients in dedicated rehabilitation units, this required an increase in the number of healthcare workers, reduced the number of patients that could have been treated in the same period, and increased costs, resulting in a total cost twice that of the other rehabilitation units in this study. These factors are paramount in this pandemic: the greater the number of rehabilitation beds, the higher the possibility of admission for these patients who are suffering from a severe disease (13). Healthcare systems must reconsider and improve the management of COVID-19 rehabilitation and funding. Furthermore, if there is a new increase in cases of COVID-19, the rapid reorganization of hospital facilities must include setting up dedicated SARS-CoV-2 rehabilitation units with the same urgency as ICU units (5). Failure to consider the complexity of this new clinical entity could rapidly reduce the availability of beds and therefore increase the morbidity and mortality of this viral epidemic, due to the impossibility of delivering appropriate medical assistance to every patient (13). Moreover, to date, the reorganization of the worldwide healthcare systems in the current pandemic, has focused only on increasing the capacity in ICU and subacute beds, and has neglected the need to strengthen the rehabilitative offer to these patients. A comprehensive health organization is essential to cope with current and future pandemics, and must include the strengthening and correct organization of rehabilitation as an integral part of the therapeutic process.
The programing of infectious COVID-19 Rehabilitation Units requires organizational analysis of the specific needs of this new clinical entity, not previously provided for in healthcare organizations worldwide (13).
The authors have no conflicts of interest to declare


 Click to show fullsize
Click to show fullsize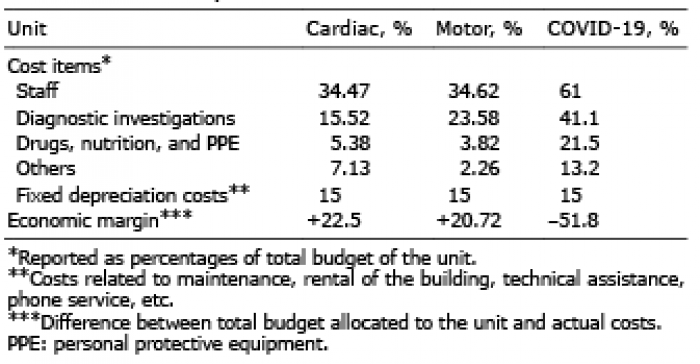 Click to show fullsize
Click to show fullsize