
From the 1Fundació Aspace Catalunya (ASPACE), 2Department of Neurology, Hospital de la Santa Creu i Sant Pau, 3Blanquerna School of Health Science, Ramon Llull University, 4Global Research on Wellbeing (GRoW) Research Group, Ramon Llull University, 5Iberoamerican Cochrane Centre, Hospital de la Santa Creu i Sant Pau-IIB Sant Pau, CIBER de Epidemiología Clínica y Salud Pública, Barcelona, Spain and 6Extracorporeal Shock Wave Research Unit, Chair of Neuroanatomy, Institute of Anatomy, Faculty of Medicine, LMU Munich, Munich, Germany
Objectives: To investigate whether botulinum toxin type A (BTX-A) injection is more effective than radial extracorporeal shock wave therapy in reducing plantar flexor muscle spasticity in subjects with cerebral palsy.
Methods: A total of 68 subjects with cerebral palsy were randomly allocated to BTX-A injection (Group 1) or radial extracorporeal shock wave therapy (Group 2) (first experiment; E1). Outcome was evaluated using the Tardieu V1 and V3 stretches, at 3 weeks, 2 months (M2) and M3 after baseline. At M6 subjects in Group 1 received radial extracorporeal shock wave therapy and subjects in Group 2 received BTX-A injection (second experiment; E2); outcome was evaluated as in E1. Treatment success was defined as improvement in foot dorsiflexion ≥10° when performing the V3 stretch at M2 in both experiments.
Results: In both experiments mean V1 and V3 significantly improved over time. In E1 both treatments resulted in similar treatment success. In E2 fewer subjects treated with BTX-A injection reached the criteria of treatment success than did subjects treated with radial extracorporeal shock wave therapy, which was due to a carry-over effect from E1. No significant complications were observed.
Conclusion: BTX-A injection is not superior to radial extracorporeal shock wave therapy in the treatment of plantar flexor muscle spasticity in subjects with cerebral palsy.
Key words: botulinum toxin type A; cerebral palsy; radial extracorporeal shock wave therapy; rESWT, spasticity.
Accepted May 27, 2020; Epub ahead of print Jun 10, 2020
J Rehabil Med 2020; 52: jrm00076
Correspondence address: Christoph Schmitz, Extracorporeal Shock Wave Research Unit, Chair of Neuroanatomy, Institute of Anatomy, Faculty of Medicine, LMU Munich, D-80336 Munich, Germany. Email: christoph_schmitz@med.uni-muenchen.de
Cerebral palsy is caused by a non-progressive disorder of the immature brain. In most subjects with cerebral palsy spasticity is the main motor disorder. Spasticity of the muscles that pull the foot upward is a particular problem in cerebral palsy, because it can result in disturbances in balance and walking. Botulinum toxin type A (BTX-A) injection is a widely used and effective treatment for spasticity. However, BTX-A is expensive and not available in many countries, and BTX-A injection is an invasive procedure that may cause pain. This study found that BTX-A injection is not superior to non-invasive radial extracorporeal shock wave therapy in managing spasticity of the muscles that pull the foot upward (both treatment modalities were combined with regular conservative therapy consisting of passive mobilization, balance work and coordination). How-ever, radial extracorporeal shock wave therapy is much cheaper and much less painful than BTX-A injection.
Cerebral palsy (CP) is characterized by a persistent disorder of movement and posture, caused by a non-progressive disorder of the immature brain (1). The pooled overall prevalence of CP has been reported to be approximately 2 cases per 1,000 live births in the UK, the USA, India and China (1–3). Most subjects with CP have spasticity as the main motor disorder (1, 4). Spasticity of plantar flexor muscles is a particular problem in CP because it can result in disturbances in balance and walking and interfere with gross motor function (4).
Botulinum toxin type A (BTX-A) is a widely used and effective pharmacological treatment for focal muscle overactivity (2). It specifically inhibits the release of acetylcholine at the neuromuscular junction, thereby reducing muscle spasticity (5). However, BTX-A is expensive and is not available in many countries. Furthermore, injection of BTX-A is an invasive procedure that may cause pain and requires appropriate, effective analgesia (6). With regard to lower extremity post-stroke spasticity, a recent systematic review did not find sufficient evidence to support or refute improvement in walking or quality of life following BTX-A injection (7). Collectively, these issues indicate a need to develop novel approaches for treating lower extremity spasticity in subjects with CP.
Radial extracorporeal shock wave therapy (rESWT) may serve as a non-pharmacological, non-invasive alternative in the treatment of lower extremity spasticity in subjects with CP (e.g. 8–10). During the last 2 decades rESWT has emerged as a non-invasive management option for tendon and other pathologies of the musculoskeletal system, with only a few unwanted side-effects, such as temporary skin redness and discomfort during treatment (11, 12). However, rESWT does not require analgesia, sedation and anaesthesia (13), even in the treatment of lower extremity spasticity in very young children (aged between 12 and 60 months) with CP (10).
Two types of extracorporeal shock waves are used in medical therapy, radial extracorporeal shock waves (rESWs) and focused extracorporeal shock waves (fESWs) (11). Both are single acoustic impulses with an initial positive peak pressure between approximately 11 Megapascals (MPa) (rESWs) (14) and more than 100 MPa (fESWs) (15) reached in less than 1 μs. A recent study has demonstrated the superiority of rESWs over fESWs in the treatment of spastic equinus in subjects with stroke (16).
The aim of the present study was to test the following hypotheses related to the treatment of lower extremity spasticity in subjects with CP: (i) with regard to effectiveness, BTX-A injection (combined with regular conservative therapy consisting of passive mobilization, balance work and coordination) is superior to rESWT (also combined with regular conservative therapy); and (ii) rESWT is less painful than BTX-A injection.
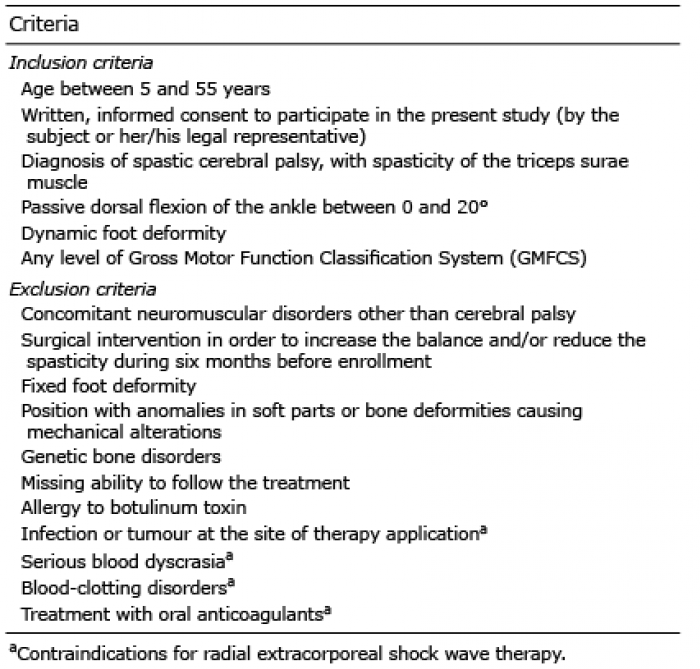
This randomized controlled cross-over study was performed at the Centre Pilot Arcàngel Sant Gabriel of the Associació de Paràlisi Cerebral/Fundació Aspace Catalunya (ASPACE), Barcelona, Spain. A total of n = 70 subjects of any race and ethnicity with CP were assessed between September 2014 and May 2015 for eligibility for enrolment in the study. All the subjects were from Barcelona and other cities in the Catalonia region of Spain. Diagnosis was based on the subject’s history and physical examination at ASPACE. Subjects were considered for participation in the study according to the inclusion and exclusion criteria summarized in Table I.
Table I. Inclusion and exclusion criteria for subjects with spastic plantar flexor muscles due to cerebral palsy enrolled in the study
Ethics committee approval
The study was approved by the ethics committee of ASPACE (number 1638, 24 January, 2014) and carried out in accordance with the World Medical Association Declaration of Helsinki. Subjects or their legal representatives were allowed to withdraw consent term to participate in the study at any time. The study has been registered with ClinicalTrials.gov (Identifier NCT 02400619).
Procedures
Before randomization, a thorough explanation of the various options, as well as the potential risks, benefits and outcomes associated with the various options, took place. Two subjects assessed for eligibility were excluded because they did not meet the inclusion criteria, or the subjects or their legal representatives chose to withdraw or declined to sign the consent form. After having obtained written informed consent from each of the remaining 68 subjects or their legal representatives, they were randomly assigned to receive either a single BTX-A injection (Group 1; n = 33) or rESWT (Group 2; n = 35) in the first experiment (Fig. 1).
Randomization was performed by a person who was not involved in the study, at APACE, using a computerized random number generator. The results of randomization were kept in sealed opaque envelopes, thus allocation was concealed from both subjects and therapists until treatment started. The characteristics of included subjects at baseline are shown in Table II. In case of subjects with bilateral spasticity the leg that was more affected was treated and examined.
In the first experiment (E1) subjects in Group 1 received a single BTX-A injection (BOTOX®; Allergan, Dublin, Republic of Ireland), which was divided into 3 injection sites each of the medial head of the gastrocnemius muscle, the lateral head of the gastrocnemius muscle, and the soleus muscle (total of 9 injection sites) according to the manufacturer’s instructions (total dose between 4 and 10 U/kg body weight). Injections were performed by manual needle placement using anatomical landmarks and palpation (17). No anaesthesia or analgesic drugs were applied during BTX-A injection. Subjects in Group 2 received rESWT with the Swiss DolorClast device (EMS Electro Medical Systems, Nyon, Switzerland) using the EvoBlue handpiece and the 15-mm applicator. Each subject received 3 rESWT sessions (one session per week). Each session consisted of 2000 rESWs applied to the gastrocnemius muscle and the soleus muscle. The positive energy flux density of the rESWs was between 0.10 and 0.12 mJ/mm2, corresponding to an air pressure of 2.2–2.4 bar. The rESWs were applied at a frequency of 8 Hz. No anaesthesia or analgesic drugs were applied during the rESWT sessions. Regular conservative therapy consisted of passive mobilization, balance work and coordination, with one session per week tailored to the individual subject’s needs. Regular conservative therapy was provided throughout the entire study duration, including the time interval between E1 and E2.
Six months later (second experiment after cross-over; E2) the subjects in Group 1 received rESWT as described above for the subjects in Group 2 in E1, and the subjects in Group 2 received a single BTX-A injection as described above for the subjects in Group 1 in E1 (Fig. 1). All subjects received treatment as allocated, and no subject was lost to follow-up. The time interval of 6 months between E1 and E2 was determined based on reports of repeated BTX-A injections in subjects with CP in the literature (c.f. (18)); corresponding data for rESWT had not been published at the time when this study was performed.
The study protocol did not allow blinding of the subjects and the therapists who performed the BTX-A injections and rESWT. On the other hand, the study investigators and evaluators were blinded for the entire duration of the study. Specifically, the study investigators and evaluators did not have access to the subjects’ treatment records, including subject allocation or the allocation sequence, until all subjects had completed the 3-month follow-up examination of the second experiment.
Fig. 1. Flow of subjects in the present study. BTX-A: botulinum toxin type A; rESWT: radial extracorporeal shock wave therapy.
Outcomes
The primary outcome measure was resistance to passive movement of the foot at a slow and fast velocity (Tardieu scale) (19). To this end, passive stretches were separately applied to the gastrocnemius muscle (measured with the knee extended) and the soleus muscle (measured with the knee flexed at 90°) at 2 velocities. The first stretch (V1) was used to determine the angle of muscle reaction at slow velocity, equivalent to the passive range of motion (19). The second stretch (V3) was used to determine both the angle of muscle reaction and the quality of muscle reaction at the fastest possible velocity (19). Measurements were performed with a goniometer at the baselines of both E1 (BLE1) and E2 (BLE2) as well as 3 weeks (W3), 2 months (M2) and 3 months (M3) after both BLE1 and BLE2. The dorsiflexion angle was designated as positive and the plantar flexion angle as negative, considering the neutral position of the joint as 0°.
Treatment success was defined as individual improvement in the dorsiflexion of the foot by at least 10° of the gastrocnemius muscle or the soleus muscle when testing V3 at M2 (separately performed for E1 and E2). Of note, this definition of therapeutic success did not depend on which of the 2 muscles was more affected by spasticity. Based on data reported in the literature (20) and our own experience we expected treatment success in 70% of the subjects in the BTX-A injection group, and in 35% of the subjects in the rESWT group. Considering a 2-sided significance level of 5%, power of 0.9 and equal samples, the power analysis (performed with the online tool, Open Source Epidemiologic Statistics for Public Health (21)) retrieved a minimum number of n = 32 per group to be enrolled in the study.
The secondary outcome was the pain experienced during BTX-A injection or the first rESWT session, respectively (also separately performed for E1 and E2). Pain was assessed using a VAS scale ranging from 0 (no pain) to 10 (maximum, unbearable pain). The mental status of 10 subjects in Group 1 and 8 subjects in Group 2 did not allow valid and reliable information to be obtained about pain experienced during treatment.
Statistical analysis
Statistical analysis was performed on an intention-to-treat basis. However, because all subjects received treatment as allocated and none of the subjects were lost to follow-up, it was not necessary to separately perform statistical analysis for the intention-to-treat population and the per-protocol completers.
Mean and standard error of the mean (SEM) were calculated for all investigated variables. The D’Agostino and Pearson omnibus normality test was used to determine whether the distribution of the investigated variables of the subjects in Groups 1 and 2 were consistent with a Gaussian distribution.
According to Moher et al. (22) no significance tests of baseline differences were performed, except for testing differences in mean V1- and V3-related dorsiflexion of the foot when stretching the gastrocnemius muscle and the soleus muscle between BLE1 and BLE2. This was performed using 2-way repeated measures ANOVA, with the different experiments as within-subject factor and the different groups as between-subject factor.
Treatment-related differences in mean V1- and V3-related dorsiflexion of the foot when stretching the gastrocnemius muscle and the soleus muscle between the subjects in Group 1 and the subjects in Group 2 were also tested with 2-way repeated measures ANOVA, with the different follow-up times (BL, W3, M2, M3) as within-subject factor, and the different groups as between-subject factor. This was separately done for E1 and E2.
Treatment success was tested with Fisher’s exact test. This was also done separately for E1 and E2.
Treatment-related differences in pain between the subjects in Group 1 and Group 2 were tested with 2-way repeated measures ANOVA, with the different experiments as within-subject factor, and the different groups as between-subject factor.
Because the baseline data of V1- and V3-related dorsiflexion of the foot when stretching the gastrocnemius muscle and the soleus muscle were used in 2 statistical analyses, an effect was considered statistically significant if its associated p-value was smaller than 0.025 (0.05 in case of the pain data). Calculations were performed with GraphPad Prism (Version 8.4.2; Graph Pad Software, San Diego, CA, USA).
No apparent differences between the groups were observed at BLE1 (Table II).
Subjects in Group 1 (treated with BTX-A injection in E1 and rESWT in E2) showed no statistically significant differences between BLE1 and BLE2 in mean V1- and V3-related dorsiflexion of the foot when stretch-ing the gastrocnemius muscle or the soleus muscle. In contrast, subjects in Group 2 (treated with rESWT in E1 and BTX-A injection in E2) showed significantly improved mean V1-related dorsiflexion of the foot when stretching the gastrocnemius muscle or the soleus muscle at BLE2 compared with BLE1 (Fig. 2).
Table II. Characteristics of included subjects at baseline (intention-to-treat population)
Fig. 2. Baseline data of the first and second experiments. The panels show Tukey box-plots of (A, B) V1- and (C, D) V3-related dorsiflexion of the foot when stretching (A, C) the gastrocnemius muscle or (B, D) the soleus muscle at the baseline of the first experiment (E1) and the baseline of the second experiment (E2). p-values of 2-way repeated measures analysis of variance are provided at the bottom of the panels. Results of group-specific Bonferroni’s multiple comparison tests are indicated (**p < 0.01). G: group; E: experiment; S: subjects (matching); BTX-A: treatment with botulinum toxin type A injection (open bars); rESWT: treatment with radial extracorporeal shock wave therapy (grey bars). Accordingly, baseline data of subjects in Group 1 are shown in columns E1: BTX-A (first experiment) and E2: rESWT (second experiment), and baseline data of subjects in Group 2 in columns E1: rEWST (first experiment) and E2: BTX-A (second experiment).
In E1 the mean V1- and V3-related dorsiflexion of the foot when stretching the gastrocnemius muscle or the soleus muscle improved significantly over time (Fig. 3). The same effect was found in E2 for the mean V1-related dorsiflexion of the foot when stretching the gastrocnemius muscle and the mean V3-related dorsiflexion of the foot when stretching the soleus muscle (Fig. 4). Furthermore, there was a general (albeit not statistically significant) trend towards better outcome after rESWT than after BTX-A injection in both E1 (Fig. 3E–H) and E2 (Fig. 4E–H).
Fig. 3. Outcome of the first experiment. The panels on the left show Tukey boxplots of (A, B) V1- and (C, D) V3-related dorsiflexion of the foot when stretching the gastrocnemius muscle (A, C) or the soleus muscle (B, D) at baseline (BL) and at 3 weeks (W3), 2 months (M2) and 3 months (M3) after treating subjects with a single session of botulinum toxin type A (BTX-A) injection at BL (Group 1; open bars) or 3 sessions of radial extracorporeal shock wave therapy (rESWT) starting at BL (Group 2; grey bars), respectively. p-values of 2-way repeated measures ANOVA are provided at the bottom of the panels. 95% confidence intervals (Bonferroni) of the differences of group-specific mean data between subjects who were treated with BTX-A injection and subjects who were treated with rESWT are shown in (E–H). TC: time course; Tr: treatment; S: subjects (matching).
Fig. 4. Outcome of the second experiment. Panels on the left show Tukey boxplots of (A, B) V1- and (C, D) V3-related dorsiflexion of the foot when stretching the gastrocnemius muscle (A, C) or the soleus muscle (B, D) at baseline (BL) and at 3 weeks (W3), 2 months (M2) and 3 months (M3) after treating subjects with 3 sessions of radial extracorporeal shock wave therapy (rESWT) starting at BL (Group 1; grey bars) or a single session of botulinum toxin type A (BTX-A) injection at BL (Group 2; open bars), respectively. p-values of 2-way repeated measuresanalysis of variance are provided at the bottom of the panels. 95% confidence intervals (Bonferroni) of the differences of group-specific mean data between subjects that were treated with rESWT and subjects that were treated with BTX-A are shown in (E–H). TC: time course; Tr: treatment, S: subjects (matching).
In E1 both BTX-A injection (Group 1) and rESWT (Group 2) resulted in similar relative numbers of subjects who reached the criteria of treatment success (BTX-A: 12/33 = 36.4%; rESWT: 16/35 = 45.7%; p = 0.469). In contrast, in E2 a statistically significantly lower relative number of subjects who reached the criteria of treatment success was found after BTX-A injection (Group 2; 4/35 = 11.4%) than after rESWT (Group 1; 13/33 = 39.4%) (p = 0.011). A sub-analysis of the data of the subjects in Group 2 at BLE2 demonstrated that compared with the 31 subjects who did not reach the criteria of treatment success (TS-), those 4 subjects who reached the criteria of treatment success (TS+) showed similar mean V3-related dorsiflexion of the foot when stretching the gastrocnemius muscle (TS–: –7.9°; TS+: –6.3°) or the soleus muscle (TS–: –3.2°; TS+: –3.8°), but showed improved mean V1-related dorsiflexion of the foot when stretching the gastrocnemius muscle (TS–: +11.9°; TS+: +18.8°) or the soleus muscle (TS–: +3.7°; TS+: +10.0°), respectively.
In both E1 and E2 BTX-A injection caused approxi-mately twice as much pain as rESWT (Fig. 5).
No significant complications were observed.
Fig. 5. Pain experienced during the treatments. Tukey boxplots of VAS scores reported after the botulinum toxin type A (BTX-A) injections (open bars) and the first radial extracorporeal shock wave therapy (rESWT) session (grey bars) during the first and second experiments. The results of 2-way repeated measures analysis of variance were as follows: pTime=0.296; pTreatment=0.675; pTime × Treatment < 0.001; pSubjects (matching)=0.757. Results of group-specific Bonferroni’s multiple comparison tests are indicated (***p < 0.001).
To our knowledge this is the first report indicating that BTX-A injection (combined with regular conservative therapy) may not be superior to rESWT (also combined with regular conservative therapy) in the treatment of lower extremity spasticity in subjects with CP, thus offering a non-pharmacological, non-invasive and less painful treatment alternative. In general, these results are in agreement with data from a recent randomized controlled trial (RCT) that did not show superiority of BTX-A injection over rESWT in the management of subjects with post-stroke upper limb spasticity (23). The improvement we achieved with rESWT in mean V1 (equivalent to the passive range of motion; (19)) is in line with earlier results we obtained in a case-control study on 34 young children with spastic plantar flexor muscles due to CP, who were treated with 1 rESWT session per week for 3 months plus regular conservative therapy (control: 32 age-matched children treated only with regular conservative therapy) (10). The current results are also in line with data from a RCT in which 16 adults with spastic equinus due to stroke were treated with 1 rESWT session per week for 3 weeks plus regular conservative therapy (control: 15 age-matched adults treated with 1 fESWT session per week for 3 weeks plus regular conservative therapy) (16). To our knowledge, alterations in V3 as a result of rESWT or fESWT for spastic plantar flexor muscles have not been reported in the literature. The improvements we measured with BTX-A injection in mean V1 and mean V3 were in line with data reported in the literature (17, 20).
The current study evaluated treatment outcome with the Tardieu scale, instead of the modified Ashworth scale (24), which was used in most studies on rESWT and fESWT for spasticity published to date (c.f. (10)). In this regard, it is of note that the Taskforce on Childhood Motor Disorders of the U.S. National Institutes of Health (NIH) defined spasticity in 2001 as hypertonia in which one or both of the following signs are present: (i) resistance to externally imposed movement that increases with increasing speed of stretch and varies with the direction of joint movement; and (ii) resistance to externally imposed movement that rapidly increases above a threshold speed of joint angle (25). The Quality Standards Subcommittee of the American Academy of Neurology (QSS-AAN) and the Practice Committee of the Child Neurology Society (PC-CNS) pointed out that, according to a study by Nielsen & Sinkjaer (26), the Modified Ashworth Scale measures a broader set of neural and musculoskeletal factors of non-velocity-dependent hypertonia in addition to spasticity itself (2). According to QSS-AAN and PC-CNS the Tardieu scale is a tool that is more consistent with the proposed definition of spasticity provided by the NIH Taskforce on Childhood Motor Disorders (25).
BTX-A injections were performed by manual needle placement using anatomical landmarks and palpation. This was justified by the fact that a recent RCT found no statistically significant differences between groups for the Tardieu scale when investigating the clinical outcomes of manual needle placement, needle placement guided by electrical stimulation and needle placement guided by ultrasonography for BTX-A injection into the gastrocnemius muscle of a total of 47 adults with spastic equinus after stroke (17). Another study investigated the accuracy of manual needle placement for the gastrocnemius muscle in children with CP who were under the age of 8 years by means of ultrasonography, and found that the needle was accurately inserted into the gastrocnemius muscles in approximately 80% of cases (27). Collectively, these data indicate that the current study would have come to the same conclusion if needle placement for BTX-A injection had been guided by ultrasonography or electrical stimulation. However, this finding must not be generalized. Rather, treatment of other muscles with BTX-A injection, and treatment of young children, may require needle placement guided by ultrasonography or electrical stimulation (6).
Our finding of rESWT-related, statistically significantly improved mean V1-related dorsiflexion of the foot when stretching the gastrocnemius muscle or the soleus muscle even 6 months after baseline (Fig. 2) was unexpected (note that in this regard rESWT was superior to BTX-A injection in the present study). To our knowledge long-term effects of extracorporeal shock waves on spastic muscles have been investigated in only one study to date (28). The authors of this study treated 21 children (age range 3–16 years) with CP and unilateral spastic equinus foot with defocused extracorporeal shock waves (dESWs) generated with an electromagnetic ESWT device (Duolith SD1, Storz Medical AG, Tägerwilen, Switzerland). Each child was treated 5 times with dESWs (1 treatment session per week) with 500 dESWs per treatment session and an energy level of 0.25 mJ/mm2 (which was most probably the total energy flux density). The dESWs were applied at the proximal one-third of the soleus muscle. The authors found a reduction in the elasticity index of the soleus muscle (determined with ultrasound elastography), with a minimum stiffness at approximately the 13th week after baseline and return to baseline data at 25 weeks after baseline (28). There were 2 key differences between this (28) and the current study: (i) isolated treatment of the soleus muscle in (28) vs combined treatment of the gastrocnemius and the soleus muscles in the current study, and (ii) application of 500 dESWs per treatment session in (28) vs application of 2,000 rESWs per treat-ment session in the current study.
This unexpected long-term effect of rESWT on spastic muscles caused a carry-over effect on the subjects in Group 2 in the second experiment of the current study. Of note, this carry-over effect was found in V1-related, but not in V3-related, dorsiflexion of the foot at the baseline of the second experiment (Fig. 2), but apparently had negative impact on the improvement in the V3-related dorsiflexion of the foot when stretching the gastrocnemius and the soleus muscle at 2 months after BTX-A injection (hence the low relative number of subjects in Group 2 in the second experiment who reached the criteria of treatment success). Further studies are warranted to figure out the background of this previously unknown phenomenon. In any case, the design of further cross-over studies on treatment of spastic muscles with BTX-A injection and rESWT must consider that the effects of rESWT may last longer than the effects of BTX-A injection, and that cross-over at 6 months after the start of rESWT may be too early.
The molecular and cellular mechanisms of rESWT on spastic muscles causing a lasting reduction in muscle tone are largely unknown. Taking biopsy samples of spastic muscles after repeated rESWT has not yet been performed and appears to be problematic from an ethical point of view. In an earlier study, Kenmoku et al. (29) exposed the gastrocnemius muscle of Sprague Dawley rats to rESWs using the same rESWT device as in the present study (2,000 rESWs; 15-mm applicator; 4 bar air pressure). The authors found that rESWs induced degeneration of acetylcholine receptors (detected by means of a rhodamine-α-bungarotoxin binding method). In addition, the compound muscle action potential (CMAP) amplitude was significantly decreased immediately after exposure to rESWs compared with unexposed control muscles. This reduction in CMAP amplitude lasted for 8 weeks without delaying latency. The authors concluded that these results suggest a transient dysfunction of nerve conduction at the neuromuscular junction (29). Very recently the same group performed another study on the same animal model and investigated the neuromuscular junction using electron microscopy (30). All rESW-exposed muscles exhibited neuromuscular junctions with irregular end plates. Of note, the mean interjunctional fold interval was significantly increased compared with unexposed control muscles, whereas axon terminals and muscle fibres surrounding the neuromuscular junction with irregular end plates were unchanged (30). Collectively, these results provide a possible mechanism for the effectiveness of rESWT for spasticity. However, other working mechanisms of rESWT on spastic muscles cannot be ruled out.
These results raise the question as to whether the combination of BTX-A injection and rESWT may be superior for treating lower extremity spasticity in subjects with CP than either treatment modality alone. We are aware of 3 studies whose outcomes suggest that this might indeed be the case. One of these studies was an RCT in which a combination of BTX-A injection and fESWT (BTX-A/fESWT; 16 subjects; mean age 64.4 years (standard deviation (SD) 6.1); mean was compared with a combination of BTX-A injection and electrical stimulation (BTX-A/ES; 16 subjects; mean age 63.1 years (SD 7.0)) for treating focal upper limb spasticity after stroke, with better outcome after BTX-A/fESWT than after BTX-A/ES (31). However, this study did not comprise groups of subjects who were treated with BTX-A, fESWT or ES alone. The second study was a pilot RCT on 10 children with lower extremity spasticity due to cerebral palsy who were treated with BTX-A/fESWT (5 subjects; mean age 9.9 years (SD 6.5) or BTX-A alone (5 subjects; mean age 9.6 years (SD 3.4), with better outcome after BTX-A/fESWT than after BTX-A alone (32). However, the sample size in this study seemed too narrow to draw reliable conclusions that could be generalized. A similar study design was applied in a study by Megna et al. (33) (30 subjects with post-stroke spasticity of the biceps brachii, superficial flexor digitorum, gastrocnemius medialis and lateralis muscles, who were either treated with BTX-A/rESWT or BTX-A alone, respectively). However, because of substantial differences in physical load it appears inadequate to mix results achieved on the upper and the lower extremities in the same analysis.
Study limitations
This study has several limitations. First, the sample size was small, and the small number of subjects could potentially confound the clinical results. In particular, the study design was not suitable for testing non-inferiority of rESWT compared with BTX-A injection in the treatment of lower extremity spasticity due to CP. Replication of these findings in large cohorts of subjects with lower extremity spasticity due to CP is therefore important. Secondly, we did not investigate the effects of BTX-A injection and rESWT on gait parameters and daily living activities (such as static and dynamic balance, gait velocity, step length, foot positioning, etc. (20)). Based on the current results we hypothesize that BTX-A injection will also not be superior to rESWT (as performed in this study) in improving these parameters. Thirdly, we neither performed electrophysiological examinations nor took muscle biopsies and, thus, could not investigate potential molecular and cellular mechanisms of reducing muscle tone by rESWs.
Conclusion
This study indicates that BTX-A injection may not be superior to rESWT (as performed in this study) in the treatment of plantar flexor muscle spasticity in subjects with CP. Together with data from a similar study on subjects with post-stroke upper limb spasticity (23) the results indicate that rESWT could generally serve as a non-pharmacological, non-invasive treatment alternative in the management of spasticity.
This study was performed with the radial extracorporeal shock wave device Swiss DolorClast, which is manufactured and distributed by Electro Medical Systems (Nyon, Switzerland). Christoph Schmitz has received research funding at LMU Munich and consulted (until December 31, 2017) for Electro Medical Systems. However, Electro Medical Systems had no role in study design, data collection, data analysis, data interpretation, or writing of the report. All other authors declare no competing interests.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize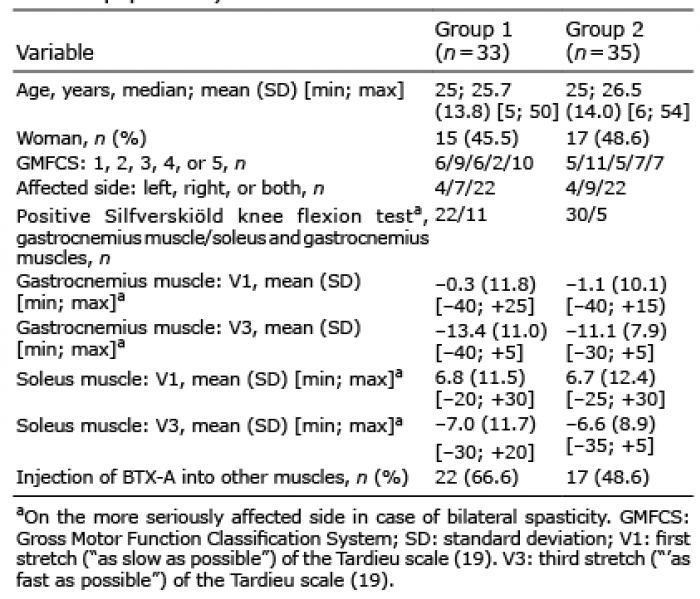 Click to show fullsize
Click to show fullsize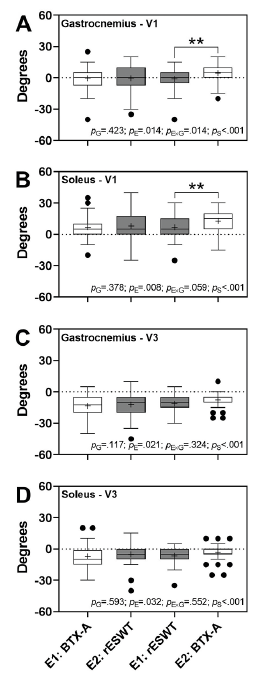 Click to show fullsize
Click to show fullsize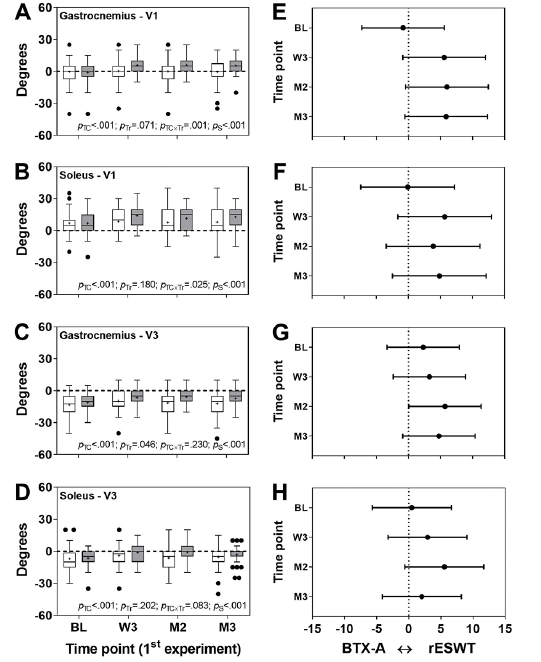 Click to show fullsize
Click to show fullsize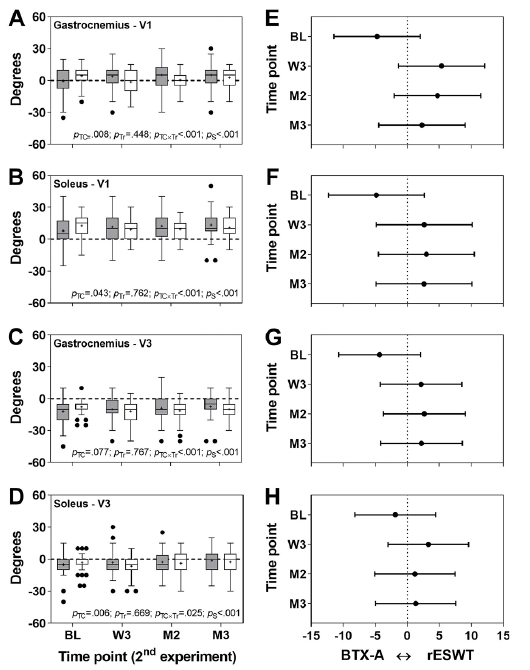 Click to show fullsize
Click to show fullsize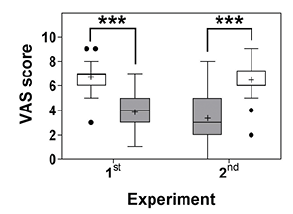 Click to show fullsize
Click to show fullsize