
From the Department of Clinical Sciences, Karolinska Institutet and Department of Rehabilitation Medicine, Danderyd University Hospital, Stockholm, Sweden
Objective: To create and evaluate a preliminary ICF Core Set for myalgic encephalomyelitis/chronic fatigue syndrome using a team-based approach.
Design: Observational study.
Subjects/patients: A total of 100 consecutive patients (mean age 45 years (standard deviation (SD) 9 years)) were assessed by a rehabilitation team and included in the study.
Methods: A preliminary International Classification of Functioning, Disability and Health (ICF) Core Set was created, based on literature studies, and on discussion forums between the team and the researchers. Patients were assessed by a rehabilitation medicine team regarding impairments in body function, activity limitations, and restrictions in participation.
Results: Clinical assessments of the component Body Functions found impairments in energy, fatigue, physical endurance, fatigability, sleep and pain in 82–100% of patients. At least half of the patients had impairments in higher cognitive functions, attention, and emotions, as well as sound and light hypersensitivity, general hyper-reactivity and thermoregulatory functions. For the component Activity/Participation, the most frequent limitations and restrictions were in doing housework (93%), assisting others (92%), acquisition of goods and services (90%), remunerative employment (87%), handling stressful situations (83%), preparing food (83%), recreation and leisure (82%), informal socializing (78%) and carrying out daily activities (77%). The most frequent degrees of impairments/limitations/restrictions assessed were light and moderate, except for remunerative employment, for which restrictions were severe.
Conclusion: Using unconventional methods, this study sets out a preliminary ICF Core Set list for patients with myalgic encephalomyelitis/chronic fatigue syndrome. Further studies are required to improve and test this Core Set in myalgic encephalomyelitis/chro-nic fatigue syndrome populations.
Key words: myalgic encephalomyelitis/chronic fatigue syndrome, ME/CFS; International Classification of Functioning, Disability and Health, ICF; activity; multimodal assessment.
Accepted May 18, 2020; Epub ahead of print May 28, 2020
J Rehabil Med 2020; 52: jrm00074
Correspondence address: Indre Bileviciute-Ljungar, Department of Clinical Sciences, Karolinska Institutet, Danderyd University Hospital, Building 18, 5th Floor, SE182 88 Stockholm, Sweden. E-mail. indre.ljungar@ki.se
*This article has been handled and decided upon by Chief-Editor Henk Stam. Kristian Borg has not been involved in the decision process.
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a disabling condition with no diagnostic or prognostic markers. The patient group is heterogeneous, and impairments in functioning and disability vary between patients. The International Classification of Functioning, Disability and Health (ICF) is a well-established method to assess patient’s functioning and disability. This study sets out a preliminary ICF Core Set for ME/CFS in rehabilitation medicine. However, this requires improvement, and approval by research society and clinicians working with ME/CFS. The introduction of post-exertional malaise as a new category in the ICF should also be considered.
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is characterized by physical and mental fatigue and fatigability, which are not ameliorated by rest. In addition, patients experience widespread diffuse pain and cognitive difficulties that last more than 6 months (1). Patients often report malaise, worsening of symptoms with effort, non-restorative sleep, sore throat, swollen lymph nodes, and other symptoms (2, 3). The prevalence varies depending on the criteria used. For example, the prevalence according to the broad Oxford criteria is 2.6% (4) and 1.2% when Canadian criteria are applied (5). Suffering is described as mild-to-moderate when patients are able to maintain part-time employment, or severe-to-extremely-severe when patients are on 100% sick leave, bedridden or housebound. At least 75% of patients with ME/CFS develop the illness after an infection (6). The cause of ME/CFS is unknown. Few patients recover completely, and curative treatment is lacking (7). From the clinical point of view, diagnosis of ME/CFS is an exclusionary clinical condition when all other possible clinical explanations are rejected or assessed as stable and the fatigue cannot be explained by appropriate specialists (e.g. endocrinologist for hypothyreosis, pain specialist for fibromyalgia/pain syndromes, sleep specialist for sleep disorders, neurologist for head-aches, gastroenterologist for functional gastrointestinal disorders, etc.) (5). Patients with ME/CFS have severe impairments in body functioning; however, no objective or structural findings have been identified as diagnostic or prognostic markers (5). Since there are no objective markers for ME/CFS, there is a great need to classify the symptomatology, to categorize functioning and disability, and to propose standardized measurements with the aim of making research and patient cohorts more understandable and comparable with each other.
The International Classification of Functioning, Disability and Health (ICF) is a classification of health and health-related domains describing functioning and disability (8). The ICF was officially endorsed by all 191 World Health Organization (WHO) Member States in the Fifty-fourth World Health Assembly on 22 May 2001 (resolution WHA 54.21) (8). ICF is the WHO’s framework for categorizing health and disability at both individual and population levels, and is recommended for use in clinical and research practise. As the functioning and disability of an individual occurs within a context, the ICF also includes a list of environmental factors (8). ICF Core Sets have been developed for several (chronic) health conditions (9–14), but, until now, not for ME/CFS.
The primary aim of this study was to create a list of ICF categories for Body Functions, Activities, Participations and Environmental Factors, in order to use it as a preliminary ICF Core Set for patients with ME/CFS. The second aim was to evaluate the Core Set in clinical practice using a team-based approach and to determine the difference between 2 different methods of assessment (test-based vs. observational-based).
Creating an ICF Core Set for myalgic encephalomyelitis/chronic fatigue syndrome
The ME/CFS-project at Danderyd University Hospital started in 2011, with the aim of finding the most appropriate methods of assessment and mix of rehabilitation interventions. Before admitting the patients, literature reviews were performed. Thereafter, the rehabilitation programme was planned, and work on the “ICF Core Set” began. According to the ICF manual, an individual’s disability can be recorded by selecting the appropriate ICF category and its corresponding code, and by adding the qualifier digit that specifies the extent of the reduction in body functions, limitations in the person’s activity and restrictions in participation, and the extent to which an environmental factor is a facilitator or a barrier (8). Categories for the initial ICF Core Set for ME/CFS were chosen according to CDC/Fukuda (1994) (1) and Canadian/Caruthers criteria (2003) (3) (Table I), which are closed to each other, and completed by transforming the results of the evaluation methods into ICF codes, as described below. The following ICF components were evaluated: b-Body Functions, d-Activity and Participation, and e-Environmental Factors. Component s-Structural Factors was not used, since no measurable and specific body macro-structure is known to be impaired in patients with ME/CFS.
Table I. Linking of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) diagnostic criteria to International Classification of Functioning, Disability and Health (ICF) categories
For the clinical practice, a profile of ICF categories was created matching the diagnostic ME/CFS criteria. This profile, a list of ICF categories and a space in which to record the assessed qualifier digit, provided a useful guide to assess each patient’s body functions, activities, participations and environmental factors according to clinical investigations, tests and/or observation (Table SI1). Each ICF category was distributed to professionals within the team, according to their competence profile, and some categories were evaluated by the whole team (Tables II–IV). The degree of impairments/limitations/restrictions was specified using the ICF qualifiers, scored from 0 to 4, corresponding to “none” (0–4%), “mild” (5–24%), “moderate” (25–49%), “severe” (50–95%) and “complete” (96–100%), respectively (8). Environmental factors were used in only approximately half of the patients (due to the absence of a social worker after 2014).
Table II. Impairments in Body Functions according to the International Classification of Functioning, Disability and Health (ICF) b-categories
Table III. Limitations in activities and restrictions in participation according to International Classification of Functioning, Disability and Health (ICF) d-categories
Table IV. Environmental Factors (International Classification of Functioning, Disability and Health (ICF) e-categories
Table V. Overview and suggestion of b-categories for the Brief International Classification of Functioning, Disability and Health (ICF) Core Set for myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS)
Questionnaires for clinical assessment and scoring of the ICF Core Set
A battery of questionnaires was used to assess symptoms related to ME/CFS and functioning/activity/disability. The following questionnaires were used as a part of clinical evaluation: (i) Short-Form 36 (SF-36) is a validated and widely used questionnaire to assess health-related quality of life (HRQoL) (15, 16); (ii) the Swedish version of the Multidimensional Fatigue Inventory (MFI-20) (17); (iii) Hospital Anxiety and Depression Scale (HADS) to determine the levels of anxiety and depression (18); (iv) sleep questionnaires related to diagnosis of restless legs syndrome (RLS) (19) and Epworth Sleepiness Scale (ESS) (20); (v) pain analysis by pain anamnesis, intensity rating by numeric rating scale (NRS) and pain drawings. The results of the questionnaires are not presented, since they were used as a part of clinical assessment.
Additional testing for scoring the ICF Core Set
In addition to clinical and psychological investigations, a number of tests were carried out by team members in order to establish the activity level and to find objective markers for physical fatigue and post-exertional malaise, e.g. repeated submaximal test (Astrand test: a standardized bicycle test to measure aerobic capacity and physical condition) (21, 22); 6-min walk test (6MWT) (23) and Assessment of Motor and Process Skills (AMPS), which is an observation-based assessment providing linear measures of activities of daily living (ADL) motor and ADL process skill ability (24). Full-night polysomnography was performed according to the risk factors for sleep apnoea syndrome (25), and the results were considered when evaluating ICF categories, such as sleep and fatigue. The results of these tests were all taken into account when discussing the diagnosis of ME/CFS, and when evaluating the degree of functional impairments, limitations of activity level and restrictions of participation level in the list of ICF categories for every patient.
Participants, diagnostic procedure and rehabilitation
A total of 100 patients with ME/CFS were recruited from an outpatient rehabilitation programme at the Department of Rehabilitation Medicine, Danderyd University Hospital, ME/CFS-unit, Stockholm, Sweden. The study was carried out during 2011–2015. Diagnosis of ME/CFS was given according to CDC (1) and/or the Canadian criteria (3) during 2011–2013. During 2013–2015 only the Canadian criteria (3) were used, based on suggestions by patient organization and decision-makers. Both medical and psychiatric comorbidities were accepted, as far as they were treated and not judged to be the primary explaining factors for the symptoms presented. The patients underwent laboratory tests to exclude ongoing inflammation, infection, metabolic and immunological disorders and/or other pathological conditions.
During 2011–2013, a multidisciplinary team, consisting of a specialist physician (rehabilitation medicine or neurology), psychologist, physiotherapist, occupational therapist, nurse, and a social worker assessed all patients before confirming the diagnosis of ME/CFS. Diagnosis of ME/CFS was given during a clinical team conference. Multidisciplinary assessment was carried out within approximately 1–2 months. For medical investigation, a specialist physician screened every patient during a 90–120 min visit. In addition, patients met a certified psychologist/neuropsychologist twice for 90 min for psychological evaluation, including a standardized Mini International Neuropsychiatric Interview according to DSM-IV (MINI-D). Several validated tests were also used by the physiotherapist and occupational therapist as a part of team evaluation (Table SI1). Evaluation of the severity of each ICF category was based on clinical investigation, questionnaires and test findings, all of which were performed before rehabilitation. The rehabilitation programme was individually tailored and lasted approximately 6–8 months. In the current study, this approach to ICF assessment is termed “test-based ICF assessment at the start of rehabilitation”. The number of participants was 58.
During 2014–2015, a multidisciplinary team, consisting of a specialist physician (rehabilitation medicine, pain medicine or neurology) and a psychologist performed clinical assessments (90–120 min each) and the diagnosis of ME/CFS was given within approximately 2–4 weeks. The neuropsychological tests were not performed. If the patient fulfilled the diagnostic criteria for ME/CSF, he/she was offered participation in a rehabilitation programme for 6 months. The patients attended approximately once per month during the 6-month rehabilitation programme. The individual part of rehabilitation was followed by weekly phone calls, in order to establish and follow-up the activity level. During 2013–2015, the ICF Core Set was based on the primary clinical assessment and questionnaires and subsequently by observations following the 6-month rehabilitation. It was completed at the end of the rehabilitation programme. In the current study, this approach to ICF assessment is termed “observation-based ICF assessment at the end of rehabilitation”. There were 42 participants.
Devices to assist with ADL were offered to patients, when appropriate, during both periods (2011–2015).
The use of clinical data for scientific analysis was considered by the regional ethics review board in Stockholm (number 2014/300-31) and approved by Danderyd University Hospital (DS2014-0447). Written informed consent was obtained from all participants.
Statistical analysis
Descriptive statistics were used for ICF qualifiers ranging from 0 to 4 (8).
The ICF categories were compared concerning different evaluation approaches (test-based ICF assessment at the start of rehabilitation vs observation-based ICF assessment at the end of rehabilitation). Mann–Whitney U and χ2 tests were used for comparison of these 2 approaches. Only those categories for which significant differences were found using both comparison methods, and for which different median values were found, are presented here.
Statistical package SPSS, version 22 was used for analyses.
The patient population included 17 males and 83 females, mean age 45 years (SD 9). Fifty-three (range 41–53) ICF categories for b-Body Functions and d-Activity and Participation were scored and 51 were included into the analyses. Categories such as vocational training (d825) and higher education (d830) were mostly scored as “not specified” or “not applicable” and were excluded from the analyses, since many patients had already been educated when they developed ME/CFS. Table II presents ICF categories for Body Functions (34 categories), Table III shows results for Activity and Participation categories (17 categories) and Table IV for Environmental Factors (10 categories).
For the component Body Functions (Table II), 88–100% of the patients showed impairments in fatigue- (b1308), sleep- (b134) and energy- (b1300) related domains, including post-exertional malaise measured by the category physical endurance (b4550). Moreover, in more than 75% of patients, impairments were found in pain-related categories (pain sensation, headache and neck pain, b2800 and b28010, respectively) and thermoregulatory functions (b5508). At least half of the patients had attentional (b140), cognitive (b164) and emotional impairments (b152). However, neuro-psychological tests were omitted during 2013–2015 and the percentage of patients evaluated for memory functions was lower. Nevertheless, in those analysed, memory impairments were found in 46 patients vs 17 for memory functions (b144) and in 45 vs 20 for short memory (b1440). This indicates that more than half of patients with ME/CFS tested for memory functions had memory impairments. Frequent impairments were also found for hypersensitivity, both for sound (b2408) and light (b21020), as well as for general body hyper-reactivity (b4351). Immune system-related (b435, b4353, b550), gastrointestinal (b535) and cardiovascular (b460) functions were also impaired in approximately 50% of patients. Body weight (b530), urination (b630) and skin (b830), as well as blood pressure (b420) and capillary (b4151) functions, were impaired in a smaller number of patients (less than 50%). Musculoskeletal functions, such as mobility of joints (b710), muscle power (b730) and muscle endurance (b740), were not assessed in approximately 50% of patients, due to omission of physical tests after 2013 (clinical assessment tests of muscle strength, mobility as well as muscle endurance tests, e.g. 6MWT and submaximal bicycle (Astrand)). The results indicate that, in those who were assessed, categories of muscle power functions (b730) and muscle endurance (b740) were impaired in more than 50% of cases. Fig. S11 presents median of qualifiers of most frequently impaired body functions (over 75% of patients). Median scoring of impairments was 2 (2=”moderate” 25–49% impairment) except for thermoregulatory functions (1=”mild” 5–24% impairment).
For Activity and Participation, the most frequent limitations and restrictions were found in doing housework (93%), assisting others (92%), acquisition of goods and services (90%), remunerative employment (87%), handling stressful situations (83%), preparing food (83%), recreation and leisure (82%), informal socializing (78%) and carrying out daily activities (77%) (Table III). Activities associated with walking functions (d455 and d4501) were not assessed in a proportion of patients, mostly because 6MWT and occupational therapy tests were omitted after 2013. However, those activities were impaired in more than 75% patients assessed. Fig. S21 presents the median of most frequently impaired activity and participation domains (in over than 75% of patients). Median scoring of severity of restrictions was highest for remunerative employment (3=”severe” 50–95% impairment) and varied between 1 and 2 for other categories.
Ten Environmental Factors (range 4–10) were assessed in 42 participants (Table IV). For the Environmental Factors, support (e3) and attitudes (e4) from family and friends were often found to be facilitators, whereas society services, systems and policies (e5) were more often found to be barriers than facilitators (Table IV).
Comparison of 2 different ICF assessment methods (test-based ICF assessment at the start of rehabilitation vs observation-based ICF assessment at the end of rehabilitation) shows differences in 1 b-category and 2 d-categories (Table SII1). Immunological functions (b435) were scored more impaired by observation-based assessment, while basic interpersonal interactions (d710) and informal socializing (d9205) were scored higher by test-based evaluation method (Table SII1).
This is a first attempt to create a preliminary ICF Core Set to evaluate body functions, activity and participation of patients with ME/CFS. According to Canadian diagnostic criteria for ME/CFS (2, 3), 51 ICF categories in b-Body Functions, d-Activities and Participation and 10 e-Environmental Factors were selected. Thirteen of 34 Body Functions and 3 of Activity/Participation were chosen from the tertiary level, which means that a more detailed categorization of the selected domains was used by a rehabilitation team. Eight of 34 ICF b-categories (4 fatigue, 1 sleep, 2 pain and 1 thermoregulatory) were found to be impaired in at least 75% of patients. This corresponds to the clinical symptoms and diagnostic criteria of ME/CFS, since ME/CFS patients report fatigue, post-exertional malaise, non-restorative sleep, feelings of fever, and chronic pain (Table I). Regarding cognitive functions, the most frequent impairment found was attention (in 71% of patients). Eleven of 17 ICF d-categories were restricted in at least 75% of the patients assessed, indicating difficulties in Activities/Participation. Though the degree of impairments varied between mild-moderate, the summarized impairments/limitations/restrictions in 61 ICF categories confirm the complexity of ME/CFS in functioning and disability as well as the interplay with environmental factors. These complex impairments and restrictions affect patients’ daily life, welfare and social life.
In practice, 2 ICF Core Sets are usually developed for international use in healthcare, social welfare, labour activities and research: the Comprehensive Core Set and the Brief Core Set. The Comprehensive ICF Core Set should include as many categories as necessary to be comprehensive, but as few as possible to be practical for the reporting of disability. The Brief ICF Core includes the smallest number of ICF categories that can serve as a minimal standard to be used for the reporting of disability. The Brief ICF Core Set for rehabilitation medicine contains 9 categories from Body Functions, 21 from Activity/Participation and 12 Environmental Factors categories; a total of 32 ICF categories (26). In comparison with the Brief ICF Core Set for rehabilitation medicine, the current ICF Core Set includes mostly the same Body Functions (8 of 9, except for sexual functions (b640)), many Activity/Participation categories (11/21) and some (3/12) Environmental Factors categories (26). Moreover, the preliminary ICF Core Set for ME/CFS includes all 7 ICF categories supposed as a minimal generic set for functioning and health (b130 Energy and drive func-tions, b152 Emotional functions, b280 Sensation of pain, d230 Carrying out daily routine, d450 Walking, d455 Moving around and d850 Remunerative employment) (27). Further studies are encouraged to improve and validate this preliminary ICF Core Set for ME/CFS in other ME/CFS populations and to choose the categories for the Brief and Comprehensive ICF Core Sets for ME/CFS.
Another general issue is how to measure ICF categories in patients with ME/CFS, as many functions are evaluated clinically with few objective tests. In the present study, we have compared 2 different methods of evaluation: one at the start of rehabilitation, based on the clinical evaluations, including objective tests, and one at the end of the 6 months’ rehabilitation period, based on clinical evaluations at the start with no objective tests and during 6 months of observations. Some differences were obtained favouring the test-based assessment vs the observational-based one. However, on the whole we do not believe that this influences the overall results. The category of immunological functions (b435) evaluated by the patient’s sensitivity to infections was scored as more impaired by the observational method. Patients with ME/CFS have increased sensitivity to infections and impaired temperature regulation. It was easier to observe these findings during a longer (observational) period. Participations, such as basic interpersonal interactions (d710) and informal socializing (d9205), were evaluated by a neuropsychological interview and favoured the test-based assessment. However, only informal socializing was impaired in more than 75% of patients, while the remaining 2 categories were impaired in approximately or less than 50% of patients. Taken together, both assessment methods seem to be reliable for the group as a whole, since the majority of the most important impairments for patients with ME/CFS, such as fatigue, sleep, pain, thermoregulation, cognitive functions, etc., did not differ between the 2 different evaluation approaches.
Study limitations
The ICF Core Sets are usually created by a formal consensus process integrating evidence in the literature and gathering expert opinion based on the ICF framework and classification (9–11). Usually, both the Comprehensive ICF Core Set and the Brief ICF Core Set are defined. We created a Preliminary ICF Core Set by limited involvement of experts and clinicians and by using diagnostic criteria for ME/CFS as a starting point. Although the linking of ICF dimensions to the diagnostic criteria of ME/CFS helps in choosing the most important ICF categories, some dimensions might be missed. However, during the period 2011–2015, the ICF categories were continuously checked by the team and adjusted to cover all possible functional impairments, activity limitations and participation restrictions.
Another study limitation is that only patients who were ready for a rehabilitation programme and able to come to the hospital were included in the study. No housebound patients were included. This creates difficulties in drawing general conclusions about impairments in ICF categories in the ME/CFS population as a whole. The third limitation was due to the change of physiotherapist after 2012, which resulted in tests for muscular functions being excluded, and functions such as mobility of joint functions (b710), muscle power functions (b730) and muscle endurance (b740) not being assessed in approximately 50% of patients. However, in those patients who were assessed, the impairments were found in 50–75% of cases. This indicates the importance of assessing ICF categories related to muscular functions in future studies of ME/CFS. The same concerns the absence of both a nurse and a social worker after 2013. A new social worker was employed later on. However, there was no possibility to assess environmental ICF categories, creating difficulties in evaluation of environmental factors. Therefore, environmental factors were not evaluated in a satisfactory way and should be interpreted with care. Despite the fact that several objective tests were used (e.g. full-night polysomnography, manual mouth temperature, blood pressure, and functional tests, such as 6MWT, repeated sub-maximal (Astrand’s) and activity test (AMPS)), one of the major functional impairments affecting ADL in patients with ME/CFS, orthostatic intolerance, was not assessed.
In order to collect objective data in assessing ICF, many physiological parameters, such as blood pressure, weight, daily physical activity, temperature, heart rate activity, etc., can be measured at home using digital devices. Monitoring at home is thought to bring valuable information regarding activity and functioning level and could lead to standardized evaluation of many ICF b- and d-categories in general. This study did not evaluate either the effect of rehabilitation per se, which might influence the ICF categories if it was performed at the end of the rehabilitation period. However, the current clinical report shows few effects of multimodal rehabilitation in patients with ME/CFS, which is in line with studies by Vos-Vromans et al. (28). In addition, the current study did not assess Personal Factors, which have been shown to be important in the outcomes of ME/CFS rehabilitation (29).
Study strengths and further suggestions
The strengths of this study are: (i) it is longitudinal and clinically-adapted (2011–2015); (ii) the length (at least 6–7 months) of observation of patients participating in the rehabilitation programme; (iii) the use of as many objective measurements as possible during 2011–2013; and (iv) the multimodal assessment. Another strength is that the Preliminary ICF Core Set was continuously checked, improved and adjusted in order to optimize it for the clinical setting. Therefore, we suggest the following improvements: (i) only ICF b-categories impaired in at least of 50% of patients with ME/CFS should be chosen; (ii) substitution of some b-categories in order to evaluate them without time-consuming tests, such as neuropsychological tests, which require a trained psychologist; and (iii) using all d-categories suggested, although not all of them were impaired in 50% of patients. It is assumed that d-categories, especially those related to ADL, are significantly impaired in more severely affected (e.g. housebound) patients. This includes dressing (d540), washing (d510) and other ADL. An adjustment of b-categories and an introduction of 3 new d-categories (d350 Conversation, b210 Undertaking a single task and d220 Undertaking multiple tasks) is presented in Table V. This comprises 25 b-category and 20 d-categories; a total of 45 items for b- and d-categories. The research community and clinicians working with patients with ME/CFS should discuss whether to introduce a new b-category for post-exertional malaise in the next version of the ICF. Post-exertional malaise in ME/CFS does not only mean impairments in physical fatigability (b4552) and physical endurance (b4550) or muscle power functions (b730)/muscle endurance (b740). Clinically, post-exertional malaise means a relationship between the amount of load (physical, cognitive or social) and the magnitude/duration of worsening in ME/CFS symptoms after the applied load. Post-exertional malaise is evaluated clinically, since there are no tests or validated questionnaires (30).
Conclusion
This is the first presentation of a preliminary ICF Core Set for ME/CFS, showing significant functional impairments, activity limitations and participation restrictions in many of the ICF categories measured. Further studies are needed to validate this ICF Core Set in other ME/CFS clinical settings, such as primary, secondary and tertiary care, including housebound patients. Monitoring of patients with ME/CFS at home should be the next step in improving the assessment of functioning and disability and might contribute to the operationalization of ICF categories.
The authors thank Per Julin, MD PhD, and physiotherapist Philippe Njoo, who initiated this ICF project in 2011, as well as the ME/CFS team at the Department of Rehabilitation Medicine, Danderyd University Hospital, Stockholm, who contributed to assessments during 2011–15.


 Click to show fullsize
Click to show fullsize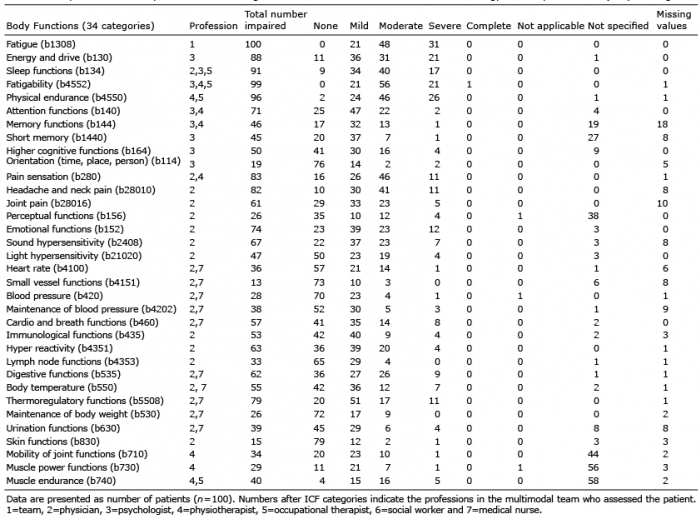 Click to show fullsize
Click to show fullsize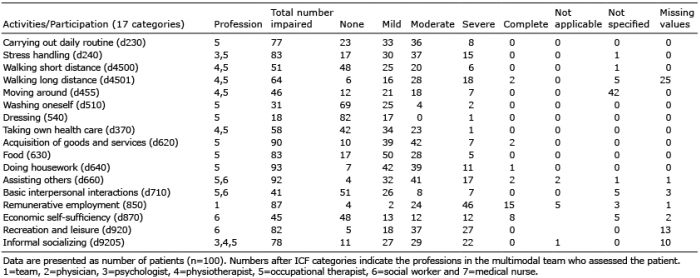 Click to show fullsize
Click to show fullsize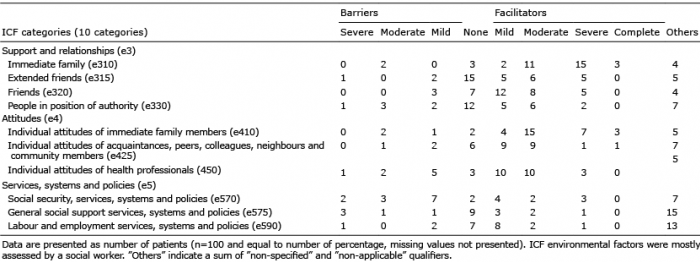 Click to show fullsize
Click to show fullsize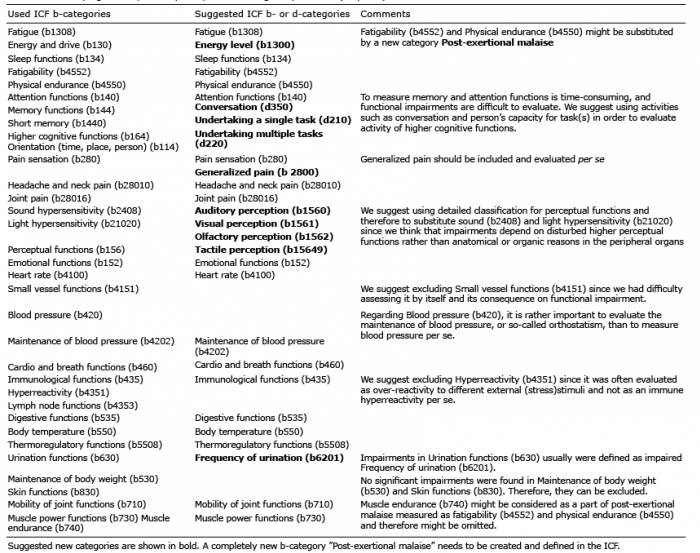 Click to show fullsize
Click to show fullsize