
From the 1Division of Pediatric Neurology, Department of Women’s and Children’s Health, Karolinska Institutet, 2Allied Health Professionals Function Medical Unit Occupational Therapy and Physiotherapy, Karolinska University Hospital, 3Motoriklab, Department of Women’s and Children’s Health, Karolinska Institutet, 4Department of Pediatric Radiology, Karolinska University Hospital, 5Clinical Pediatrics Unit, Department of Women’s and Children’s Health, Karolinska Institutet, 6Department of Physical Performance, Norwegian School of Sport Sciences, Oslo, Norway, 7Department of Pediatric Orthopedic Surgery, Karolinska University Hospital, and 8Department of Laboratory Medicine, Division of Clinical Physiology, Karolinska Institutet, and Unit of Clinical Physiology, Karolinska University Hospital, Stockholm, Sweden
Introduction: The development of efficient resistance exercise protocols to counteract muscle dysfunction in cerebral palsy is warranted. Whether individuals with cerebral palsy are able to perform iso-inertial resistance (flywheel) exercise in a comparable manner to typically developed subjects has never been experimentally tested.
Design: A comparative, controlled study.
Subjects: Eight young ambulatory adults with cerebral palsy (mean age 19 years; Gross Motor Function Classification System (GMFCS) I–III) and 8 typically developed control subjects (mean age 22 years).
Methods: Subjects performed acute bouts on the weight-stack and flywheel leg-press device, respectively. Range of motion, electromyography, power, work and muscle thickness (ultrasound) data were collected.
Results: Subjects with cerebral palsy were able to produce a greater eccentric/concentric peak power ratio on the flywheel (p < 0.05 vs ratio in weight-stack), however absolute values were lower (p < 0.05 vs weight-stack). Typically developed subjects produced more power per mm of thigh muscle than the cerebral palsy group, independent of leg, device and action.
Discussion: Subjects with cerebral palsy could not elicit the eccentric overload seen in typically developed subjects. Furthermore, peak power production per mm muscle was markedly reduced in both legs in subjects with cerebral palsy. In conclusion, this comparative study of weight-stack and flywheel exercise does not support the implementation of the current iso-inertial protocol for young adults with cerebral palsy.
Key words: cerebral palsy; resistance exercise; eccentric overload; muscle thickness; ultrasound; electromyography.
Accepted Apr 15, 2020; Epub ahead of print Apr 21, 2020
J Rehabil Med 2020; 52: jrm00060
Correspondence address: Ferdinand von Walden, Division of Pediatric Neurology, Department of Women’s and Children’s Health, Karolinska Institutet, Stockholm, Sweden. E-mail: Ferdinand.von.walden@ki.se
Cerebral palsy is an umbrella term for a movement disorder in children and adults, which is caused by damage to the immature, developing brain. Individuals with cerebral palsy have weaker, thinner and stiffer muscles compared with individuals without cerebral palsy. Poor muscle function makes everyday activities harder. Efficient training regimes to improve muscle function are therefore needed. This study investigated whether an alternative form of resistance exercise (iso-inertial exercise) was feasible in individuals with cerebral palsy. The results show that iso-inertial exercise was difficult for individuals with cerebral palsy to perform and is probably unsuitable for clinical practice for this specific population.
Cerebral palsy (CP) is the most prevalent motor disorder in children (1). Although initiated by a non-progressive brain lesion before the age of 2–3 years (2), clinical manifestations and functional impairments usually worsen over time. Individuals with CP show weaker, thinner and stiffer skeletal muscle than typically developed (TD) children (3), and have decreased muscle volume in affected limbs (4). Poor muscle quality is believed to contribute substantially to the reduced functional capacity typically seen in this population.
Although resistance exercise (RE) programmes can result in increased strength in individuals with CP (5), evidence of transfer effects on functional mobility are lacking (5, 6). This lack of transfer effects may be explained by the concept of training specificity which incorporates the mismatch of selective neuromuscular control, speed of movement, and loading stimulus of currently employed RE models relative to functional activities. Indeed, Damiano and co-workers (7) have shown that individuals with CP have difficulty activating their muscles during concentric (CON; shortening) compared with eccentric (ECC; lengthening) muscle actions to generate force. Despite this finding, published more than 15 years ago, the vast majority of RE protocols currently used in clinical practice still use traditional isotonic, weight-stack (WS) devices that provide a sub-optimal load during the ECC action (8). This is rather surprising, considering the importance of high-intensity ECC actions to boost efficacy of training (9).
Contrary to gravity-dependent isotonic RE protocols, the flywheel (FW) iso-inertial technology (10) allows for maximal intensity during the entire range of motion of the CON action, and with the appropriate technique (11), brief episodes of ECC overload (i.e. greater force/power production during ECC vs CON). Flywheel RE has been proven effective to counteract the negative effects of unloading on skeletal muscle (12, 13), and, compared with traditional WS, FW RE induces greater muscle hypertrophy in TD subjects (14, 8). In a recent clinical trial with stroke patients, who, similar to individuals with CP, present more preserved ECC vs CON force (15), FW RE training induced robust and positive muscle (i.e. hypertrophy, force, power) adaptations (16). Yet, differences in aetiology of the motor impairment and patient characteristics between stroke and CP warrant specific investigations testing the viability, safety and efficacy of FW RE in individuals with CP.
Individuals with unilateral CP have lower muscle mass and isometric strength on the more-affected side (17), thought to be caused by a combination of the primary cerebral insult and a secondary deterioration of skeletal muscle mass and quality (18). Past studies have shown that muscle mass and the ability to produce isometric force with muscles on the less-affected side is comparatively well preserved and more similar to TD individuals (17). Yet, whether the brain damage hampers power production of larger muscles on the less-affected side during dynamic and explosive actions (e.g. isotonic and iso-inertial RE) needs to be explored to fine-tune RE protocols in individuals with CP.
Therefore, we performed a comparative study of acute RE bouts of isotonic WS-based loading, and iso-inertial FW-based loading in CP and TD adolescents to address the following research questions:
General design
Eight teenagers and young adults diagnosed with CP, and 8 age-matched TD subjects completed 4 testing sessions within a period of 3 weeks. The first session consisted of an ultrasound examination of the vastus lateralis and intermedius muscles of the quadriceps group and the medial gastrocnemius muscle, assessment of anthropometry and passive range of motion (pROM) in lower limb, and familiarization on the WS and FW leg press devices, respectively. In the second session a 7-repetition maximum (7RM) test (unilaterally, in both legs) on the WS leg press was performed followed by a second familiarization on the FW device. The third session consisted of one set of 7RM test for each leg, assessing muscle activity (electromyography; EMG), active range of motion (aROM) and power during the test in the WS device. The session ended with a third familiarization on the FW leg press. During the fourth session EMG, aROM, power, and force were recorded during one set (for each leg) of 7 maximal repetitions using the FW leg press. A minimum of 48 h rest was scheduled between sessions for all subjects, and tests were conducted at the same time of the day (± 2 h) for each subject.
Subjects
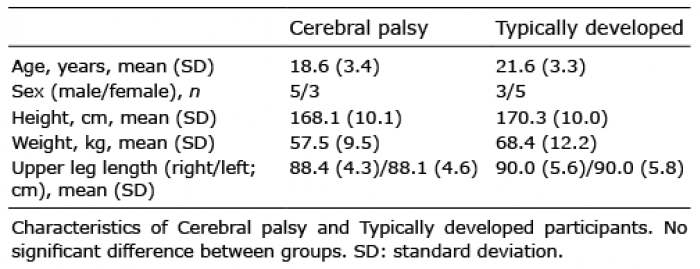
Subjects with CP (n = 8) were recruited from the Department of Pediatric Orthopedic Surgery, Astrid Lindgren’s Hospital, Karolinska University Hospital and the Habilitation services (Stockholm County Council). Inclusion criteria were children and young adults between the ages of 15 and 25 years with unilateral or bilateral spastic cerebral palsy and classified as GMFCS I–III according to Gross Motor Function Classification System, i.e. they could all walk with or without aids (19). Detailed information about type of CP, contractures, spasticity and selective motor control of the foot of all CP subjects can be found in Table SI1. Exclusion criteria included surgical treatment of the knee extensor apparatus within the last 12 months, botulinum toxin treatment within the last 3 months and/or ongoing intrathecal baclofen treatment. A group of 8 TD subjects was recruited in the Stockholm area. Inclusion criteria were an age in the range 15–25 years with no history of neuromuscular diseases. Descriptive characteristics of both groups are shown in Table I. All subjects, and caregivers (when applicable), were informed of the purposes and potential risks associated with the interventions before giving their written informed consent to participate. The study protocol was approved by the Regional Ethical Review Board in Stockholm.
Table I. Characteristics of cerebral palsy and typically developed participants
Seven repetition maximum (7RM)
This test was performed in the WS leg press (NORSK Original Sequence Training System, Scandinavian Rehabilitation Equipment e. K, Borschen, Germany) unilaterally for both legs. Subjects performed 7 repetitions, from ~90° knee flexion to almost full extension (~180°), with a load previously estimated in the familiarization sessions. The load had been set at the second testing occasion, increasing by 5–10 kg in subsequent sets of 7 repetitions until the subject failed to complete the set in 2 successive trials. The 7RM was achieved between 3 and 6 attempts (sets), and trials were interspersed by a 3-min recovery period. Recovery between 7RM in the more-affected/non-dominant leg and the 7RM in the less-affected/dominant leg was 5 min. A standardized warm-up (7 repetitions at 60% of estimated 1RM) was conducted before the 7RM test.
Experimental exercise test on the weight-stack leg press
After the standardized warm-up, one set of 7 repetitions with the load corresponding to the 7RM for each leg was performed (starting with the more-affected/non-dominant leg; 5 min recovery between legs). Active knee ROM during the test was measured through a 3D kinematic system with 8 cameras (Vicon MX40, Oxford, UK) with 18 reflective markers attached to anatomical landmarks on the hips, knees and feet. Peak and mean power, and work were recorded in all repetitions with an encoder (100Hz; SmartCoach™, Stockholm, Sweden), but only the the first 3 repetitions were considered for downstream analysis in order to avoid the influence of potential fatigue. The encoder measures the velocity of every muscle action, and by manually setting the load in the associated software (SmartCoach™), peak and mean power, and work are calculated for each CON and ECC action. Angular velocity was calculated using the range of motion of the first 3 repetitions (°; Vicon) and the time (SmartCoach™) to complete the CON and ECC phases in each repetition. Muscle activity was measured with electromyography (EMG; see below).
Experimental exercise test on the flywheel leg press
Flywheel RE technology utilizes the inertia of a spinning flywheel to generate resistance. One inertia of 0.025 kg·m2 ((YoYo®, Technology AB, Stockholm, Sweden) was used. A standardized warm-up (one set of 7 reps, starting at 50% and progressively increasing the load to ~80% in the last 2 reps) was conducted before the experimental exercise test on the FW leg press. After one initial submaximal repetition to initiate the FW movement, instructions were given to “push” with maximal effort during the entire CON action, as to complete the action as fast as possible. Upon reaching ~170° of knee extension, the FW strap rewound due to inertial forces and the ECC action was initiated. According to our previous studies using this technology, the subjects were instructed during the familiarization sessions to achieve ECC-overload, i.e. they were requested to resist gently during the first third of the ECC action and then to apply maximal “braking” force to stop the movement at approximately 90° knee flexion (20). Then, the next CON action was immediately initiated. CP and TD subjects completed one set of 7 repetitions at maximal intensity for each leg (starting with more-affected/non-dominant leg; recovery time between legs was 5 min). Peak and mean power, work, aROM, and angular velocity were assessed for the first 3 repetitions, as described above for the WS exercise. Muscle activity was recorded using EMG (see below). To investigate whether the CP and TD subjects could produce ECC-overload, the ECC/CON ratio was determined in terms of peak power, i.e. ECC/CON peak power; values >1 indicate the presence of ECC-overload in FW RE execution. These data were compared with the same ratio obtained from the WS exercise bout.
Electromyography
During the experimental tests on both WS and FW devices, electrical activity of the vastus lateralis (VL) and biceps femoris (BF) muscles was assessed by EMG (21, 22). Electrodes were placed according to the Seniam guidelines (23), and raw data (1,000 Hz) was acquired using Vicon system (MX40, Oxford, UK). Data were then transformed to a frequency matching the ROM measurements (i.e. 100 Hz), and peak muscle activation averaged in the 3 first CON and ECC repetitions was calculated. ECC/CON ratio was determined in terms of muscle activity for each muscle group.
Ultrasound
Muscle thickness of the thigh (vastus lateralis and intermedius of the quadriceps muscle together) and calf (medial gastrocnemius muscle) was measured in both legs using ultrasound. The examinations were performed by a paediatric radiologist with musculoskeletal ultrasound experience. For the thigh, the length of the upper leg was measured and divided at half length, which was where the probe was placed. For the lower leg, the probe was placed on the most prominent bulge of the medial gastrocnemius muscle. Ultrasound images were captured using a linear transducer with standard musculoskeletal settings on a Siemens Acuson s2000 (Siemens, Erlangen, Germany). The ultrasound settings were standardized and not altered between subjects. To avoid any pressure by the probe on the muscle that could bias the measurement, ample amounts of water-soluble transmission gel was applied. Pictures were considered valid when the normal curved shape of the superficial part of the muscle was clearly visible. Several images (5–8) were taken of each muscle and averaged to ensure consistency of measured values. Muscle thickness of vastus lateralis and intermedius muscles together was defined as the distance between the fascia overlaying the lateral vastus lateralis and the femur. Gastrocnemius muscle thickness was measured as the distance between the superficial and deep fascia of the medial gastrocnemius. The relationship between muscle thickness and power produced was investigated by dividing the power produced (in Watts) by the muscle thickness (in mm), for each leg, action, and device.
Statistical analysis
All data are presented as mean (standard deviation; SD). Normal distribution of data were verified using the Shapiro–Wilk test. Descriptive data were compared between CP and TD using independent Student’s t-test. Muscle activity and peak power ECC/CON ratio was investigated using a 3-way ANOVA with repeated measures for group (CP vs TD), device (FW vs WS) and leg (more-affected/non-dominant vs less-affected/dominant). A 2-way analysis of variance (ANOVA) with repeated measures for leg (more-affected/non-dominant vs less-affected/dominant) and group (CP vs TD) was used to analyse 7RM data and ultrasound (separately for thigh and calf muscles) results. Peak power, mean power, work, angular velocity, and power (Watts) produced per mm of muscle in the thigh were analysed using a 4-way ANOVA with repeated measures for group (CP vs TD), action (CON vs ECC), device (FW vs WS), and leg (more-affected/non-dominant vs less-affected/dominant). When significant interactions were found, simple effect tests were employed. The level of significance was set at 0.05. Cohen’s d was used to assess the effect size based on differences between means for a given variable (EF; 0.2; small, 0.5; medium, 0.8; large, 1.2; very large). All statistics were computed in SPSS version 25, 2017 (IBM Corp., Armonk, N.Y., USA).
Difference in eccentric/concentric peak power ratio between the flywheel and traditional weight-stack resistance exercise
There was a significant interaction leg × group (p = 0.018; F = 7.1), as well as significant main effects of device (p < 0.0005; F = 32.0) and leg (p = 0.035; F = 5.4) (Fig. 1). Thus, the ratio was significantly greater in FW RE than in the WS RE for CP (most-affected leg; p = 0.003, EF = 1.1, less-affected leg; p = 0.207, EF=0.5) and TD (non-dominant leg; p < 0.0005; EF > 1.2, and dominant leg; p = 0.001; EF > 1.2). The TD group achieved mean values for the ECC/CON ratio above 1, demonstrating peak power ECC-overload during FW RE. This was not observed for the CP group. The ECC/CON ratio of averaged peak quadriceps muscle activation (i.e. EMG) was overall higher in TD subjects compared with CP, independent of device and leg (main effect of group; p = 0.038; F = 5.2) (Fig. 2A). No effects or interactions were observed in the ECC/CON ratio for biceps femoris (Fig. 2B).
Fig. 1. Eccentric (ECC)/concentric (CON) peak power ratio (mean ± standard deviation (SD)) during leg press exercise using a flywheel or a weight-stack resistance exercise device in cerebral palsy (CP) or typically developed (TD) individuals. Note that values > 1 indicate eccentric overload. Significant main effects (p < 0.05); ainteraction leg × group; bmain effect of device; cmain effect of leg. Significant simple effects (p < 0.05); *greater than weight-stack within leg and group. Dom: dominant leg; Ndom: non-dominant leg; LaL: less-affected leg; MaL: more-affected leg.
Fig. 2. Eccentric (ECC)/concentric (CON) ratio in muscle activity (mean±SD) for: (A) vastus lateralis and (B) biceps femoris of the more-affected/non-dominant leg and less-affected/dominant leg during the flywheel and weight-stack exercise in cerebral palsy (CP) and typically developed (TD) individuals. amain effect of group; p = 0.038. Dom: dominant leg; Ndom: non-dominant leg; LaL: less-affected leg; MaL: more-affected leg.
Subjects with CP showed significantly lower peak power independent of device, leg and muscle action (interaction device × action × group; p = 0.001; F = 15.6; EFs>1.2 Table II). Both the TD and CP subjects produced higher power during the CON action compared with the ECC action in the WS device. There was no significant differences between CON and ECC peak power during the acute bout on the FW device for either group. In both FW and WS devices subjects with CP produced less peak power with the more-affected leg compared with the less-affected leg (p < 0.04; EFs 0.6-0.9). Finally, only TD subjects showed higher peak power in the ECC action on the FW compared with the WS device (p < 0.001; EF > 0.9 for both legs).
Similar significant results for mean power were found (Table II); (i.e. higher mean power in TD vs CP, higher mean power in less-affected vs more-affected leg within the CP group, and higher mean power in FW vs WS within the TD group only). Work production in the CP group was lower compared with TD, independent of leg, device and muscle action (p < 0.01, Table II), and the more-affected leg of subjects with CP produced less work in both RE devices than the less-affected leg (p < 0.01). Performing RE in the FW device involved a larger range of motion compared with WS RE (main effect p < 0.0005; F = 30.6; EF = 0.6 Table II). Angular velocity was higher in FW compared with WS (main effect device; p < 0.0005; F = 59.5), although such difference was much greater in TD (EF > 1.2) than CP subjects (EF = 0.6) (interaction device × group; p = 0.002; F = 13.0; Table II). Finally, TD showed greater (EF > 1.2) 7RM values in both legs than CP patients (more-affected/non-dominant; p < 0.0005, less-affected/dominant; p = 0.007; Table II). The values for 7RM in CP subjects were larger in the less-affected leg compared with the more-affected leg (p < 0.0005; EF = 0.9; Table II).
Table II. Power and work production during flywheel or weight-stack resistance exercise, angular velocity and 7 repetition maximum (7RM) in the weight-stack device, in cerebral palsy and typically developed participants.
Performance in muscles of less- and more-affected sides during dynamic resistance exercise
An interaction leg × group (p = 0.002; F = 13.6) was found for the thigh muscles thickness (Fig. 3A). TD presented greater values than the CP group in the more-affected/non-dominant leg (p = 0.02; EF > 1.2). Also, CP subjects showed greater thigh muscle thickness in the less-affected leg than in the more-affected one (p < 0.0005; EF = 1.0). Calf muscle thickness was lower in CP patients independent of the leg (main effect of group; p = 0.001; F = 15.6; EF > 1.2; Fig. 3B). TD subjects produced more power (Watts) per mm of muscle in the thigh than the CP group, independent of leg, device and action (main effect of group; p < 0.0005; F = 26.2; EF > 1.2, Figs 3C and 3D).
Fig. 3. (A) Thickness (mm) of the quadriceps muscle in typically developed (TD) and cerebral palsy (CP) subjects (mean±standard deviation (SD)). (B) Thickness (mm) of the gastrocnemius muscle in TD and CP subjects. (C) Peak power (watts) per mm quadriceps muscle in TD and CP on the weight-stack (WS) device. (D) Peak power (watts) per mm quadriceps muscle in TD and CP on the flywheel (FW) device. *Significantly different from TD (p < 0.05). †Significantly different from less-affected leg within CP group (p < 0.05). ‡Significantly different from TD independent of leg, device and action (p < 0.001). Dom: dominant leg; Ndom: non-dominant leg; LaL: less-affected leg; MaL: more-affected leg.
This study examined whether the difference in ECC/CON peak power ratio between FW and traditional WS RE in CP adolescents is comparable to that observed in TD adolescents. Subjects with CP were able to produce a greater ECC/CON peak power ratio while exercising on the FW device, but absolute values were lower compared with the traditional WS device. Individuals with CP can thus use the correct fast deceleration technique during the eccentric phase of FW, and produce a relatively greater peak power than during WS. But, as impaired motor control in CP reduces the rate of force development (24), a lower absolute peak power output is produced during FW compared with WS.
A further potential reason for the difficulties observed with respect to subjects with CP mastering the iso-inertial FW RE device relates to other aspects of poor neuromuscular control. It has been shown that individuals with CP use fewer synergies (weighted groups of muscles) compared with TD individuals during gait (25, 26). As impaired selective neuromuscular control leads to recruitment of fewer synergies (27), less efficient movement patterns could contribute to less power being produced during RE in individuals with CP compared with TD controls. A recent study by Goudriaan and co-workers targets the importance of neural and non-neural contributors to impaired gait in children with Duchenne’s muscle dystrophy (DMD) (non-neural) and CP (neural + non-neural) (28). This study suggests that the non-neural weakness in DMD has only limited influence on the complexity of neuromuscular control during gait and that the decreased synergistic variance in children with CP is mainly related to neural impairments caused by the brain lesion. In the context of the current study, these data infer that the loading complexity (force, speed and acceleration) of the iso-inertial device hampers performance with respect to peak power in adolescents with CP. Muscle composition in CP is altered with reduced muscle mass and increased amount of intramuscular fat and connective tissue (29–32), which probably also contribute to less force and power being produced.
Skeletal muscle strengthening protocols for individuals with CP have been shown to promote gains in isometric force and task-specific performance (33–35). However, weak transfer effects of RE to functional mobility, such as standing up and walking, walking speed, walking in stairs, and movement measured with accelerometers, have highlighted the need for alternative RE protocols, e.g. with respect to intensity, power and loading strategy. In recent years, some studies have described significant improvements in functional outcomes following a period of training to reach specific goals. Van Vulpen and colleagues (36) have performed a study resembling HIIT (high-intensity interval training) with walking/running/climbing exercises 3 times/week for 14 weeks with progressive resistance. They showed significant improvements in muscle strength, walking capacity and achievement of individually tailored walking/running/climbing goals measured with the goal attainment scale (GAS). Likewise, Gillett and co-workers (35) performed a high-intensity 12-week RE training study targeting the lower limbs, with the addition of anaerobic training activities, and observed improvements in functional outcomes (6-min walking test and a combined score for functional strength including 30-s repetition maximum for lateral step-up, sit-to-stand and stand from half-kneel). Moreover, gains in muscle volume were correlated with increased plantar flexor isometric strength. Therefore, it appears that a common denominator for studies demonstrating transfer effects of RE into functional gains in individuals with CP is a high training intensity and volume, as well as aspects of specificity of training, i.e. training actual functional activities.
We thereafter asked whether there is deficit in performance, probably originating from a neural component (voluntary activation) limiting muscles of both the less- and more-affected sides during dynamic RE in CP. Previous studies have investigated how the brain damage affects force production in individuals with CP. Hussain and colleagues (17) investigated a group of 11 men with unilateral spastic CP and 11 TD controls. Skeletal muscle anatomical cross-sectional area (ACSA), as measured with magnetic resonance imaging (MRI), was significantly reduced in the paretic limb (control: 25.9 cm2, paretic: 20.7 cm2, non-paretic 24.3 cm2). In addition, the more-affected limb was clearly the weaker side, as the plantar flexors of the paretic limb produced 52% less isometric torque compared with the control group, and 42% less compared with the non-paretic side. Similar results were observed, with the more-affected side producing significantly less power. The thickness of the vastus intermedius and lateralis muscles were significantly lower on the more-affected side in the CP group, whereas the same muscle in the less-affected leg did not differ from control. Interestingly, when normalizing peak power either during CON or ECC actions with thigh muscle thickness, it becomes evident that performance in both the more- and less-affected sides is markedly impaired. This suggests that the neural component reduces power production on both sides in an equal manner. Thus, even though muscle thickness is approximately 30% greater in the less-affected leg, power per mm muscle is not greater than the more-affected leg. Poor power production will probably hamper exercise intensity and thereby negatively influence training adaptations. A speculative extrapolation of this finding could be that this suggests that the thigh muscles on both the more- and the less-affected sides in the CP group will not receive an optimal training stimulus with respect to mechanical load during either WS or FW exercise when performing a set with a low number of repetitions. To compensate for the lower RE load during low-repetitions, high-intensity routines (due to the neurological deficit), a possible suggestion is that individuals with CP should instead increase training volume and always aim for repetitions until failure (volitional fatigue). Resistance exercise until failure using >7–10 RM loading, rather than fewer repetitions with high intensity, still calls for both type I and type II muscle fiber activation and produces a similar muscle fiber activation pattern compared with a short duration high-intensity protocol (37). Furthermore, data show that chronic RE training with low loads until failure results in hypertrophy of both type I and type II fibres in TD subjects (38–40). Thus, in CP, RE regimes aiming for repetitions until task failure will probably stress the muscle in a more efficient manner, compared with a pre-set number of repetitions at a comparatively higher load.
Study limitations
When interpreting the results of the present study, some limitations should be considered. The number of subjects in each group may be too small to detect all clinically relevant differences in the loading pattern between FW and WS exercises. Also, the variability added by the different degree of disability in the CP group, as well as the differences between groups in terms of age and weight should be considered. Finally, the fact that the order of testing sessions was standardized, and not randomized, should also be taken into account.
Conclusion
In conclusion, FW RE calls for greater muscle activity during the ECC action than WS RE, which is translated into a greater ECC/CON peak power ratio. However, probably due to impaired neuromuscular control, subjects with CP could not elicit the ECC overload or produce higher absolute peak power on the FW device in a comparable manner to TD adolescents. Moreover, peak power production per mm muscle was markedly reduced in both legs in individuals with CP on both the WS and FW device. Thus, our comparative study of WS and FW exercise does not support the implementation of iso-inertial loading regimes for RE training in adolescents with CP, an interpretation specifically supported by the overall lower peak power output observed in CP subjects on the FW device. We therefore suggest that an alternative loading regime, favouring lower load RE performed until failure, could be more suitable in this specific population.
The authors thank students Negar Chamsai, Sara Rindborg, Olav Kvitastein and Johan Persson for their valuable efforts during data collection.
This work was supported by grants from Linnea & Josef Carlsson (FvW) and Stiftelsen Promobilia and RBU research foundation (RFG).


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize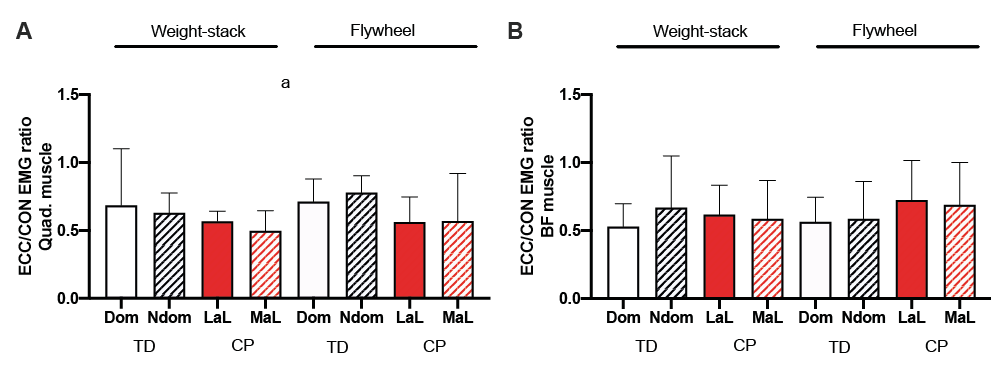 Click to show fullsize
Click to show fullsize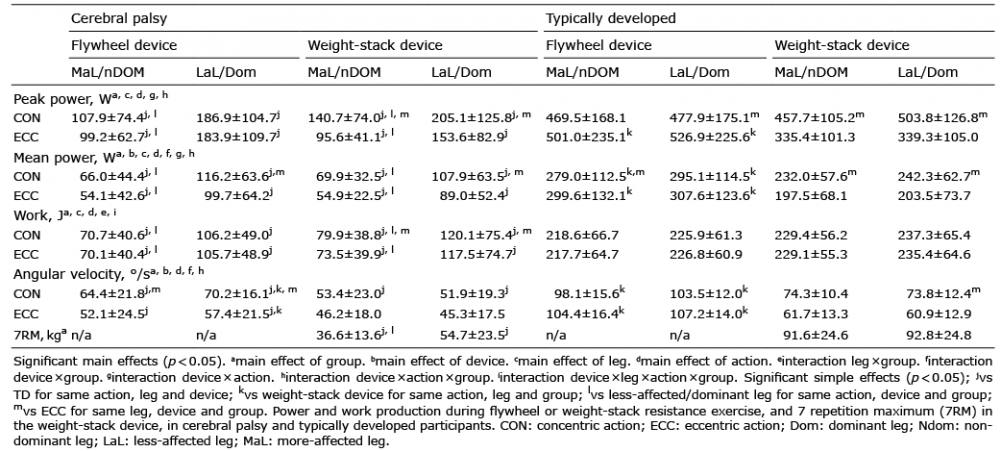 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize