
From the 1Department of Rehabilitation, St Vincent’s Hospital Melbourne, Fitzroy, 2Department of Medicine, Austin Health, The University of Melbourne, Heidelberg, 3Department of Physiotherapy, St Vincent’s Hospital Melbourne, Fitzroy, 4School of Medicine, Monash University, Clayton, 5Department of Occupational Therapy, St Vincent’s Hospital Melbourne, Fitzroy, 6Department of Endocrinology and Diabetes, St Vincent’s Hospital Melbourne, Fitzroy, and 7Department of Endocrinology, Austin Health, Heidelberg, Australia
Objective: To investigate the association of goal attainment scaling outcomes with change in the Func-tional Independence Measure, and the association between the perceived importance, difficulty and degree of achievement of individual goals in general inpatient rehabilitation.
Design: Prospective cohort study.
Participants: A total of 208 participants admitted to inpatient rehabilitation in a metropolitan tertiary referral hospital in Melbourne, Australia.
Methods: Participants determined the nature of the goals and their importance, and therapists determined the difficulty of the goals. The associations were investigated using median regression and random effect ordinal regression.
Results: An increase of each point in the goal attainment scaling score was associated with an adjusted median increase of 0.34 points (95% confidence interval (CI): 0.18–0.5, p < 0.001) in Functional Independence Measure change. More important goals of similar difficulty (very important vs a little important: adjusted common odds ratio (cOR) = 1.97, 95% CI: 1.01–3.83, p = 0.045) and less difficult goals of similar importance (moderately difficult vs a little difficult cOR = 0.59, 95% CI: 0.04–0.87, p = 0.007; very difficult vs a little difficult cOR = 0.59, 95% CI 0.37–0.94, p = 0.027) were better achieved.
Conclusion: Rehabilitation progress measured using the goal attainment scaling method is associated with changes in functional outcomes. For goals with similar difficulty, those with higher importance were better achieved, while for goals with similar importance, less difficult goals were better achieved.
Key words: goal attainment scaling; outcome assessment; inpatient rehabilitation.
Accepted Apr 1, 2020; Epub ahead of print Apr 14, 2020
J Rehabil Med 2020; 52: jrm00054
Correspondence address: Irina Churilov, Department of Rehabilitation, St Vincent’s Hospital Melbourne, 41 Victoria Pde, Fitzroy, Victoria 3065, Australia. E-mail: Irina.churilov@gmail.com
In inpatient rehabilitation the progress made by patients can be measured by setting them individual goals, then measuring how well they achieve the goals using a me-thod called “goal attainment scaling”. An important part of this method is articulating the importance of the set goals by the patient. This study investigates how well the set goals are achieved and whether this can help with understanding patient’s progress in rehabilitation. The results show that the goal attainment scaling me-thod accurately describes patients’ progress in rehabilitation. Goals of similar difficulty that patients considered more important were better achieved. Further research is needed to find out whether routine discussion with the patient of the importance of setting goals is associated with better patient progress in rehabilitation.
Patient involvement in their healthcare-related decision-making has become a focus of research efforts in recent years (1–3), and may lead to improved quality of life and health outcomes (4, 5). Rehabilitation is a medical speciality that focuses on functional performance. Patients’ progress is usually measured by achievement of specific rehabilitation goals (6). Goal attainment scaling (GAS), which measures the degree of this achievement (7) is performed in consultation with patients or their carers (7). GAS has been demonstrated to be beneficial to patients’ motivation and engagement due to its patient-centric nature (8).
The GAS goal-setting process starts at initial assessment and involves setting the expected level of achievement as well as 4 additional levels of potential patient function; 2 above and 2 below the expected level. This method has been found to be feasible in a number of rehabilitation settings, including for patients recovering from acquired brain injury (8–10), arthroplasty (11), veterans (12), patients with upper limb spasticity (13), geriatric patients (14) and amputees (15), although studies in non-neurological diagnostic streams included small sample sizes. The association of the GAS goal-setting method with the more objective and commonly used, standardized and validated Functional Independence Measure (FIM) (16) has been investigated only in patients recovering from acquired brain injury (9, 17), with inconsistent findings in this population. However, the GAS goal-setting method has not been investigated in the full range of inpatient rehabilitation diagnostic streams, including deconditioning, non-arthroplasty musculoskeletal diagnoses and spinal cord injury diagnoses. Furthermore, while GAS goal-setting has been demonstrated to be beneficial to patients’ motivation and engagement, which is hypothesized to be due to patient involvement in the process (8, 18), there is a gap in knowledge about the association between the degree of achievement of individual GAS goals, and their difficulty and perceived importance to the rehabilitation patient. Addressing this gap would benefit achieving better function in rehabilitation patients by supporting the therapists in setting goals that would be both important to patients and be of sufficient difficulty.
The objective of this study was to investigate the use of GAS in general inpatient rehabilitation by: (i) estimating the association of GAS outcomes with standardized functional improvement measures; and (ii) estimating the association between the individual GAS goals’ degree of achievement, difficulty, and perceived importance to the rehabilitation patient.
Settings and participants
This prospective cohort study was conducted in a general rehabilitation unit at St Vincent’s Hospital Melbourne, a tertiary referral metropolitan hospital in Victoria, Australia. Patients consecutively admitted from November 2016 to December 2018 were assessed for eligibility to participate. Patients who were older than 18 years, able to provide informed consent, and had an expected length of stay of over 5 days were eligible for inclusion. Written informed consent was obtained from all participants. The study was approved by the St Vincent’s Hospital Melbourne Human Ethics Committee (approval number LRR/16/SVHM/160). The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines for observational studies were followed.
Measures
Information was collected by multidisciplinary rehabilitation team members trained in administering FIM and GAS tools. Information collected about the participants on admission to the Rehabilitation Unit included demographic, admission diagnoses and Charlson Comorbidity Index (CCI). Participants’ FIM scores were collected on admission and discharge.
Functional Independence Measure
The FIM tool (19) is a 126-point score that assesses the patient’s independence in the domains of self-care, continence, transfers, mobility, communication and cognition. It has been validated as having high internal consistency and adequate discriminative capabilities in inpatient rehabilitation patients (16), and is one of the most common functional measures used in rehabilitation (20). In addition to the total FIM score, we also investigated the physical component of FIM score, defined as the sum of self-care and mobility scores.
Charlson Comorbidity Index
The CCI is an instrument that measures the patients’ burden of disease by describing comorbidities (such as diabetes, malignancy and liver disease) and age. This index was originally developed to predict one-year mortality (21), but is more commonly used to describe the extent of an individual’s illness and disability.
Goal attainment scaling goal-setting and scoring process
Therapists trained in the GAS goal-setting process supported patients in identifying their level of mobility-related performance (physical goals) and self-care-related performance (functional goals) that they hoped to achieve by the time of discharge from inpatient rehabilitation unit. The therapists used these aspirations to formulate a number of goals that were specific and measurable.
Five goal achievement levels were formulated by the
therapists, specifically the expected level of achievement and 2 levels above and below the expected level. On discharge from rehabilitation, the degree of achievement of the GAS goals was assessed by the treating therapists. The therapists were not instructed to place the participant’s admission level of function at -2, as is commonly done in patient populations where some improvement is universally expected, and were instead encouraged to tailor all 5 levels of function to the individual participants. This was due to the wide range of participant diagnoses and their anticipated progress, including some participants where the goal was to optimise safety in view of ongoing functional deterioration.
As part of the GAS goal-setting process, patients were asked to state the degree of importance of individual goals to them, using the following 4 options: Not at all important; A little important; Moderately important; and Very important. The therapists ranked the difficulty of the goals using the 4 options of: Not at all difficult, A little difficult, Moderately difficult, and Very difficult. The therapists’ ranking of a goal’s difficulty was not communicated to the patient.
The GAS score was calculated using the following equation:
where i is the number of the individual goal, wi=weight assigned with the i-th goal (importance multiplied by difficulty) and xi =the score of the i-th goal (22).
This scale is designed so that for patients who achieve the expected level of function, the GAS score is 50. Therefore, it is expected that in a setting where the goals are set in an unbiased fashion, leading to patients over- and underachieving the expected level of function in roughly equal proportions, the median GAS score is expected to be 50 (9).
Semi-structured interviews were conducted with the goal-setting therapists in order to investigate the qualitative aspects of feasibility of the use of GAS method in routine clinical practice.
Statistical analysis
Power analysis showed that, assuming a 2-tailed alpha of 0.05, recruitment of 200 participants would yield 0.8 power to observe a small-to-medium effect size in correlation between GAS score and FIM change (rho = 0.2).
GAS scores were summarized as medians and interquartile ranges (IQRs) and compared across diagnostic streams using Kruskal–Wallis test.
The association between GAS score and FIM change (both for total FIM and physical component) at the patient level was investigated using quantile regression due to the violation of the assumption required for standard linear regression and lack of suitable transformations to satisfy these assumptions. Quantile regression estimates differences in the quantiles of the FIM change variable per 1-point increase in GAS score. For example, a median (50th percentile) regression of FIM change on GAS score estimates the difference in the median FIM change per 1 unit increase in GAS score adjusted for patient’s age and admission FIM. The current study included 3 quantile regression models: the 25th percentile, the 50th percentile (median), and the 75th percentile. Standard assessment of collinearity was conducted using variance inflation factors (VIF) and condition number.
Associations between the importance of individual goals and their degree of achievement, and between the difficulty of individual goals and their degree of achievement, were investigated using random effect ordinal logistic regression modelling, with degree of individual goal achievement on an ordinal scale as dependent variable, and patients’ age, Charlson comorbidity score, baseline FIM, goal’s difficulty and importance as independent variables, and individual patients treated as random effects. Respective effect sizes were estimated using a common odds ratio (cOR) of better achieving the goals with corresponding 95% confidence intervals (CIs), with goals that were a little difficult and of low importance used as reference categories. Goals that were either not at all difficult or not at all important were excluded from the analysis due to very low count that would render any comparison meaningless. Proportional odds assumptions were verified using Brant and likelihood-ratio tests.
Statistical analysis was conducted using Stata 15IC statistical software (StataCorp, College Station, TX, USA). p-values below 0.05 were regarded as indicative of statistical significance.
A total of 208 participants were recruited for the study from November 2016 to November 2018. The median age was 65 years (IQR 54.5–73), and 53% were male. The diagnostic streams and their age and sex distributions are shown in Table I.
Table I. Patients’ diagnostic streams, age and sex
The overall median GAS score was 56 (IQR 50–63), ranging from median 62 (IQR 50–68) in Spinal diagnostic stream patients to median 55 (IQR 47–54) in the Other/Deconditioning diagnostic group (Kruskal–Wallis p = 0.68 ) (Fig. 1). The median admission FIM was 87 (IQR 76–99), and the median FIM change was 22 (IQR 12–31). For physical components of FIM, the median admission value was 54 (IQR 42–64), and the median change was 22 (IQR 12–30).
Fig. 1. Goal attainment scaling (GAS) scores by diagnostic streams. The expected level of 50 is indicated by the red line. Diagnostic streams: Amp: amputee; Mus: musculoskeletal; Neu: neurologica; Dec/Oth: deconditioning/other; Spi: spinal.
Association between goal attainment scaling and Functional Independence Measure: patient-level analysis
Adjusting for age and baseline FIM, a 1-point increase in GAS score was associated with a statistically significant median increase of 0.34 points in FIM change (95% CI: 0.18–0.5, p < 0.001). The corresponding increase for the 25th percentile was 0.53 (95% CI 0.24–0.81, p < 0.001), and for the 75th percentile 0.25 (95% CI 0.12–0.39, p < 0.001) (Fig. 2a). Similar findings were observed for the association between physical components of FIM and GAS (25th percentile: 0.49 (95% CI 0.23–0.74; p < 0.001); median 0.33 (95% CI 0.18–0.49; p < 0.001); 75th percentile: 0.26 (95% CI 0.13–0.39; p < 0.001)).
There was a clear ceiling effect observed in FIM at discharge, while no obvious ceiling effect was present for GAS score (Fig. 2b).
Fig. 2. (a) Increase in Functional Independence Measure (FIM) change per point increase in goal attainment scaling (GAS) score with 95% confidence interval (95% CI) for different study sample quantiles. (b) Discharge FIM and GAS score for the study sample.
Association between difficulty of goals, their importance, and achievement: goal-level analysis
A total of 751 individual goals were set: 433 (58%) physical, 253 (34%) functional, 38 (5%) combined, and 27 (3%) other. The majority of goals were deemed to be very important by the patients (472 goals (63%)), with 229 goals (30%) moderately important, 43 goals (6%) a little important, 4 goals (0.6%) not at all important, and 3 goals (0.4%) not having been designated a level of importance. The distribution of the goals’ difficulty was 201 goals (27%) were very difficult, 341 goals (46%) moderately difficult, 201 goals (27%) a little difficult, 5 goals (0.7%) not at all difficult, and 3 goals (0.4%) not having been designated a level of importance.
Adjusting for patients’ age, Charlson comorbidity score, baseline FIM, and the goal’s difficulty, more important goals had higher common odds of being better achieved (moderately important vs a little important cOR=1.35, 95% CI: 0.68–2.69, p = 0.395; very important vs a little important cOR = 1.97, 95% CI: 1.01–3.83, p = 0.045) (Fig. 3). Adjusting for patients’ age, Charlson comorbidity score, baseline FIM, and goal’s importance, more difficult goals had lower common odds of being well achieved (moderately difficult vs a little difficult cOR = 0.59, 95% CI: 0.04–0.87, p = 0.007; very difficult vs a little difficult cOR = 0.59, 95% CI 0.37–0.94, p = 0.027). Similar results were observed when they type of goal was included as an additional covariate in both models.
Fig. 3. Individual goals’ importance and degree of achievement.
The treating therapists reported that, while the GAS goal-setting process was initially more time-consuming than the routine goal-setting for rehabilitation patients (which does not require the setting of 4 extra achieve-ment levels, difficulty or importance), its efficiency improved with time. The opportunity to discuss the goals in greater depth was felt to be beneficial for building rapport with the patients.
The main findings of this study are that there is a clear association between more subjective and patient-centric outcomes of GAS goal-setting method and more objective and commonly used, FIM measures in a variety of neurological and non-neurological diagnostic streams, and that more important goals of similar difficulty and less difficult goals of similar importance are better achieved.
Association between goal attainment scaling scores and Functional Independence Measure change
The main limitation of the GAS goal-setting process is that it is inherently subjective (9, 23). In the absence of a standardized scale, experienced clinicians are relied upon to judge difficulty and expected level of achievement, based on their past experience with similar patients, and to guide junior allied health staff. The consistent finding of GAS median above 50 indicates the therapist’s conservative approach in setting the “expected” level of achievement. It was, therefore, reassuring that an association was identified between GAS score and FIM change. This finding provides evidence for concurrent validity of GAS in the general rehabilitation population. Nearly identical results for the analysis of the total FIM score and its physical component were likely to be explainable in this patient sample by the inclusion criterion of being able to provide informed consent. Although remaining positive and statistically significant for the key percentiles of the sample, the magnitude of association varied, with smaller increase in FIM change per 1-point increase in GAS score observed for higher percentiles. We hypothesize this to be the manifestation of a potential ceiling effect of FIM score in this study sample, where is not possible to observe sufficient increase in FIM during the inpatient rehabilitation episode in the patients with sufficiently high baseline FIM values. The absence of a ceiling effect in GAS scores makes this method more sensitive to assessing progress in patients who achieve a higher functional level.
Goals more important to patients are better achieved
It is well recognized that rehabilitation goals should be specific, measurable, achievable, realistic and time-specific (SMART) (7) and set in consultation with the patient, and this forms the basis of GAS goal-setting. GAS goal-setting has been previously demonstrated to be beneficial to patients’ motivation and engagement, which is hypothesized to be due to patient involvement in the process (8, 18). However, in the context of time pressures that are inevitable in clinical setting, it is not uncommon for the goals to be set without a specific discussion with the patient, especially when the goals relate to such universally important activities as independent mobility and self-care. Based on the findings of the current study, we hypothesize that engaging the patient in explicitly articulating the importance of the rehabilitation goals set as a part of GAS goal-setting method may contribute to subsequently better achieving the more important goals. Ensuring that the majority of the set goals are important to the patient may facilitate better goal achievement. Patient involvement in the goal-setting process may therefore contribute to achieving improved specific and measurable rehabilitation outcomes, which we demonstrated to be associated with improvement in objective and validated FIM measures. This hypothesis may be tested in a prospective randomized study explicitly comparing patient outcomes using different goal-setting methods as an intervention.
Study limitations
The main limitation of this study is that it was conducted in a single centre. Coupled with the inherently subjective nature of the GAS goal-setting method, the generalizability of our findings will need to be further established. At the same time, the findings that the patients who achieve better GAS score also achieve better functional performance on a well-established objective measure, as well as the consistency of our findings regarding the relationship between importance and degree of achievement of individual goals with psychology literature, provide reassurance of the validity of our results.
Conclusion
This study found that a subjective measure of patient progress in inpatient rehabilitation, encapsulated by the patients’ GAS score, was consistent with a more objective measure of change in functional independence. Among individual patient goals with similar difficulty, those with higher importance were better achieved, while among individual goals with similar importance, less difficult goals were better achieved.
As patients’ involvement in goal-setting aims to ensure articulation of the importance of the goals to the patient, further investigation is needed to evaluate whether routine discussion of the importance of set goals to the patient is associated with a higher degree of goal achievement.
The authors gratefully acknowledge the contribution of the St Vincent’s Hospital Melbourne Rehabilitation Unit allied health staff in incorporating the GAS goal-setting method into their work with the study participants.
Irina Churilov acknowledges the support of the Australian Commonwealth Government through the Australian Government Research Training Scholarship.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize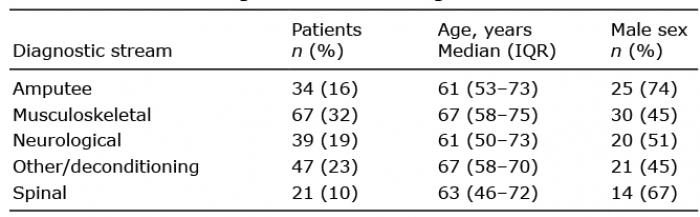 Click to show fullsize
Click to show fullsize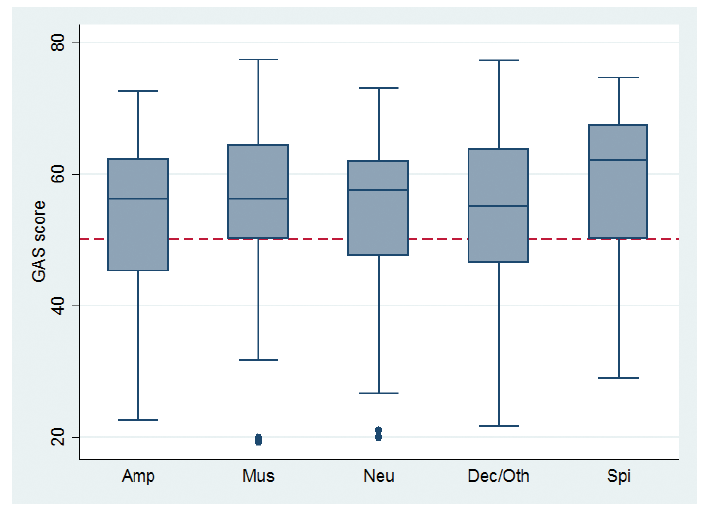 Click to show fullsize
Click to show fullsize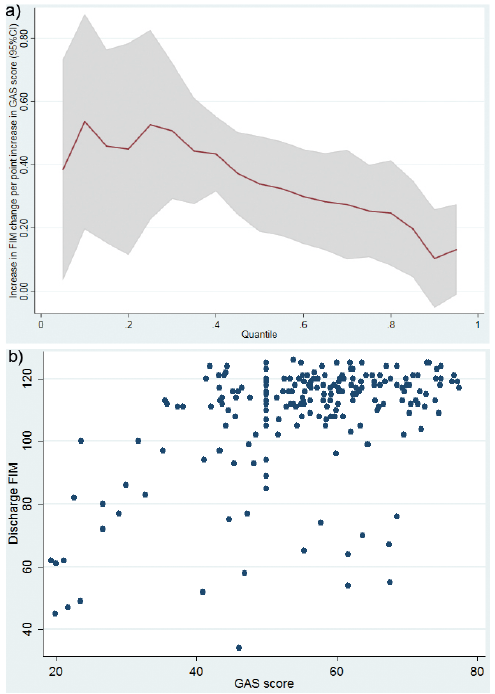 Click to show fullsize
Click to show fullsize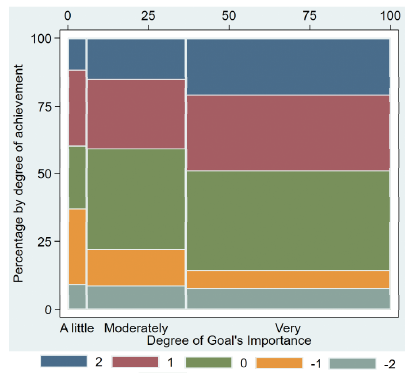 Click to show fullsize
Click to show fullsize