
From the 1Institute of Neuroscience and Physiology, Rehabilitation Medicine, Sahlgrenska Academy, University of Gothenburg, and the Sahlgrenska University Hospital and 2Institute of Neuroscience and Physiology, Department of Health and Rehabilitation, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
*Joint first authors.
Objective: A prospective, observational study to describe levels of physical activity in patients with stroke on day 2 and day 5 or 6 after admission to a comprehensive stroke unit in Sweden.
Methods: The study was performed at the stroke unit at Sahlgrenska University Hospital during a period of 4 months between 2017 and 2018. Consecutive patients with stroke were observed for 1 min every 10 min while the multidisciplinary team was at work. The level of physical activity, location and the people present were noted at each time-point.
Results: A total of 46 patients were observed on day 2, of whom 29 were observed a second time on day 5 or 6. Patients were in bed half of the time and engaged in upright activity for less than 10% of day 2. Patients spent 73% of day 2 in the bedroom and 56% of this day alone. Over time, there was a significant shift of 10% from “in bed” activity to “sitting” (p <0.001).
Conclusion: Patients are physically inactive, alone and in their rooms for a majority of the time during the first days at a comprehensive stroke unit. There is some increase in physical activity during the first week after admission.
Key words: stroke rehabilitation; exercise; observation; physical therapy modalities.
Accepted Mar 23, 2020; Epub ahead of print Apr 7, 2020
J Rehabil Med 2020; 52: jrm00041
Correspondence address: Adam Viktorisson, Sahlgrenska Academy, Institute of Neuroscience and Physiology, Per Dubbsgatan 14, 3rd floor, PO Box 430, SE 405 30, Gothenburg, Sweden. E-mail: adam.viktorisson@gu.se
This study aimed to map physical activity in patients treated at a stroke unit in Sweden between day 2 and day 5 or 6 after admission to hospital. The patients were observed for 1 min every 10 min between 08:00 h and 17.00 h on these days. A total of 46 patients were observed on day 2, of whom 29 were observed again on day 5 or 6. These results show that patients are inactive, alone and in their rooms for a majority of the time at the stroke unit. This study also shows that there is some increase in physical activity over time during the first days of the hospital stay.
Stroke is an acute cerebrovascular disorder and the largest single cause of long-term disability in European adults today (1). Since a majority of patients survive the acute phase of stroke, many go on to a life with new bodily circumstances that are unexpected and potentially lifelong. The most common sequelae post-stroke include cognitive impairment, disability and reduced participation (2). Early rehabilitation and organized inpatient care following stroke are important contributors to a better neurological outcome (3, 4). Treatment at a stroke unit is associated with improved survival and better functional recovery (5, 6); hence, in Sweden, all patients with stroke are recommended this treatment (7). Stroke rehabilitation in Sweden begins directly upon hospital arrival, unless palliative care is initiated, and is provided by a multidisciplinary team (3).
Physical activity is defined as “any bodily movement produced by the contraction of skeletal muscles that results in energy expenditure” (8). Early implementation of physical activity is an extensively studied component of stroke unit care and has been named one of the most important contributors to a better outcome post-stroke (9, 10). An increased level of physical activity has also been associated with improved motor recovery, quality of life and activities of daily living (ADL) (11, 12). In contrast, a recent multicentre study on very early stroke mobilization found evidence that too much out-of-bed activity within the first day after onset may, in fact, impair the recovery process, as measured by a modified Rankin Scale score, 3 months after stroke (13). Therefore, it is becoming more evident that the total amount and frequency of early out-of-bed activity during the hospital stay may be of greater importance than the time of first mobilization (14).
The activity levels of acute stroke patients can be attributed to a number of factors, such as overall health, body function and participation, as well as environmental factors and activities, defined by the International Classification of Functioning, Disability and Health (ICF) (15). Previous studies have found increased levels of physical activity among stroke patients of younger age, independent gait and those subjected to more intensive rehabilitation programmes and enriched environments (16–18). Research on physical activity levels among patients with stroke during the first few days are sparse, but could provide valuable knowledge regarding the optimal timing and dosage of physical rehabilitation (19). Previous studies have reported that stroke patients spend more than one-third of their days in bed within 2 weeks after admission and approximately two-thirds of the day alone (18, 20).
The main aim of this study was to describe the levels of physical activity in patients with stroke at a comprehensive stroke unit in Sweden on the second day after admission. In addition, the levels of physical activity were observed again on day 5 or 6 among patients still receiving treatment at the hospital. The predefined period of inclusion was 4 months, which was divided into 2 periods of 2 months during summer and 2 months during winter.
Design and setting
This prospective, observational study was conducted at the comprehensive stroke unit at Sahlgrenska University Hospital, Gothenburg, Sweden. The stroke unit has a catchment area of approximately 700,000 people, and patients who are subject to thrombolysis or thrombectomy in nearby regions are also transported to this hospital. A multidisciplinary team, consisting of nurses, physiotherapists, occupational therapists, speech and language therapists, psychologists, and social workers, work at the unit. All patients are assessed by a physiotherapist, an occupational therapist and a speech and language therapist within 24 h of hospital arrival, in accordance with the National Swedish Stroke Guidelines (7). The physiotherapist evaluates gait, transfer, postural balance and upper and lower limb function. The occupational therapist evaluates fine motor skills, cognitive function and ADL. The speech and language therapist evaluates swallowing, understanding and speech. Individual rehabilitation programmes are set up for each patient. All patients receive a minimum of 30 min training with a physiotherapist and 30 min with an occupational therapist each day. Individual rehabilitation begins on the day of hospital arrival and is provided Monday to Saturday by the physiotherapist and occupational therapist, and Monday to Friday by the speech and language therapist. Nursing assistants working at the stroke unit are trained to provide rehabilitation on Sundays and holidays. The mean length of stay for patients treated at the stroke unit during the study period was 11 days.
The stroke unit at Sahlgrenska University Hospital was built in 2009. It comprises a total of 21 beds; 4 in single rooms and the others in shared bedrooms with 2 or 3 beds in each. All rooms have a window and a television. The rooms are located along the same corridor as a patient lounge with a television, sofas and a kitchen. Patients can move freely within the room, corridors and patient lounge. Therapy areas are on the same floor of the building, but patients can access them only when accompanied by personnel. Nursing staff have 2 workplaces in the corridor, from which they can oversee the ward. The ward also has a balcony, which is open mainly during the summer months. There is a cafeteria downstairs and a garden outside.
Study population and data collection
All patients who were treated at the stroke unit and fulfilled the inclusion criteria were enrolled consecutively during 2 periods of 2 months: 12 June 2017 to 14 August 2017 and 15 January 2018 to 16 March 2018. The inclusion criteria were: age 18 years or older, diagnosed with a first or recurrent acute stroke (as defined by the World Health Organization (21)) and available for observation on day 2 (24–48 h) after hospital admission. Exclusion criteria were: stroke due to subarachnoid haemorrhage, patients who could not receive information about the study due to language barrier/severe aphasia (with whom communication was impossible), or patients undergoing palliative care (for whom rehabilitation was not initiated).
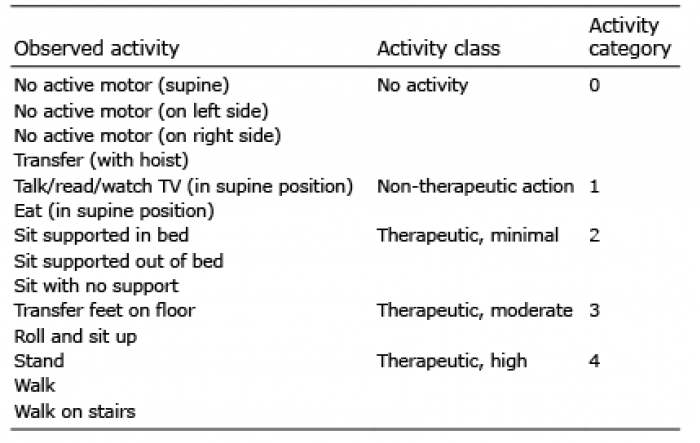
Four observers (medical students) performed all observations. During one day of observation, a total of 50 observations were made per patient. The observations took place during work days (Monday to Friday) from 08:00 h to 17.00 h, when the stroke unit’s multidisciplinary team was at work. Patients were observed for 1 min every 10 min on a single day, with the exception of a 30 min to 1 h lunch break and 2 randomly scheduled shorter breaks. All observations on 1 patient were performed by the same observer. Between each observation, patients were left alone by the observer. At each registration time-point, the observer reported the patient’s location, the people present, and the patient’s physical activity according to the Case Report Form for Observed Motor Activity from the National Stroke Research Institute (NSRI) in terms of activity category (AC), as detailed in Table I (20). If a patient was still receiving care at the stroke unit, a second observation was performed on day 5 or 6 (96–144 h after hospital admission) following the same routine. Demographic variables and data regarding stroke-related and diagnostic tools, including the National Institutes of Health Stroke Scale (NIHSS) and Saltin-Grimby Physical Activity Level Scale (SGPALS), were collected from the medical records of included patients.
Table I. Physical Activity Categories from the National Stroke Research Institute
Statistics and data analysis
The observation standards of the observers were calibrated through common evaluation of several test subjects prior to the start of the study. The first 5 patients were observed in pairs and inter-rater reliability of observed motor activity was calculated with Cohen’s kappa coefficient to ensure a substantial agreement. Cross-tabulation was made between AC and all locations and all people present. Physical activity levels between day 2 and day 5 or 6 of patients observed at both time-points were compared with Wilcoxon signed-rank test and presented as a bar chart with shift of proportions of the ACs. A correlation analysis was performed, between 4 independent variables (sex, age, NIHSS, and SGPALS) and the median AC on day 2. The analysed variables were included based on clinical reasoning. Statistical analyses were performed with IBM SPSS Statistics 24.0 (Armonk, NY, USA: IBM Corp). All p-values were 2-sided and interpreted at a 0.05 significance level.
Ethics
The study was approved by the Regional Ethics Committee in Gothenburg (EPN384-17). Information about the purpose of the study and its conduct was provided both verbally and in writing. Written consent was obtained from each study participant.
A total of 557 patients were admitted to the stroke unit for a suspected stroke during the enrolment periods, of whom 312 (56%) were discharged with a stroke diagnosis (Fig. 1). Approximately one-third (30%) of the stroke patients were discharged before day 2 (to their home or a regional hospital) and a further one-quarter (27%) could not be observed, as day 2 fell on a weekend. A total of 67 patients were targeted for participation and 46 were enrolled for observation on day 2 after admission. Of these, 29 were still receiving treatment at the hospital and were available for a second observation on day 5 or 6. A total of 3,606 observations were made of the 46 patients. Of these, 2,202 observations were made on day 2. At 243 of the time-points (6.7%) it was not possible to ascertain the type of physical activity, due to the patient being in a private situation (3.9%) or off-ward (2.8%). Demographic variables and data regarding stroke-related and diagnostic tools are shown in Table II.
Fig. 1. Flowchart of study population.
Table II. Baseline patient demographics (n = 46)
Stroke patients were lying in bed (AC0-1) for 49% of the second day of admission to the stroke unit and engaged in standing and/or walking for only 7% of the time that day. At this time-point, they spent 73% of their day in their room, 6% in the hallway and 9% in the patient’s lounge. Only 3% of day 2 was spent in the therapy area. On average, the patients spent more than half of the observed day (4.5 h) alone. When in their rooms, patients were observed to be in bed approximately 65% of the time. In the hallway and therapy area physical activity levels were fairly equal, with 55% of the time in a sit supported position and 40% standing or walking. On average, patients were accompanied by a therapist (physiotherapist, occupational therapist, or speech and language therapist) 12% (60 min) of the observed day. Patients were found to be most active in the presence of a physiotherapist, with almost 40% of the time spent standing or walking (AC4) and only 20% of the time lying down (AC1-2).
A significant correlation was found between pre-stroke physical activity (SGPALS) and a higher median AC at the stroke unit on day 2 (Spearman’s rho value = 0.302, p = 0.044). There was also a significant correlation between stroke severity (NIHSS) and physical activity at the stroke unit, where a more severe stroke correlated with a lower median AC on day 2 (Spearman’s rho value = 0.296, p = 0.046). In contrast, there was no correlation between age or sex and the observed AC at the stroke unit on this day.
A comparison between ACs on day 2 and day 5 or 6 is shown in Fig. 2. Only patients who were observed on both occasions (n = 29) were included in the shift analysis. There was a significant decrease in time spent in AC1 and a significant increase in activity in AC2 over time (p < 0.01). In other words, approximately 10% of the in-bed activity had shifted to sit supported activity at the second observation time-point.
Fig. 2. Shift-analysis of the mean time patients spent in each activity category (AC) on day 2 compared with day 5 or 6. Results from Wilcoxon signed-rank test comparing physical activity between the 2 time-points is shown as a Z-score and p-value (n = 29).
To our knowledge, this is the first study to map physical activity levels in the very early phase of stroke in a comprehensive stroke unit ward. The primary aim of this study was to describe observed levels of physical activity in patients with stroke at a comprehensive stroke unit on day 2 after admission. Included patients were found to spend half of their day in bed when the multidisciplinary team was at work. In contrast, patients engaged in upright activity, such as standing and walking, for less than 10% of the day, and spent more than half the day alone. A secondary aim was to compare differences in the level of physical activity on day 2 and day 5 or 6. There was a statistically significant decrease of 10% in bed-bound activity in favour of sit supported activity at the second observation time-point.
Previously reported data from 24 studies summarized in one review article concluded almost identical levels of physical activity (corresponding to the AC classification in NSRI) as this study (19). However, many of the observational studies of physical activity in the early phase of stroke have defined the acute phase as within the first 2 weeks after symptom onset, and a majority of the studies were not carried out in an acute stroke unit ward, but in rehabilitation units (19). Furthermore, several of these studies did not report time since stroke and or admission to hospital. This is problematic, as almost half of the patients in the current study had been discharged within the first week after hospital admission.
Significant correlations were found between low levels of physical activity at the stroke unit and a more severe stroke and a low pre-stroke physical activity level. These results coincide with previous results from a Swedish study on physical activity and stroke severity, where low pre-stroke physical activity was found to predict a more severe stroke (22). There is a question as to whether the results reflect a need for rest or if there is more potential to mobilize patients with beneficial results. In another study from Sweden, there was no significant difference between an inpatient rehabilitation setting and an acute stroke unit setting regarding physical activity in stroke survivors (23). However, in a rehabilitation setting, patients spent less time lying in bed, less time in their rooms, and more time with therapists. These results suggest that patients will perhaps not be more active unless therapy time is increased. In another recent study, environmental change from a rehabilitation unit to the patients’ homes was associated with reduced time in the sitting position and increased time spent standing and walking, measured using activity monitors (24). The fact that patients in the current study were observed in their room 73% of their day certainly reveals flaws in the environment, especially as they were observed to be in bed for more than 60% of the time spent in their room. A study comparing different stroke units found that patients treated at a unit with shared bedrooms were more active than patients at a unit with exclusively single bedrooms (25). Another study found that stroke units serving food in communal areas had more physically active patients compared with units in which food was served in patients’ rooms (26). Personnel working at the stroke unit investigated in this study observed that patients became less motivated to get out of bed and spent less time in the patients’ lounge when all rooms were equipped with a television. In addition, many of the locations at the stroke unit are not easily accessible to patients; the therapy area is available only while the patient is in therapy, the patients’ lounge is mainly used for meals, and patients rarely stay in the hall for a longer period of time, due to the inconvenience created for staff by patients obstructing the hallway. Access to other, enriched, areas could enable patients to be more physically active throughout the day, beyond the time spent in therapy (17). Future research on how the environment influences physical activity is needed to clarify how patients are encouraged or discouraged to undertake physical activities when treated at an acute stroke unit. The fact that patients remaining at the stroke unit became more active on day 5 or 6 might represent that their health improved, or perhaps that they were more able, or better encouraged, to participate in physical activities.
When attended by a physiotherapist, patients were observed to be most active in comparison with other members of the multidisciplinary team, which confirms the results from a previous study (18). Patients were also active while attended by an occupational therapist, but to a lesser extent compared with the time spent with a physiotherapist, which supports the results of previous studies (27). When patients were accompanied by a speech and language therapist, they were sitting (supported and unsupported) 70% of the time, which affirms the idea that most speech therapy sessions take place in a sitting setting. No patients were likely to be physically active beyond therapeutic levels (13).
Methodical considerations and limitations
As with many observational studies, the effect of the attending observer should be considered. Although patients were instructed to not pay attention to the observer, patients often acknowledged the presence of an observer by making eye-contact. The presence of the observer might also have affected the staff attending the patient. In such cases, the physical activity level was probably overestimated. Today, various devices, such as accelerometers and step counters to monitor activity after stroke increase in use. The greatest advantage of such devices, over an observational method, is that the measurement is more accurate, as it measures continuously over the course of a day. However, the accuracy of the measurements of bed-bound patients must be considered. In addition, the positive effect on physical activity of wearing an activity monitor should not be neglected. In contrast to activity monitors, the observational technique can provide information about where the patient is and with whom they interact. Although, physical activity level was recorded during the 1-min observation, it cannot be assumed that it was maintained for the entire 10-min period between observations.
There are limitations to the generalizability of the results of this study. Firstly, the results reflect only a single stroke unit, and physical activity levels are known to vary between stroke units, both nationally and internationally. Patients were, however, included during 2 months in the summer and 2 months during winter in an attempt to diversify the study population and minimize selection bias. A fixed enrollment period of 4 months was set to avoid reporting bias. As mentioned previously, physical activity levels are probably dependent on the environment at the stroke unit. Secondly, there is probable selection bias, as the majority of the patients included in this study had had a minor stroke. Patients with more severe stroke were less able to give written consent to participate in the study. Thus, these results cannot be conclusive of patients with stroke overall. In addition, more than one-third of all patients in this study were discharged from the stroke unit before day 5 or 6. The group observed at the second time-point must therefore be presumed to be of worse health compared with the group that left the hospital early, which further complicates the interpretation of the results. In a study examining acute stroke patients, a higher NIHSS score was associated with lower levels of physical activity (20). However, NIHSS at admission does not give the full picture, as the impact of stroke and the potential level of physical activity will be dependent on what treatment (i.e. thrombolysis, thrombectomy etc.) patients are given during the hospital stay. Lastly, no sample size calculation was performed, as the periods for enrollment were set beforehand. The p-values should therefore be interpreted with caution.
Conclusion
Patients with stroke were observed to be inactive for the majority of the day during the first few days after admission to a comprehensive stroke unit in Sweden. Patients were also observed to be alone and in their rooms for a large proportion of the day, both associated with low physical activity. These findings may or may not be a reflection of the patients’ need for rest, but what is of more importance is the necessity to further investigate what amount of physical activity should be provided and when it should be implemented.
The authors thank Amina Cehic, Rua Hasan and Nafeesa Ambreen for their help with data collection, Professor Julie Bernhardt for access to the Case Report Form for Observed Motor Activity, and Dr Kate Bramley-Moore for English language proofreading. This study was supported by grants from the Swedish Research council (VR2017-00946), the Swedish Heart and Lung Foundation, the Swedish Brain Foundation and by grants from the Swedish government under the agreement between the Swedish government and the county councils: the ALF agreement (ALFGBG-718711).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize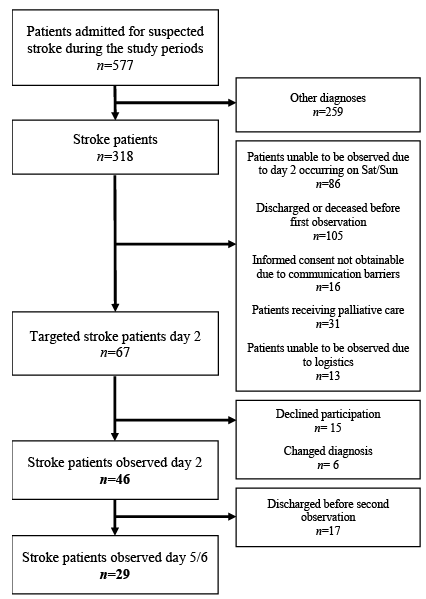 Click to show fullsize
Click to show fullsize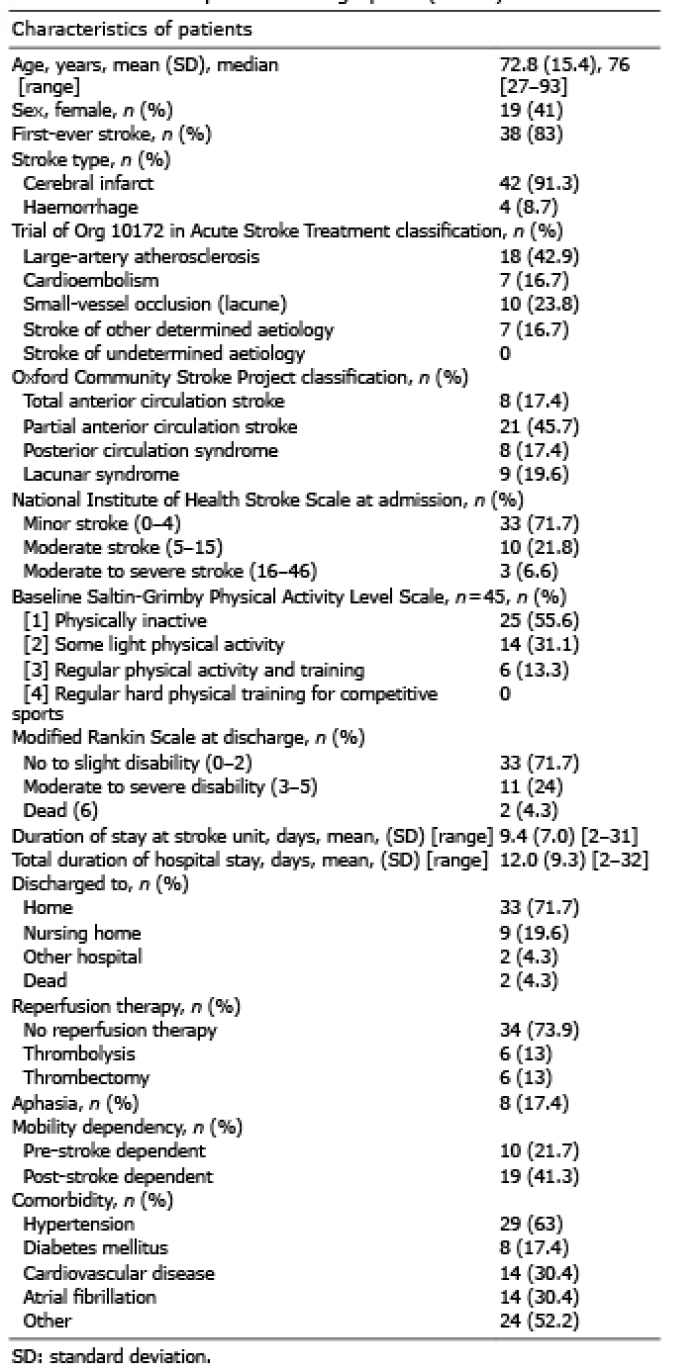 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize