
From the Department of Clinical Neuroscience, The Sahlgrenska Academy, University of Gothenburg and Sahlgrenska University Hospital, Gothenburg, Sweden
The paper presents a summary of the Olle Höök lecture, which was presented at the Baltic and North Sea Conference on Physical and Rehabilitation Medicine in Oslo, Sweden, in October 2019. The paper aims to provide a worldwide picture of stroke, developments in this field, and the evolution of stroke rehabilitation. It sets out the background to, evidence for, and content of the comprehensive stroke unit. The paper also describes some rehabilitation techniques based on neurophysiology, the use of robotics, and the evidence level for interventions. Organization of the stroke care chain and different aspects of rehabilitation during its trajectory are described. However, the need for rehabilitation is often not met, due to restricted and unevenly distributed resources. With increasing knowledge of neurophysiology and evidence from meta-analyses, the content of stroke rehabilitation will continue to evolve.
Accepted 2020, Mar 20; Epub ahead of print April 3, 2020
J Rehabil Med 2020; 52: jrm00053
Correspondence address: Katharina Stibrant Sunnerhagen, Institute of Neuroscience and Physiology, University of Gothenburg, Per Dubbsgatan 14, 3rd floor, 413 45 Göteborg, Sweden. E-mail: ks.sunnerhagen@neuro.gu.se
This paper presents a summary of the Olle Höök lecture, which was presented at the Baltic North-Sea Forum Conference in Oslo, Sweden, in October 2019. The paper
aims to provide a worldwide picture of stroke, developments in this field, and the ongoing development of stroke rehabilitation. It describes the background to, evidence for, and content of the comprehensive stroke unit. The paper also describes some rehabilitation techniques based on neurophysiology. In addition, the use of robotics is described, as well as the evidence level for the interventions. The organization of the stroke care chain and different aspects of the rehabilitation trajectory are described. However, the need for stroke rehabilitation is often not met, due to restricted resources and their uneven distribution. With increasing knowledge from neuro-physiology, and evidence from meta-analyses, stroke
rehabilitation will continue to develop in the future.
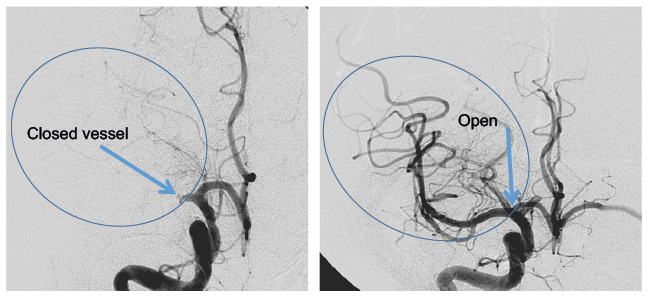
Research into the global burden of disease shows that the number of stroke cases is increasing (1) and that the incidence risk of having a stroke is 1 in 4 (1 in 2 in China, and 1 in 3 in some Eastern European countries). This global increase is due to the increasing number of cases in less developed parts of the world. Socioeconomic status is associated with stroke incidence (2); poverty leads to stroke and stroke leads to poverty (3). In the high-income countries, the incidence of stroke is decreasing (1). However, improved acute care has been shown to result in higher survival rates and increased disability adjusted life years (DALYs) (4). One reason for improved acute care is the provision of stroke units (5) with reperfusion therapy (6, 7) (Fig. 1).
Fig. 1. Angiogram showing a clot blocking blood circulation. Pre- (left-hand image) and post- (right-hand image) reperfusion.
Rehabilitation is traditionally targeted to the patient’s needs. The goals therefore often contain different components or are multifaceted. Thus it is difficult to perform traditional randomized trials, in which both the patient and the health professional are blinded (8). However, it is possible to perform single-blinded trials. The complexity of rehabilitation also means that a stringent theoretical approach is required when the interventions are delivered (9). Is the focus on impairment then assessment should be on impairment. Is the focus on participation in society the intervention and assessment require another set of tools. Interventions may vary with time. In addition, the complex interventions often delivered in stroke rehabilitation may be difficult to assess, and often require more than 1 outcome measure. A wide range of outcome measures are available (10). This has led to discussion regarding the best measures to use in stroke trials. An example of a good measurement scale for stroke impairment, which is currently recommended (11), is the Fugl-Meyer assessment for post-stroke sensorimotor function (12) (Fig. 2).
Fig. 2. Part of the Fugl-Meyer Motor Assessment Scale for the upper limb.
The 1970s saw the beginning of increasing interest in stroke care. An early report from Sweden dealt with the need for stroke rehabilitation (13), highlighting the needs of individuals of working age. The study showed that only approximately 30–40% of those who survived 6 years after stroke returned to work. There were reports of more intensive care stroke units (14, 15), as well as comprehensive units in which the rehabilitation team was important (16, 17), and of subsequent randomized controlled trials (RCTs) (18–20). The results showed that the stroke unit saved lives and reduced disability (5), and that these gains were also seen up to 10 years after the acute incidence (21).
Stroke damages the brain, with the resulting impairment being related to the localization of the damaged area. Most motor and sensory functions are more localized than are cognitive functions, such as perception, attention, memory and language, which are more distributed in interactive and overlapping networks.
Motor control theory is based on the interaction of the individual’s resources (perception, cognition and action), the nature of the task (stability, mobility, manipulation) and the characteristics of the environment (22). The theory is that there are systems in which higher levels in the nervous system activate lower levels, while the lower levels activate synergies (muscles that act as a unit). It is thought that the person gains motor control through searching for an optimal solution for performing a task. On the basis of this theory, current stroke rehabilitation is individualized, task-specific and goal-oriented (Fig. 3).
Fig. 3. Balance training in man with left hemiparesis. Shifting center of mass in the sagittal plan by moving forwards and backwards.
Discovery of the central gait pattern (23) and, subsequently, the possibility of regaining function through training (24), provided a basis for the idea of providing support for people to enable them to take more steps while walking on a treadmill (25). Studies in Canada (26) and Germany (27), and a multicentre RCT in Sweden (28), however, have divergent results. Meta-analyses, performed by Cochrane (latest update 2017; (29)), which included 56 trials with 3,105 participants, showed that the likelihood of being independent walkers after using treadmill, was no different from those not receiving treadmill training. However, walking speed and walking endurance may improve slightly in the short term and the energy cost may be reduced (30), which could make this an alternative gait training modality.
The idea that the brain can change, i.e. plasticity, was first suggested in the 1980s. Brain plasticity is a broad term for the ability of the brain to change and adapt as a result of environmental pressure, experiences and challenges, including brain damage. An early publication in this area discussed the possible impact of this in stroke rehabilitation (31). However, the implications for rehabilitation did not really take off until later. Nudo & Friel (32) Nudo & Milliken (33) found increased cortical representation of the hand in a monkey with stroke, and the changes that occurred when the monkey had to feed himself with the paretic limb. This led to a wave of studies on constraint-induced movement therapy (CIMT) (34–36). CIMT involves the use of a splint (or similar), which is applied to the intact hand for 90% of the day in order to force use of the paretic hand, combined with ‘’shaping’’ (including verbal feedback) by which the tasks are made progressively more difficult (37). Finally, a large multicentre RCT (38) with a strict training procedure, showed an effect of CIMT on upper extremity function, not only on impairment level, but also in activities of daily living (ADL) (Fig. 4). Modification of this intervention has also shown effectiveness, as stated in a Cochrane review from 2015 (39). The review included 42 studies involving 1,453 participants. CIMT was associated with limited improvements in motor impairment and motor function; however, this did not result in improved function (reduced disability).
Fig. 4. Washing the window using the impaired left hand, with a restraining orthosis on the right hand.
Mirror neurones were discovered in the mid-1980s; first in macaque monkeys and subsequently in humans (40, 41). Mirror neurones are involved in the process of humans understanding the meanings of others while observing their actions; for example, when a person smiles and gets a smile in return. This has implications for stroke rehabilitation; it was shown that when a person watches a hand movement the neurones are activated in the same way as when they actually perform the action (42). This mimicking in the brain is useful when the therapist shows a patient how to accomplish a movement, such as lifting the arm. Looking at the action in a mirror also results in the same activation of neurones as when watching the movement directly. Thus, when a person with stroke uses the mirror to observe a movement they are performing with their better hand, the brain interprets the image as if it is observing the impaired hand (Fig. 5). A Dutch RCT study (43) showed that, in a group of subacute stroke patients, mirror therapy as an add-on to a conventional rehabilitation programme led to improved function in the impaired limb immediately after 4 weeks of treatment, as well as at the 6-month follow-up. A Cochrane review (44) has shown the efficacy of mirror therapy in improving upper extremity function and ADL. Mirror therapy is easy to perform, and can be carried out by patients on their own, or with family, and is not dependent solely on professionals.
Fig. 5. Use of a mirror box. The subject performs movements with their right (unaffected) hand, while the left (impaired) hand is in the box (out of sight). They observe the movements of their right hand in the mirror.
The brain is organized such that the cortical sensory and motor representation of the hand exerts inhibitory influences on the homonymous representation in the opposite hemisphere. This inhibition from the opposite hemisphere is thought to contribute to skilled motor performance. After a stroke, the surrounding intact tissue has an inhibitory effect on the damaged area. In order to increase the activity of the injured area, different neurophysiological strategies have been tried. The 2 most-studied approaches are transcranial magnetic stimulation, TMS (45) and transcranial direct current stimulation (tDCS) (46). In the clinic, 2 approaches for changing the hemispheric dominance have been applied. One approach is to reduce cortical activity on the intact side by applying low-frequency rTMS. Another approach is to enhance activity in the damaged hemisphere. This can be achieved by high-frequency rTMS or anodal tDCS. Anodal tDCS is less focused, but can be applied while performing rehabilitation. There has also been a trial in which the focus was to increase the sensory input by electrical stimulation of peripheral nerves in the impaired upper extremity (47). In theory, the combination of peripheral nerve stimulation with tDCS while performing an activity should enhance the effects of the different components.
Robots are of possible use in stroke rehabilitation. There are 2 main types of rehabilitation robots.
The first is an assistive robot that substitutes for lost movement. An example of this is a wheelchair-mounted robotic, controlled via a switch or other input device or a powered wheelchair. These devices are sometimes used for persons with locked-in syndrome after a brainstem stroke, who may still have very weak muscle function around the eyes or in a finger or toe.
The second type is a therapy robot. Therapy robots are tools for the therapist that That allows the patient to practice with the aid of the robot. There are differences in the construction of these robotic devices. The robots can be divided into exoskeleton and end-effector types, according to their method of supporting and pulling the limb.
Exo-skeleton robots are wearable mobile machines powered by a system of electric motors, pneumatics, levers, hydraulics, or a combination of these. Structurally, exoskeleton robots can be divided into upper limb exoskeleton robots, lower limb exoskeleton robots, whole-body exoskeleton robots, and all kinds of joint correction or restorative training skeletal robots. The limb is enclosed by the robot, which results in the limb movement being performed with the help of the exoskeleton. The level of input provided by the robot to execute the movement can be altered. Most exoskeletal robots in clinical use are for the lower limb. Examples of these devices are the Lokomat®, which requires walking on a treadmill, and the newer device, HAL®, which allows movement on the floor (Fig. 6).
Fig. 6. Gait training using a robot.
The end-effector rehabilitation robot system consists of ordinary connecting rod and series robot mechanism. Here the patient is connected only to the end of the robot. There are end-effector robots in clinical use for both lower and upper extremity training. MIT-Manus® is an example of upper extremity end-effector training robot. G-EO® gait trainer is a device for the lower limb, where only the feet are fixated in the working state, the robot drives the movement of the upper limbs by connecting with the patient’s arm to achieve the rehabilitation training.
There have been a number of small positive studies with the different modalities for both upper and lower limbs. However, the results of meta-analyses are not as convincing.
Electromechanical arm and hand training in combination with other occupational therapy or physical therapy for impaired arm and hand mobility after stroke has the following effects (48):
There is no scientific evidence to assess the effect on pain, muscle tone, joint mobility, quality of movement, participation, or quality of life.
Electromechanical walking training in combination with other physiotherapy in case of impaired walking ability after stroke has the following effects (49):
The burden of stroke in Europe
The Stroke Alliance for Europe (SAFE) is an organization of different patient organizations from all over Europe. Together with King’s College, London, they launched the Burden of Stroke in Europe in 2017. The report, based on governmental statistics, shows large disparities between and within countries along the entire stroke care pathway. For many countries, there is very little information on the rehabilitation therapies that stroke survivors receive, especially once they have left hospital. Quality control of rehabilitation services is scare. Rehabilitation services are usually unevenly distributed and vary in quality. Specialist rehabilitation may be available only in large urban areas. In many countries, occupational therapy and psychological support are either very limited or not available. Capacity is lacking in rehabilitation centres, as well in the communities, which leads to long delays in starting rehabilitation. Reports from the Swedish quality registries “Riksstroke” and “WebRehab”, show variation in services within Sweden.
The European Stroke Organisation (ESO) and SAFE made a joint effort to launch the European Stroke Action Plan (ESAP). The aim of the ESAP is to produce a roadmap and define goals for the treatment of stroke in Europe through to 2030. The ESAP includes 7 domains: primary prevention; organization of stroke services; management of acute stroke; secondary prevention; rehabilitation; evaluation of stroke outcome and quality assessment; and life after stroke.
The ESAP includes an overview of state of the art in the union and tries to identify the areas where rehabilitation is lacking.
The goals defined by ESAP are (50):
Stroke units
A stroke unit is a geographically identifiable unit in a hospital, which is devoted entirely (or almost entirely) to stroke care. The stroke unit is staffed by a multidisciplinary team with specialist knowledge of stroke care, and consists of the components described below.
The stroke unit contains 3 elements (51):
The stroke unit has established a programme for interventions to meet common problems among patients with stroke and for recording quality of care. It provides detailed information and educates patients and next-of-kin during the hospital stay. The comprehensive stroke unit has been shown to have a major impact on outcome after stroke. It has no side-effects and is beneficial for all types of stroke, stroke severity and ages of patients. In addition, cognitively impaired stroke patients benefit from stroke unit care.
Early supported discharge
Early supported discharge (ESD) (52) is an innovative approach to rehabilitation, in which services are provided at home by a mobile rehabilitation team, and should be regarded as a part of the stroke treatment path-way. Multidisciplinary, specialist stroke ESD teams should plan and co-ordinate discharge from hospital and provide rehabilitation in the community (53). The target audience is mainly patients with mild or moderate stroke symptoms, which includes approximately 30% of the stroke population in most settings. Meta-analyses (52) show that reduces the length of hospital stay and reduces the odds of dying due to stroke or being dependent after stroke by 20%. However, another study evaluated the real-world aspects (ecological validity) of ESD (54) and the results were similar, with significantly shorter lengths of hospital stay and reported significantly higher levels of satisfaction with services received (54). The carers also experienced the ESD as positive (Fig. 7).
Fig. 7. Gait training outside the home after early supported discharge.
Slow-stream rehabilitation
Approximately 50–70% of stroke patients have a moderate to severe stroke. They also need access to stroke rehabilitation, either during a prolonged stay in hospital or with adequate rehabilitation to address their needs in the community. With continued recovery, there is an increase in stamina, and the intensity of training may increase. Stroke survivors are often physically deconditioned, with muscle weakness in both the affected and unaffected sides, and reduced cardiorespiratory fitness. Physical fitness training after stroke has many benefits (55). It reduces disability, improves walking ability, and may improve other stroke-related deficits, such as cognition, mood and fatigue. Patients with aphasia and better stamina can receive high-intensity speech training over a long period. This type of training has been shown to improve functional communication (56). ADL training, provided in the home-setting after discharge until 1 year after stroke, has also been shown to have a beneficial effect (57).
Back into life
The ultimate goal for rehabilitation is for the person who needs rehabilitation, to be living a life again with quality. The World Stroke Organization (WSO) has stated a priority to identify and evaluate the best ways to address and improve life after stroke (58). Patient organizations have launched the Global Stroke Bill of Rights (59), in which the importance of longer-term support is highlighted.
Reports from stroke survivors show that they experience unmet needs in terms of communication, social relationships, loneliness, fatigue and finances (60), as well as lack of rehabilitation (61). It is estimated that approximately 25% of strokes occur in people of working age (62), 18–65 is what has been applied in most studies whose needs may also include support to return to work (63–65).
The burden of stroke, both for society and for individuals, is high. The consequences for individuals vary, depending on the type of stroke, its severity, and location, and on the person’s life situation. The need for rehabilitation is often not met, due to restricted resources and their uneven distribution. This means that the rehabilitation delivered needs to be adapted to the individual, as well as to the society in which they live. Increasing knowledge of neurophysiology and evidence from meta-analyses will lead to continuing changes to rehabilitation in practice. With continued willingness to change, stroke rehabilitation providers can continue to make a difference and improve the lives of stroke survivors.


 Click to show fullsize
Click to show fullsize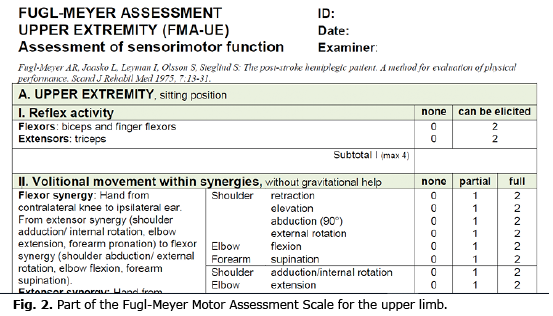 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize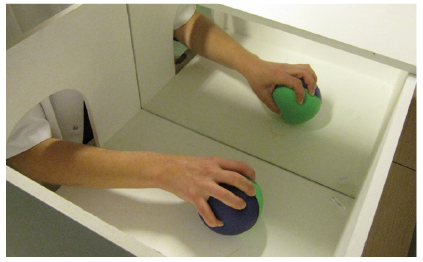 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize