
From the Department of Clinical Neuroscience, Institute of Neuroscience and Physiology, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
Objectives: To examine the relationship between, and impact of, level of physical activity and perceived impact on life at 12 months post-stroke.
Design: Cross-sectional study.
Subjects: A total of 73 participants with first-time stroke included in the Stroke Arm Longitudinal study at the University of Gothenburg (SALGOT study), Sweden.
Methods: Perceived impact of stroke was assessed with the Stroke Impact Scale and level of physical activity was assessed with the Saltin-Grimby Physical Activity Scale at 12 months post-stroke. Data were presented with descriptive and logistic regression analyses.
Results: The physically active group perceived their strength, emotion, mobility, participation and overall stroke recovery as significantly less problematic compared with the inactive group. Being physically active contributed to higher scores in the Strength domain (odds ratio, OR 7.89) and in the Stroke Recovery domain (OR 18.55). In the Participation domain being physically active (OR 8.01) and independent (OR 0.162) contributed to higher scores.
Conclusion: A positive correlation was found between level of physical activity at 12 months post-stroke and levels of strength, participation and stroke recovery.
Key words: cerebrovascular accident; exercise; rehabilitation; self-concept; recovery of function; Stroke Impact Scale.
Accepted Mar 3, 2020; Epub ahead of print Mar 16, 2020
J Rehabil Med 2020; 52: jrm00056
Correspondence address: Peta Cook, Research Group of Rehabilitation Medicine, Per Dubbsgatan 14, Floor 3, 41345 Gothenburg, Sweden. E-mail: peta.cook@vgregion.se
It is common for stroke survivors to experience long-term symptoms. This study investigated individuals’ perceptions of how stroke symptoms impact on their lives, and examined the connection between this and their level of physical activity 12 months after stroke. A total of 73 stroke survivors completed 2 questionnaires; about their level of physical activity, and their perception of how their life is impacted by stroke. The results showed that a higher level of physical activity at 12 months after stroke was linked to stroke survivors perceiving that their strength, participation in life and overall recovery from stroke was better. This study highlights the importance of being physically active even long-term after stroke, as this can help to optimize the perception of recovery and reduce the impact of stroke on life.
Physical activity (PA) has many health benefits, such as reducing the risk of heart disease, cancer and stroke (1). An adequate level of PA for adults is defined as a minimum of 150 min/week of moderate intensity aerobic activity together with regular strength training (2), either through structured activities or incidental PA. However, despite worldwide promotion of PA (1), not only does inadequate PA remain one of the 5 most preventable risk factors of stroke, PA levels post-stroke are lower than in the comparable healthy population (3).
Stroke symptoms are many and varied; for example, reduced motor function, coordination, sensation and cognitive function (4). Strong evidence has been found for the use of task-specific training within stroke rehabilitation in order to improve functions such as muscle strength, walking ability and aerobic fitness (5–8). Research has also found that higher levels of PA alone can improve functional skills, such as walking ability, balance and physical fitness post-stroke (3). However, conversely, research has shown that physical function alone cannot explain the level of PA post-stroke (9–11).
Examining outcomes post-stroke is complex and, as discussed by the International Classification of Func-tion, Disability and Health (ICF), examining multiple dimensions of health is critical (12). Multidimensional measurement tools, such as the stroke-specific Stroke Impact Scale (SIS) (13, 14), which examines varied outcomes such as function, activity levels and participation levels, and are essential in order to examine recovery post-stroke. Furthermore, it is well established that individual perception of health is important (15), which supports the use of self-rater scales such as SIS.
Increased PA has many physical and psychological benefits post-stroke (3, 8, 16, 17). However, energy expenditure has been shown to be higher in the stroke population (18), which in turn could support a hypothesis that higher levels of PA lead to increased fatigue and the consequential perceived impact of stroke on life is greater. It is thus important to develop an improved understanding of the relationship between level of PA and self-perceived impact of stroke on life, as it can have a significant impact on long-term stroke rehabilitation.
The aim of this study is to examine the relationship between, and impact of, level of PA and perceived impact on life at 12 months post-stroke.
During an 18-month period (2009–2010) individuals with first-time stroke who were cared for at the stroke unit of Sahlgrenska University Hospital were included consecutively into the Stroke Arm Longitudinal Study at the University of Gothenburg (the SALGOT study) (19).
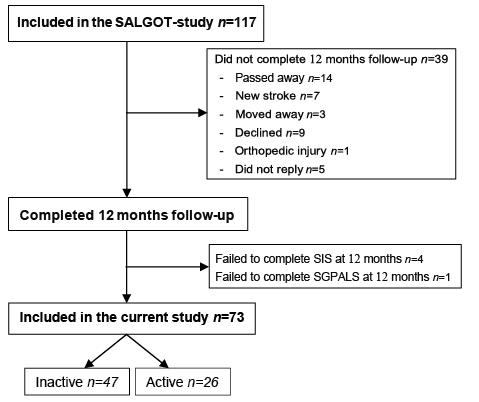
Inclusion from the SALGOT study (19) were patients who were: diagnosed with a first-time stroke; had reduced arm and hand function on day 3 post-stroke according to the Action Reach Arm Test (ARAT), with a maximum score of 57; were admitted to the stroke unit within 3 days of onset of stroke; were living in the Gothenburg urban area (maximum 35 km from Sahlgrenska University Hospital); and were over 18 years of age. The exclusion criteria were: previously reduced function in the upper limb prior to stroke (due to injury or other condition); and non-Swedish speaking prior to stroke (19). Further inclusion criteria for the current study included: completion of both Saltin-Grimby Physical Activity Level 6-Scale (SGPALS) (20, 21) and SIS at assessment 12 months post-stroke. This resulted in a total of 73 participants (see Fig. 1).
Fig. 1. Flow chart of the patient selection procedure, starting from the Stroke Arm Longitudinal Study at the University of Gothenburg (SALGOT study) population, and thereafter describing the flow of inclusion in the current study, at 12 months post-stroke. SIS: Stroke Impact Scale; SGPALS: Saltin-Grimby Physical Activity Level Scale.
The perceived impact of stroke was assessed with the self-assessment questionnaire SIS 3.0 (14). The SIS is used to assess the individual’s perceived impact of stroke in 59 items, across 8 different domains (strength, memory, emotions, communication, activities of daily living, mobility, hand function and participation). Each item was scored in an ordinal scale (1–5), and summarized to a domain score. Each domain score was transformed using the following equation: domain score= (mean item score–1)/5–1 × 100, with each domain receiving a final total score out of 100 (14). SIS also includes one final question regarding overall stroke recovery (SR), scored 0–100 in a visual analogue scale (VAS). In the present study domains 1 (strength), 3 (emotion), 6 (mobility), 8 (participation), and SR were selected for analysis, as these domains are expected to be closely related to PA.
At 12 months post-stroke participants measured their level of PA during the past 6 months using SGPALS, a self-assessed 6-grade ordinal scale, ranging from physically inactive to an elite level of PA and training (20, 21). Based on the level of PA at 12 months the study population was divided into 2 groups: an inactive group (equivalent to SGPALS 1–2) and an active group (equivalent to SGPALS 3–6) (21).
Sociodemographic data from the time of onset of stroke was used to describe the population.
Medical data from the acute stages was collected via the patients’ medical record as well as being supplemented by Riksstroke (The Swedish Stroke Register) (19, 22). Medical data included type of stroke (ischaemic or haemorrhagic) (23), and level of dependency (24). Level of dependency in activities of daily living was measured by modified Rankin Scale (mRS) (25) at time of discharge from hospital.
Variables that are shown to be important for PA and/or stroke outcome were assessed in the study; including age (24), sex (26), smoking status (“yes” corresponds with ≥ 1 cigarette/day, or quit during the last 3 months) (27), previous cerebrovascular disease (CVD) (“yes” corresponds to diagnosis of at least one of the following diseases prior to stroke: heart failure, ischaemic heart failure, hypertension, angina, hypercholesterolaemia, aortic insufficiency, atrial fibrillation, myocardial infarct, prosthetic heart valve, or rheumatic valvular heart disease) (27), living arrangements (“living alone” or “sharing household with another adult”) and occupational status (“working” ≥75% full-time work, or “not working” <75%) (28).
All assessments were completed by 3 experienced physiotherapists in a standardized procedure (SALGOT protocol) (19).
Data analysis
Differences between groups (active and inactive) in demographic data were analysed using Fisher’s exact test and Mann–Whitney U test. The level of significance was set as p-value < 0.05.
Raw responses from SIS were initially dichotomized into 1–3 representing “problematic” symptoms, and 4–5 “not problematic” symptoms (14, 29). Based on this, the median score between 3 and 4 was calculated to be 62.5 and final dichotomization of the SR VAS score was dichotomized into 0–62 and 63–100.
Logistic regressions were used to examine the relationship between the different domains of SIS (dependent variable) and the level of PA (independent variable). The initial cross-tabulation of each SIS domain with PA was conducted, and in the case of poor distribution (with fewer than 5 in a box) the variable was excluded from further analysis. Spearman’s rank-order correlation (rho) was used to check all variables potentially included in the models, with rho set to rho ≥ 0.7 (30). If rho ≥ 0.7, the variable was excluded from further analyses. In order to identify significant variables for further analysis, univariate regression of all remaining variables was completed with a significance level of p < 0.25, using Wald’s test. Multivariate logistic regression was completed with the significant remaining variables (with p < 0.25). Previously excluded variables were then reinserted in the multivariate regression with level of significance set at p < 0.05 (Fig. 2). Resulting models were analyzed with: Omnibus test (significance < 0.5); Nagelkerke R square and Cox & Snell R-square test; as well as receiver operating characteristics (ROC) curves to assess for goodness of fit (30). Statistical analysis was completed using the IBM Statistical Package for Social Sciences (SPSS version 21.0, for Windows).
Ethical issues
Written information and consent was collected from all participants or from their closest relative. The SALGOT study applied for and was granted ethical approval by the Regional Ethics Testing Board in Gothenburg (5 May 2008, diary number 255-08) and the Declaration of Helsinki follows. The SALGOT study is registered on ClinicalTrials.gov (NCT01115348).
A total of 73 participants were included in the study (Fig. 1). The participants’ mean age at stroke onset was 66.8 years (standard deviation (SD) 12), and 82.2% had an ischaemic stroke (Table I). Of the participants with ischaemic stroke, 9 received thrombolysis and one received thrombectomy. When comparing the active and inactive groups significant differences were present in age (p < 0.001), level of dependency (mRS) (p = 0.001) and working status (p = 0.002) (Table I).
Table I. Clinical characteristics of the population according to level of physical activity, n = 73
Participants in the active group perceived their strength, emotion, mobility, participation and SR as significantly less problematic compared with the inactive group (Table II).
Table II. Number of participants corresponding to Stroke Impact Scale (SIS) domains divided into level of physical activity at 12 months
Three of the 5 chosen SIS domains had sufficient data to build regression models; these were Strength (SIS-1), Participation (SIS-8) and SR (Fig. 2). No variables were found to correlate (rho ≥ 0.7) in any of the models, and all variables thus continued to the univariate regression models (Fig. 2). In the domain of Strength and SR, PA was the only independent variable that contributed to the final model, with odds ratio (OR) of 7.98 (SIS-1) and 18.55 (SR) (Table III). In the Participation domain the final model included PA (OR 8.01) and level of dependency (OR 0.162) (Table III). Nagelkerke R square and Cox & Snell R-square indicated that 19.3–26.5% of variation in the outcome SIS-1, 24.3–32.6% of the variation in outcome SIS-8, and 31.5–43.6% of the variability in SR was explained by their corresponding models.
Table III. Logistic regression modelling improvement in Strength, Participation and Stroke Recovery
Fig. 2. Flow chart of the analysis procedure for each Stroke Impact Scale (SIS) domain: starting at cross-tabulation, followed by each step of logistic regression analysis, and finally displaying the resulting models for each domain. CVD: cardiovascular diseases; PA: physical activity.
This study examined the relationship between a PA and self-perceived impact of stroke, as measured by SIS, at 12 months post-stroke. The study found that PA has a significant and positive correlation with perceived strength (SIS-1) and overall stroke recovery (SR) at 12 months post-stroke. Furthermore, PA combined with level of dependency has a significant and positive correlation with perceived participation (SIS-8) at 12 months post-stroke. That is, participants with a higher level of PA reported a lower perceived impact of stroke on their life at 12 months post-stroke, according to these 3 SIS domains.
The results of the current study imply that assisting stroke survivors to be physically active can have a positive impact on their life, as it is correlated with an increased perception of participation long term post-stroke. A recent study (31) established that SIS-8 (participation) is sensitive to change over time, finding that almost 50% of their study population had a meaningful positive or negative change in this domain between 3 and 12 months post-stroke. This strengthens the reliability of SIS-8 and thereby supports our findings.
Guidetti et al. (31) found that SR, as measured by SIS, was significantly better at 12 months in comparison with 3 months post-stroke. This could not be explained by level of dependency, age or sex, nor could it be explained by changes in other SIS domains. In the current study the outcome of SR could not be explained by age, sex, type of stroke, CVD, or living arrangements. A significant correlation was, however, found between perception of overall SR and higher level of PA. This once again highlights the importance of ensuring stroke survivors achieve an adequate level of PA even long-term post-stroke.
All 3 areas of SIS that the present study examined demonstrated a positive relationship between a higher level of PA and a lower level of perceived impact of stroke on life. As mentioned in the background, the stroke population have been found to have a higher energy expenditure compared with the normal population (18). However, our findings oppose the hypothesis that higher levels of PA would lead to greater energy loss, increased fatigue, and thus increased impact of stroke on life.
Multidisciplinary rehabilitation post-stroke has also been shown to be essential in order to minimize long-term symptoms and is optimized with early team input (32). Furthermore, in order to improve long-term levels of PA post-stroke, individualized and client-centred interventions have been found to be beneficial (6). Stroke rehabilitation is complex, and this study’s findings support a continued emphasis on assisting stroke survivors to achieve an adequate level of PA long-term post-stroke.
This study has some limitations. It is important to recognize that variables other than those examined may have impacted on outcomes, such as cultural and religious differences. The SALGOT study was an observational study with participants with initially impaired upper extremity function, who received standard Swedish rehabilitation and care. This may have influenced results and should be kept in mind when interpreting the results of this study. A larger study sample could have made it possible to complete analysis of all intended SIS domains and could have minimized any significant differences between included and excluded groups. The participants included in the study were younger than the non-included, which could be explained by the study being conducted 12 months post-stroke and older people generally having a lower survival rate post-stroke (33). However, elderly people are also found to be less active in general (34), and thus with a comparatively younger study group this could affect the results.
Conclusion
The results of this study show that PA at 12 months post-stroke has a significant and positive correlation with perceived strength and stroke recovery. Furthermore, PA combined with level of dependency is significantly and positively correlated with perceived participation at 12 months post-stroke. This is critical information within rehabilitation, and particularly within physiotherapy, where much focus is placed on encouraging and assisting stroke survivors to increase their level of PA. This is an important clinical finding, as it provides evidence for encouraging an active lifestyle post-stroke, with the knowledge that it can help survivors to increase their perceived strength, participation and stroke recovery post-stroke.
This project was funded by Greta and Einar Askers Foundation and The Local Research and Development Board for Gothenburg and Södra Bohuslän. The SALGOT study was supported by grants from the Swedish Research Council (VR 2012-70X-22122-01-3), the Swedish Research Council (VR 2017-00946), the Swedish Heart-Lung Foundation, the Swedish Brain Foundation, Promobilia, and the Swedish Stroke Association.
The authors would like to thank Margit Alt Murphy and Eva-Lena Bustrén for their work with data collection and the Riks-Stroke Collaboration for help with demographic data.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize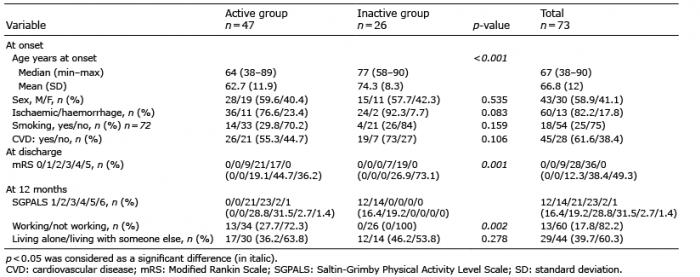 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize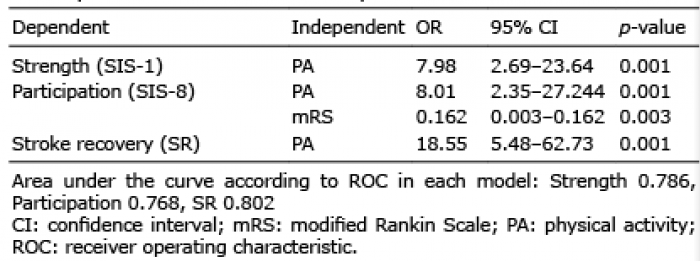 Click to show fullsize
Click to show fullsize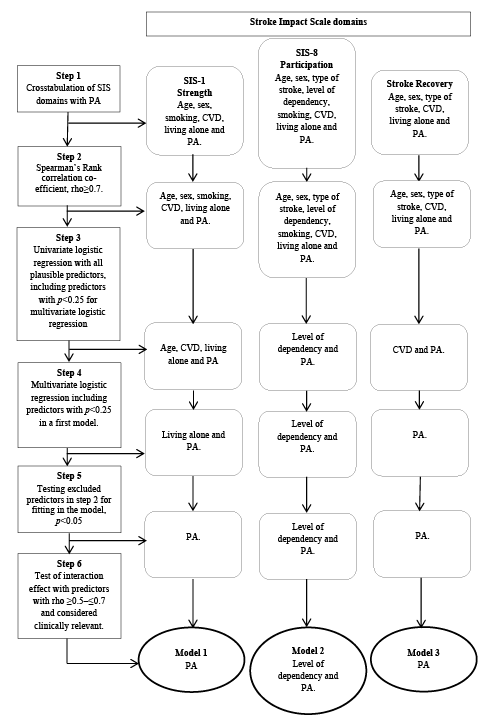 Click to show fullsize
Click to show fullsize