
From the 1Norwegian National Advisory Unit on Pregnancy and Rheumatic Diseases, St Olavs Hospital, Trondheim University Hospital, 2Department of Public Health and Nursing, Norwegian University of Science and Technology and 3Department of Rheumatology, St Olavs Hospital, Trondheim University Hospital, Trondheim, Norway
Objectives: To investigate if an intensive rehabilitation programme, including intensive exercise and patient education, for young adults with inflammatory arthritis, conducted in a warm climate, has long-term effects on general health status compared with usual care.
Design: Open randomized controlled trial.
Patients: A total of 64 patients with inflammatory arthritis, aged 20–35 years.
Methods: Patients underwent randomized allocation to an intensive 17-day rehabilitation programme in a warm climate (intervention group) or to usual care with no structured rehabilitation (control group). The primary outcomes were physical function, assessed by the “30-second Sit to Stand test”(30sSTS), and coping, measured by the “Effective Musculoskeletal Consumer Scale” (EC17).
Results: A total of 64 patients (mean age 27.5 years, 62.5% female) were randomized. Thirty out of 32 patients completed the intervention. At 12-month follow-up, 7 patients were lost to follow-up; 4 from the intervention group and 3 from the control group. The intervention group showed significant improvement in the physical function test at 3 months; estimated mean difference (95% confidence interval): 5.5 (2.8–8.1), 6 months 3.6 (0.4–6.8) and 12 months 4.0 (0.0–7.9), compared with the control group. There were no differences in coping between the 2 groups at 3, 6 or 12 months.
Conclusion: Rehabilitation in a warm climate improves physical functioning, but not coping, in young adults with inflammatory arthritis.
Key words: rehabilitation; young adult; exercise; patient education; warm climate.
Accepted Mar 5, 2020; Epub ahead of print Mar 12, 2020
J Rehabil Med 2020; 52: jrm00040
Correspondence address: Ingrid Rekaa Nilssen, Norwegian National Advisory Unit on Pregnancy and Rheumatic diseases, St Olavs Hospital, Trondheim University Hospital, Postboks 3250 Torgarden, 7006 Trondheim, Norway. E-mail: Ingrid.Rekaa.Nilssen@stolav.no
The aim of this study was to investigate if an intensive rehabilitation programme, including intensive exercise and patient education, developed for young adults with inflammatory arthritis, conducted in a warm climate, has long-term effects on general health status compared with usual care. A total of 64 participants, aged 20–35 years, were assigned to an intervention group (n = 32) or control group (n = 32). The intervention
group participated in a 17-day rehabilitation programme (intensive exercise, individual physiotherapy and patient education) in a warm climate. The control group received usual care with no structured rehabilitation. The intervention improved patient’s physical function, but not coping, up to 1 year post-intervention, compared with usual care.
Inflammatory arthritides (IA), such as rheumatoid arthritis (RA), axial spondyloarthritis (AS), psoriatic arthritis (PsA) and juvenile idiopathic arthritis (JIA) often cause symptoms of joint pain, stiffness and fatigue among others, usually with a fluctuating and unpredictable pattern (1). Even though the prevalence of IA, in general, is higher in older adults, a significant number of young adults are diagnosed with IA (2). Young adults are typically in a stage of life where they are choosing their educational path, establishing a career, finding a partner, and starting a family, and the consequences of having a chronic disease at this stage can be significant (3, 4).
Despite major improvement in pharmacological treatment for patients with IA in recent years (5), their quality of life, generic health status and functional ability are negatively influenced by their disease (4, 6, 7). They are also less likely to be employed than their healthy peers (8). Non-pharmacological interventions, such as multidisciplinary rehabilitation including exercise and patient education, are considered an important adjacent treatment for patients with IA (9–11).
Rehabilitation in warm climate has long been an established non-pharmacological treatment for patients with IA in the Nordic countries (12). These programs typically last four weeks and the main components are usually intensive exercise and physiotherapy in warm climate, combined with patient education. A systematic review published in 2010 concluded that there was evidence of low to moderate quality that comprehensive rehabilitation in warm climate lead to reduction in disease activity, pain, fatigue and global disease impact for patients with IA up to three months after discharge (12). Warm climate was here defined as a dry climate with several hours of sunshine and a mean temperature of > 20 °C during a minimum of 8 months a year. More recent studies have also concluded that rehabilitation in Mediterranean climate has beneficial effects on various health outcomes (13, 14).
However, the rehabilitation programmes mentioned above (12–14) were not tailored to the special needs of young adults. Inpatient rehabilitation programmes in general often last several weeks. For young adults, it can be especially challenging to be away from home for an extended period; often due to studies, starting a career or family-life with small children (15). Young adults emphasize that rehabilitation should focus on issues that are especially relevant for young adults and prefer to participate with people of their own age (15). Despite these apparent needs, rehabilitation offered for young adults with chronic disease in Norway is still inadequate (15).
To our knowledge, no studies have investigated the effect of rehabilitation especially developed for young adults with IA. The objective of the current study was therefore to investigate if an intensive 17-day long rehabilitation programme in a warm climate targeted at young adults with IA could improve general health status after 12 months, compared with usual care.
Trial design
This was an open 12-month, 2-group, parallel, randomized controlled trial with a 1:1 allocation ratio. Data collection lasted from June 2015 to September 2017. The study was approved by the Norwegian Regional Committees for Medical and Health Research Ethics (nr. 2015/413), and all participants provided written informed consent. The study has been conducted in accordance with the Declaration of Helsinki. The protocol was registered at ClinicalTrials.gov (study ID number NCT02430402).
No changes were made to methods or study protocol after trial registration.
Participants
Patients diagnosed with IA (documented in their hospital record), aged between 20 and 35 years, with a need for rehabilitation as perceived by their treating rheumatologist or nurse were eligible for the study. Exclusion criteria were: (i) not being independent in activities of daily living, or (ii) having comorbidities that would restrict their ability to participate in the rehabilitation programme, e.g. serious cardiovascular disease, severe lung disorder, chronic open wounds, serious psychiatric disorders, substance abuse and intolerance for sun/heat.
Patients were recruited from 3 rheumatology outpatient clinics in Central Norway. Clinical Rheumatologists and nurses in these outpatient clinics were informed of the study, and recruited eligible patients during their regular outpatient appointments. There was no registration of the number of persons asked, as this would increase the workload of the clinicians. The study nurse then contacted patients who wanted to participate. An appointment at the outpatient clinic at St Olavs Hospital, Trondheim University Hospital, Norway was made, and the patients were screened to ensure that they met the inclusion criteria.
Intervention
The intervention took place at Rheuma-Sol, a treatment centre in southern Spain, owned by the Norwegian Rheumatism Association (16). The area where this centre is located is defined as having a Mediterranean climate. There were 3 intervention groups with 10–12 participants in each. The intervention took place at the following dates; group 1: 9–27 June 2015, group 2: 11–29 August 2015, group 3: 16 August–3 September 2016. The intervention consisted of exercise and patient education, as detailed below.
Exercise. The main component of the intervention was intensive individualized exercise with guidance of experienced physiotherapists. A doctor, nurse and physiotherapist evaluated the participants’ condition to individualize their exercise plan on the first day. There were 3 daily group exercise sessions on weekdays. The morning exercise (30 min) focused mainly on stretching and mobility. The midday exercise (45–60 min) took place in the indoor gym with varying focus, such as cardio, strengthening, balance and mobility. The afternoon exercise (60 min) was an aquatic class, also focusing on cardio, strengthening, balance and mobility. The participants also had 30-min individual physiotherapy every weekday, tailored to the participants needs, with active and passive treatments. There were no exercise groups at weekends. The participants had access to exercise equipment and the pool for additional voluntary exercise.
Patient education. The other component of the rehabilitation programme was 5 group sessions of patient education. The sessions were delivered by physiotherapists and nurses, lasted for 45–60 min each, and covered areas such as physical activity, coping with pain, coping with everyday stress, sleep, sleep deprivation and nutrition/diet. The patient education sessions were mainly given as lectures, with room for discussion and reflections.
Control group. The control group did not participate in structured rehabilitation; they only received treatment as usual. This included routine consultations at the rheumatology outpatient clinic or their general practitioner (GP), as needed, voluntary community based physiotherapy and medication as usual. The participants, however, had no restrictions concerning participating in other non-pharmacological interventions during the study period, e.g. patient education, exercise or rehabilitation programmes, conducted independently of this study.
Outcome measures and data collection
This study used a national core outcome set developed to evaluate rehabilitation programmes for patients with rheumatic and musculoskeletal diseases (RMD) (16). The set consists of 9 valid and reliable self-reported outcomes measuring important health aspects that can be affected by rehabilitation. These include pain, fatigue, physical fitness, mental health, daily activities, goal attainment, social participation, quality of life and coping (16). We chose the 30-s Sit-to-Stand Test (30sSTS), a measure to assess physical capacity (17) and the Effective Musculoskeletal Consumer Scale (EC17) a measure assessing coping (18), as the predefined primary outcomes. The other outcomes in the core set were chosen as secondary outcomes. These were the Patient Specific Functional Scale (PSFS) , Hannover Functional Ability Questionnaire (FFbH) , Hopkins Symptom Checklist (HSCL-5) , EQ5D-5L (VAS scale and index score, the EQ-5D-5L Crosswalk Index Value Calculator, with the Danish values set has been used in this study) (19), Coop Wonka functional health assessment charts , and Numeric Rating Scale fatigue and pain (16).
Attendance to the various components of the intervention was recorded to assess implementation
All outcomes were assessed at baseline, and at 3, 6 and 12 months after completed intervention. Data collection was undertaken at the Department of Rheumatology at St Olavs Hospital, Trondheim, Norway. The 30sSTS was assessed by a study nurse. All other outcomes were self-reported questionnaires.
Randomization, allocation and blinding
Participants were randomized to the intervention and control groups after the baseline data collection using a web-based computerized randomization system administered by the Unit of Applied Clinical Research, Institute of Cancer Research and Molecular Medicine, at the Norwegian University of Science and Technology, Trondheim, Norway. The system used block randomization and the size of the blocks was unknown to all persons involved in the study. There was no stratification and the study nurse immediately informed the participants of the randomization outcome. As this was an open trial due to the type of intervention, the therapists, assessors and participants were not blinded.
Statistical analysis
No formal sample size calculation was performed, due to the predefined number of persons that could be included in the trial for economic reasons.
Statistical analyses were performed using IBM SPSS version 23, and carried out for observed data, with no data imputation. All analyses followed the intent-to-treat principle. All outcome variables were tested for normality, with formal normality test, as well as QQ plots and histograms. For the variables with indications of non-normal distribution and outcome measures based on ordinal scales, both parametric and non-parametric tests were performed.
Variables with indications of non-normal distribution and outcome measures based on ordinal scales are presented with the results from the non-parametric tests, with median and interquartile range.
Within-group differences were tested with paired t-test, and Wilcoxon signed-rank test as the non-parametric alternative. The within-group test was conducted by comparing each outcome time-point with the baseline value.
Between-group differences were analysed using analysis of covariance (ANCOVA) with the baseline value as a covariate, and with Mann–Whitney U test as the non-parametric alternative.
A p-value < 0.05 was considered statistically significant.
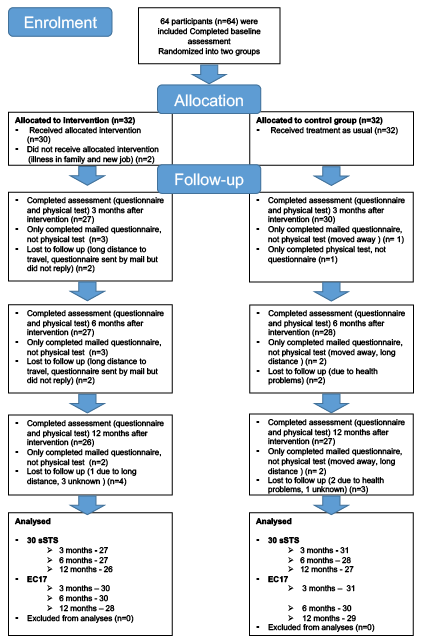
A total of 64 participants were included in the study; 32 in the intervention group (IG) and 32 in the control group (CG) (Fig. 1). Two participants dropped out prior to the intervention for personal reasons; thus 30 of the 32 patients in the IG received and completed the intervention. At 12 months follow-up, 53 out of the total sample (26 in the IG and 27 in the CG) were analysed for the 30sSTStest and 57 (28 in the IG and 29 in the CG) were analysed for the EC17 outcome.
Fig. 1. Flowchart of patient enrolment, allocation, follow-up and analysis.
Baseline characteristics
The total sample consisted of 63% females and 37% males, with a mean age of 27.6 (SD 5) years (Table I). Disease duration varied from newly diagnosed (within the last year) to 33 years. The majority of participants (84%) were using disease-modifying anti-rheumatic drug (DMARD) at baseline, including both biologic and synthetic DMARDs. Many (53%) also used either non-steroidal anti-inflammatory drugs/COX-2 inhibitors (NSAIDS/COXIBs) or other analgesics within the last week prior to baseline. Thirty-six percent of participants were either unemployed, on sick leave, or on disability pension.
Table I. Baseline characteristics
Implementation of intervention
Participation in the various parts of the intervention was high, with the following attendance rates for the various components; morning exercise 97%, midday exercise 94%, aquatic class 90% and patient education 98%.
Outcomes
The results of the intention to treat analysis are shown in Table II.
Table II. Results (main outcomes) from within- and between- (in italics) group ITT analysis. The values are observed mean (within-group) or estimated mean difference (between-group) with 95% confidence interval (95% CI)
Primary outcomes
The analyses showed a statistically significant difference between the IG and CG at all follow-up time-points in physical function assessed by the 30sSTS (Table II, Fig. 2). Estimated mean difference with 95% CI was 5.5 (2.8–8.1, p < 0.001) at 3 months, 3.6 (0.4–6.8, p = 0.028) at 6 months and 4.0 (0.0–7.9, p = 0.05) at 12 months.
There were no statistically significant differences between the IG and CG at any of the follow-ups with regards to coping, measured with the Effective Consumer Scale 17 (EC17). There was also no change within the IG, but the CG had a significant within-group change at 3 (p = 0.007) and 6 months (p = 0.006) compared with baseline.
Fig. 2. Mean number of repetitions in the 30-Second Sit-to-Stand test (30sSTS) at baseline, 3, 6 and 12 months.
Secondary outcomes
At 3 months, the analyses showed statistically significant improvements within the IG in the following outcomes (all in favourable direction); EQ5D5L VAS, FFbH, and CoopWonka physical. The CG had significant within-group difference in PSFS and EQ5D5Lindex.
At 6 months, no significant improvements were seen in the IG in any of the secondary outcomes. However, there were significant between-group differences in favour of the CG in the following outcomes: CoopWonka–Change and VAS fatigue. The control group also had significant within-group improvement in PSFS, EQ5D5L index, FFbH, CW-Change, VAS fatigue and VAS pain.
At 12 months, neither the IG nor the CG showed any significant within-group change in any of the secondary outcome measures compared with baseline (see Table III for details).
Table III. Results from within- and between- (in italics) group ITT analysis. The values are medians with interquartile range. Within-group differences is analysed with Wilcoxon signed-rank test. Between-group differences are analysed with Mann–Whitney U test. Values in bold indicate a p-value < 0.05
The intensive 17-day rehabilitation programme in a warm climate developed specifically for young adults with IA had a long-term effect on physical function, but not on coping. There were no effects on any of the secondary outcomes at 12 months.
Physical function
When comparing the mean value of repetitions in the 30sSTS at baseline (13.4 vs 13.0, IG vs CG) with reference values for healthy women and men between 18 and 29 years of age (26 and 27, respectively) (20), this study shows that the participants had reduced physical ability and low body strength. At 12 months, the IG had increased the mean value of repetitions from 13.2 to 20.2, indicating that an intensive rehabilitation programme in a warm climate is beneficial for young adults with IA.
To our knowledge, no other studies on rehabilitation in a warm climate have used the 30sSTS as an outcome measure, making direct comparison difficult. Other studies (13, 21) have used different performance measures for physical function, such as the 6-Minute Walk Test (6MWT) when comparing a 4-week rehabilitation programme in warm and cold climates. These studies found significant improvement (p = 0.001) in both groups after 16 weeks. Another study has, however, found that these 2 outcome measurements (30sSTS and 6MWT) have a statistically significant correlation, and suggest that the 30sSTS can be used as an alternative to the 6MWT as a measurement of physical performance and functional capacity (22). Thus, both our findings and the findings from other studies (13, 21) strongly indicate that rehabilitation in both warm and cold climates is effective in improving performance-based physical function in the short and long term.
Despite this significant improvement in performance-based physical function, we found no between-group differences in the outcomes measuring self-reported physical function (PSFS, FFbH and CoopWonka-phsycial) at any of the follow-up times in the current study. The IG did, however, show a significant within-group change in FFbH and Coop Wonka-physical at 3 months, although this change was not sustained at 6 and 12 months follow-up. Comparing performance-based physical function with self-reported functional status is important, as the purpose of rehabilitation for patients with IA is not only improvement in physical parameters, such as strength and endurance, but also better overall functioning and improved ability to perform tasks of everyday living (23). However, due to many different measures used for assessing self-reported physical function, the comparisons between studies on the effect of rehabilitation specifically tailored to patients with IA is somewhat difficult. One study on rehabilitation in a warm climate found improvements in Modified Health Assessment Questionnaire (MHAQ) up to 12 months (14), others found improvements in both MHAQ for patients with RA (21) and Bath Ankylosing Functional Index (BASFI) for patients with AS up to 28 weeks post-intervention (13). A third study on the effect of a 3-week rehabilitation programme for patients with ankylosing spondylitis pointed out that, despite significant improvement in disease activity (measured with Bath Ankylosing Disease Activity Index (BASDAI)), no improvement in physical function (BASFI) could be found (24). No improvement was explained by other components influencing patients’ physical function, such as environmental and personal factors, and that a relatively large reduction in symptoms is needed to improve self-reported physical function (24).
Coping and self-management
The EC-17 questionnaire was developed originally to assess self-management interventions and to measure of patient’s skills and attributes as effective consumers who manage their healthcare (25). In the current study, no significant changes were found in EC-17, either within the IG or between the IG and CG at any of the follow-up points. Studies that have shown an effect on the EC-17 are primarily studies of self-management programmes focusing on behavioural and self-management techniques (25, 26). The patient education component of the rehabilitation in this study consisted of group sessions covering how to cope with pain and everyday stress, and the methodology involved lectures, discussions and reflections. This methodology may not be sufficient to change patients’ behaviours or skills. A Cochrane Review published several years ago concluded that only patient education programmes with behavioural treatment components had some effect for patients with RA, and programmes characterized as only giving information had no effect (27). The recent recommendations of the European League Against Rheumatism (EULAR) for patient education for people with IA also states that behavioural, cognitive and emotional aspects are themes that need to be worked on thoroughly in patient education (11). However, there may be other reasons for why there was no effect on coping, as measured by the EC17. The EC17 was chosen because it was part of the national core outcome set in rehabilitation (16), but other outcomes, such as self-efficacy or patient activation, could have been relevant. Self-efficacy in patients with IA reflects patients’ beliefs in their abilities to manage relevant disease symptoms (28), while patient activation is about stages of patients’ readiness or confidence to make use of new health behaviours or strategies (29). Other studies on patient education in adults with IA have shown effects on both self-efficacy and patient activation (30, 31). It is also possible that there are important aspects that have not been captured in our study (31). The results do, however, indicate a need for reviewing and evaluating the patient education component of the intervention. It is possible that increasing the focus on self-management and including elements of cognitive behavioural treatment in the patient education part of this intervention could have increased the likelihood of improving this outcome (11).
Rehabilitation for patients with rheumatic disease often address and require major lifestyle changes of the participant in order to maintain the beneficial effect of the treatment over time (34). This illustrates, as others have pointed out, that some form of follow-up intervention could be necessary to maintain or develop processes that were initiated during the rehabilitation stay, both in terms of coping and self-reported physical function (24, 34). The research in this area is, however, limited and there is no consensus on what these follow-up interventions should consist of (33–35).
Strengths and limitations
The main strength of this study is that it is the first to evaluate an intensive rehabilitation programme developed specifically for young adults with IA. Moreover, the study has a strong methodology and long-term follow-up. However, the current study has some limitations. Sample size calculations are recommended prior to conducting a randomized controlled trial to ensure adequate power (36). This was not done, as the number of included patients was restricted, and thus predefined, based on available funding.
Lack of blinding of all involved in the study was not possible due to the type of intervention. It would have strengthened the study if the nurse in charge of the data collection was blinded (assessor blinding). This was, however, not feasible, due to practical issues, as the same nurse was in charge of the data collection and stayed at the rehabilitation centre together with the patients to oversee the intervention. The 30sSTS test is, however, an objective standardized test, and the study nurse was given detailed instructions on how to perform the test, and exactly what she should say and do. The lack of blinding should, therefore, in theory not affect the results greatly, yet it is possible that the study nurse either consciously or unconsciously treated the patients from the 2 groups differently, which somehow impacted the results (37). All other outcome measures beside the 30sSTS were self-reported. The outcomes were validated measures and the study nurse could not influence the outcomes, hence decreasing the risk of the results being affected by observer bias in a substantial way.
The intervention in this study, an intensive rehabilitation programme in a warm climate, is a highly complex intervention with multiple interacting components. This makes it difficult to distinguish which elements of the intervention are effective, and what can be explained by other factors, e.g. personality of the therapists, surroundings, social support, etc. It can therefore be questioned whether similar results would be found if the same intervention had been carried out in a different setting, in different climate and with different therapists. It would also be difficult for others to replicate the intervention, which limits the external validity of the results (38).
Conclusion
This is the first randomized controlled trial to evaluate the long-term effect of a 17-day rehabilitation programme for young adults with IA, including intensive individualized exercise and a patient education programme, carried out in a warm climate. The rehabilitation programme improved physical capacity in terms of improved lower extremity strength and power, at least 1 year after rehabilitation, but it did not have any effect on coping. Increasing focus on self-management skills, including elements of cognitive behavioural treatment in the patient education component of the rehabilitation programme, may increase the likelihood of improving patients’ coping.
The authors would like to thank the patients for participating in this study. We would also like to thank Hilde Bjørngaard, our study nurse, for her contribution.
Funding. This project was funded by the Norwegian Rheumatism Association, ”Revmafondet in Trondheim”, Central Norway Regional Health Authority research grant and St Olavs Hospital, Trondheim University Hospital. The funders had no involvement in study design, data collection, data analysis, manuscript preparation and/or publication decisions.


 Click to show fullsize
Click to show fullsize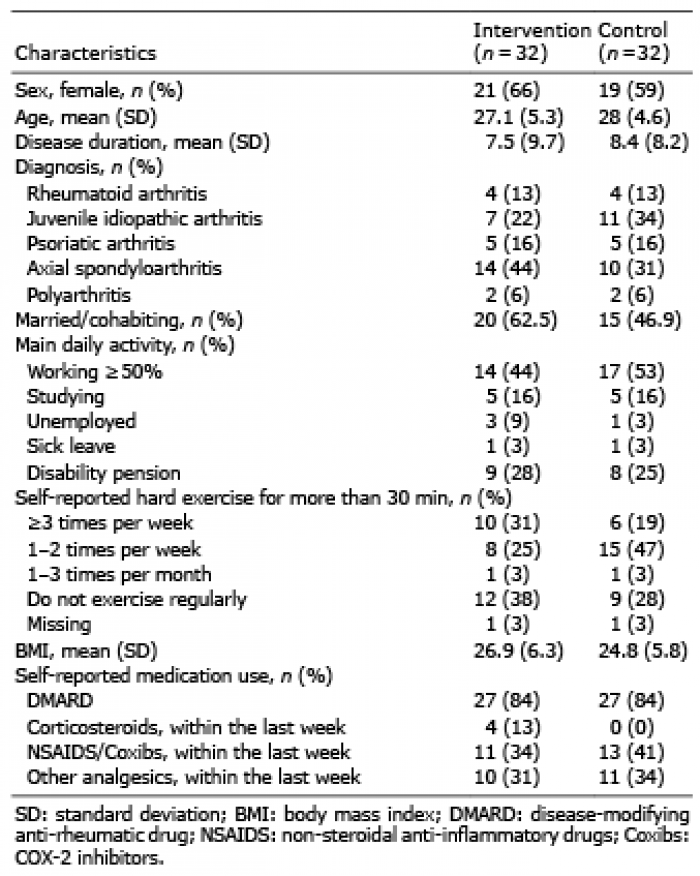 Click to show fullsize
Click to show fullsize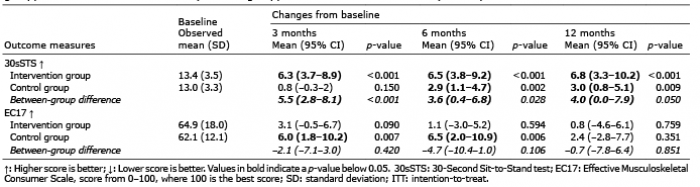 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize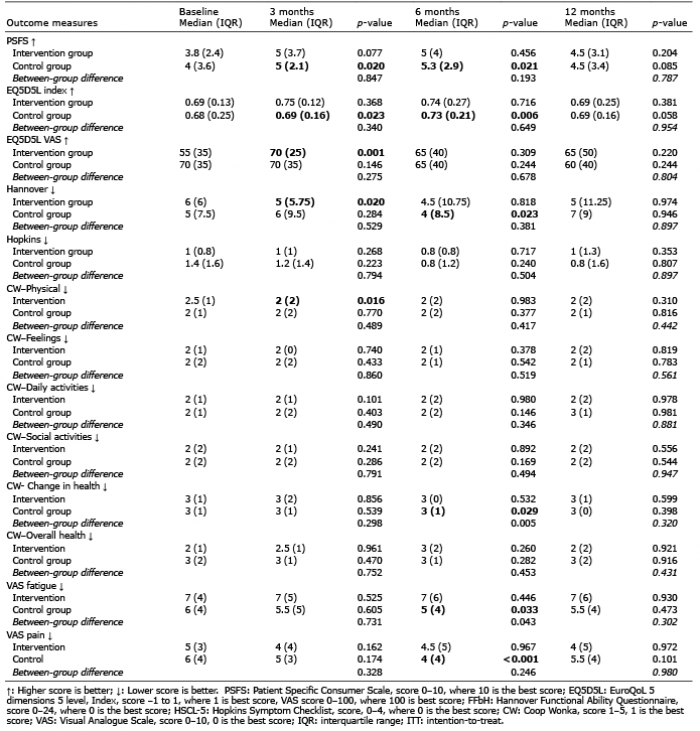 Click to show fullsize
Click to show fullsize