
From the 1Institute of Sports Medicine, Peking University Third Hospital, Beijing, China and 2Department of Sports Science and Physical Education, The Chinese University of Hong Kong, Hong Kong, China
*These authors contributed equally to this work.
Objective: To examine the effects of combining whey protein isolate supplement with preoperative isokinetic eccentric training on quadriceps mass and strength following anterior cruciate ligament rupture.
Design: Randomized controlled trial.
Subjects: A total of 37 male subjects with anterior cruciate ligament rupture.
Methods: Participants were randomly assigned to an isokinetic eccentric training group (n = 19) or an isokinetic eccentric training + whey protein isolate group (n = 18). Both groups received isokinetic eccentric training for 6 weeks. The isokinetic eccentric training + whey protein isolate group received 22 g whey protein isolate daily.
Results: After the intervention, the cross-sectional area of the affected quadriceps had increased only in the isokinetic eccentric training + whey protein isolate group (7.6 ± 6.8%; p = 0.012), whereas there was no change in the isokinetic eccentric training group (3.7 ± 4.5%; p = 0.11). Both groups showed increased quadriceps strength; however, there were no further effects for the isokinetic eccentric training + whey protein isolate group. Lysholm and IKDC 2000 knee function scores increased only in the isokinetic eccentric training + whey protein isolate group (p < 0.01).
Conclusion: Although the study showed numerically better outcomes for the combination of whey protein isolate supplement with isokinetic eccentric training compared with isokinetic eccentric training alone, no statistically significant differences were demonstrated between the groups.
Key words: eccentric training; whey protein; anterior cruciate ligament; quadriceps muscle.
Accepted Feb 26, 2020; Epub ahead of print Mar 10, 2020
J Rehabil Med 2020; 52: jrm00035
Correspondence address: Cuiqing Chang, Institute of Sports Medicine, Peking University Third Hospital, 49 North Garden Road, Haidian District, Beijing 100191, P. R. China. E-mail: changcuiqing@126.com
Following anterior cruciate ligament rupture, the mass and strength of the thigh muscle on the affected side is much lower than that of the unaffected side. This study aimed to examine the effects of combining whey protein isolate supplement with preoperative isokinetic eccentric training on the thigh muscle mass and strength following anterior cruciate ligament rupture. Subjects with anterior cruciate ligament rupture were assigned to an isokinetic eccentric training group or isokinetic eccentric training + whey protein isolate group. Both groups received isokinetic eccentric training for 6 weeks. The isokinetic eccentric training + whey protein isolate group received 22 g whey protein isolate daily. Although the study showed numerically better outcomes for the combination of whey protein isolate supplement with isokinetic eccentric training compared with isokinetic eccentric training alone, no statistically significant differences were found between the groups.
The anterior cruciate ligament (ACL) is an important structure that maintains the stability of the knee. Following ACL rupture, the strength of the quadriceps on the affected side can be 35% lower than that on the unaffected side, due to knee instability and quadriceps inactivity (1). The standard treatment for ACL rupture is ACL reconstruction (ACLR). Despite postoperative rehabilitation, the quadriceps muscle mass and strength nevertheless decreases by 10–20% because of postoperative immobilization following ACLR (2, 3). Preoperative strength of the quadriceps has been associated with postoperative muscle strength (4). Preventing asymmetry of >20% is beneficial for recovery of function after ACLR (5, 6). In addition, the loss of strength in the quadriceps is approximately 3 times greater than that of the hamstrings, resulting in an imbalance in flexor and extensor forces (1). An abnormal gait is common after ACL rupture and can continue postoperatively, causing degeneration of the knee cartilage, which increases the incidence risk of sports injuries and osteoarthritis of the knee (7).
Currently, the rehabilitation treatment worldwide focuses primarily on concentric training (CT) during the postoperative period. Studies have demonstrated that eccentric training (ET) results in a greater, more durable, improvement in muscle strength and volume compared with that achieved by CT (8–10). In recent years, ET has also been used for rehabilitation after ACLR. ET results in a significant increase in quadriceps strength, volume, and cross-sectional area (CSA) 6 weeks postoperatively, with an even greater increase observed 12 weeks postoperatively, which is a far greater effect than that achieved by CT (2, 11). The guidelines for rehabilitation following ACLR also suggest that a greater increase in muscle strength can be achieved by ET rather than CT (12). After 3 weeks of early rehabilitation following ACLR, moderate-intensity ET can be performed safely as part of the postoperative rehabilitation (13).
Despite the commencement of early rehabilitation 3 weeks postoperatively, the quadriceps muscle mass is already 25% lower than that on the unaffected side. This suggests that discussion of preoperative ET is necessary in order to address this clinical problem. Few studies currently evaluate the effect and safety of preoperative ET.
A number of studies have shown that the combination of whey protein (WP) and strength training significantly increases lean body mass and muscle mass (14, 15). WP isolate (WPI) is considered to be the most effective protein for stimulating muscle protein synthesis, both at rest and after resistance exercise (16). However, to our knowledge, no study evaluating the administration of WPI in the rehabilitation of patients with ACL rupture has been conducted.
Therefore, the aim of this study was to evaluate the effect of combining WPI with preoperative isokinetic ET (IET) on the mass and strength of the quadriceps and knee function following ACL rupture. Our hypothesis was that significant increases in quadriceps mass and strength and improvement in knee function would be achieved regardless of whether WPI was administered. This effect would be even greater with the administration of WPI.
Subjects
A total of 69 male participants, aged 18–40 years, with ACL rupture were recruited using a poster in the outpatient division of the hospital.
The inclusion criteria were: unilateral ACL rupture; male; 18–40 years of age; non-acute stage of injury; inconspicuous joint inflammation; no obvious limited range of motion (ROM) of the knee; and quadriceps atrophy, indicated by a difference of ≥1 cm in thigh circumference. The exclusion criteria were: ACL rupture combined with other injuries; inflammation and limited ROM of the knee; composite ligament relaxation of II–III degrees; bilateral knee injury; severe limb or lower back injury, such as nerve injury, fractures, and lumbar disc herniation; concurrent repairable meniscal injury on magnetic resonance imaging (MRI); articular cartilage injury; milk protein allergy; diseases that are unsuitable for exercise; and body mass index (BMI) >28 kg/m2. Based on these criteria, 37 eligible participants were enrolled in the study.
Participants were excluded if they chose to withdraw from the study, if knee fluid leakage increased, pain increased, ROM of the knee was limited for more than 3 days, or any other adverse event occurred. Data would be excluded if participants trained fewer than 8 times or did not train for 2 consecutive training sessions.
This study was approved by the Medical Ethics Committee of Peking University Third Hospital (No. [2013]070 (2)) and was registered at the China Clinical Trial Registration Center (Registration no. ChiCTR1800015967). All participants were informed of the purpose and risks of the study and provided written informed consent.
Interventions
The study was a randomized controlled clinical trial. Using a block randomization method with a block size of 4, every 4 sealed envelopes, containing 2 envelopes in each treatment, were placed in a separate pile and shuffled thoroughly. The random allocation sequence was provided by an epidemiologist supported by the university. Enrollment and assignment of participants were performed by 2 independent researchers, respectively. A total of 37 participants were randomly assigned to 2 groups, with 19 in the IET group and 18 in the IET with WPI supplement (IET+WPI) group.
Blinding of patients and the principle investigator to treatment allocation was not possible because of the nature of the intervention. Nevertheless, the data analyst was blinded to the treatment allocation because data were analysed using coded identification numbers. Physiotherapists were also blinded to the treatment allocation while performing the IET.
IET group. Patients underwent IET of the affected quadriceps in the range of 30–90° at 60°/s twice a week for 6 weeks using the Isokinetic Biomechanical Testing and Training System (CON-TREX MJ, Physiomed Elektromedizin, Schnaittach, Germany). Each session contained 4 sets with 8–10 repetitions per set and 2 min of rest between each set. The resistance was progressively increased from 50–70% of the peak torque (PT) to 70–90% of the PT in the first 2 weeks, while being maintained at 100% of the PT in weeks 3–6.
IET+WPI group. In addition to performing the IET, participants were supplied with 22 g WPI per day (99% of protein content, BiPRO ™, Davisco, Le Sueur, MN, USA) for 6 weeks. WPI was consumed within 30 min of the training, on training days, and with breakfast, on non-training days.
All subjects initiated the training at least 1 month after ACL rupture, ranging from 1 to 60 months (mean 12.9 months; standard deviation (SD) 18.9 months).
Outcome measurement
The CSA of the quadriceps was measured on MRI. Bilateral thigh MRI scans were performed on a commercial 3T MAGNETOM Trio, A Tim System (Siemens Medical Solutions, Erlangen, Germany) using an axial view with a 3-mm section thickness, 0.6-mm layer spacing, a 3-dimensional T1 VIBE fat-saturated sequence, phase code A >>P, field of view 400 × 275.2 mm, repetition time 11.3 ms, and echo time 4.79 ms. Repeat scans were performed if motion artefacts occurred. The CSA of the quadriceps was analysed at 15 cm above the upper patella using syngo MR software (Siemens, Erlangen, Germany). This was performed by the same person, and the same plane was measured repeatedly 3 times.
The eccentric strength (ES) of the quadriceps at 60°/s and concentric strength (CS) at 60, 180 and 300°/s were measured using the Isokinetic Biomechanical Testing and Training System (CON-TREX MJ, Physiomed Elektromedizin, Schnaittach, Germany). The range of motion was 20–90° during the testing. The training thigh was fixed using a strap and the unaffected knee was secured in flexion. After eliminating the self-gravity compensation, a single set was attempted prior to each mode test to ensure the correct direction of the force. Subjects were asked to use the leg to perform the test, while relaxing the body and upper limbs to avoid compensation.
Knee function was measured using the Lysholm knee score and IKDC 2000 knee score questionnaires. The maximum score was 100 points. Knee laxity was evaluated by comparing the distance of anterior translocation of tibia on the 2 sides. It was measured using the KT-2000 Knee Stability System (Kneelax3, Monitored Rehab Systems, Haarlem, Netherlands). Patients were placed in a supine position with the quadriceps completely relaxed and the knee at 30° of flexion. The distance was measured under a 30-pound tension.
Bilateral knee circumferences were measured 3 times using a tape. Participants were asked to stand upright, with their arms in a natural position at their sides. The mean value was recorded. Body composition, including weight, body fat, muscle mass and fat-free mass (FFM), was measured using BIA (Tanita MC-180 MA, Tokyo, Japan). Pain intensity of the knee was evaluated using a visual analogue scale (VAS) for pain (0–10).
Physical activity level was recorded weekly using the International Physical Activity Questionnaire (IPAQ). The 3-day diet was recorded before and after the intervention. Mean daily calorie intake and protein intake were calculated by a dietitian according to the Chinese Food Composition Tables (17).
Statistical analysis
Based on a previous study (18), which reported that a combination of whey protein intake and rehabilitation significantly increased knee extension strength during the early postoperative period in patients with hip fracture, we estimated that 25 subjects would be needed in each group to achieve 80% power to detect the smallest expected effect size (Cohen’s d = 0.818) in knee extension strength between the interventions (2-sided, 5% level).
SPSS 22.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Continuous outcomes are described as the mean (SD). Percentage changes between pre- and post-intervention for each subject were calculated for descriptive purposes. Analysis of covariance (ANCOVA), with pre-intervention values as a covariate, was used for the comparison between groups. Paired t-tests were used for comparison before and after the intervention within each group. The level of significant difference was p < 0.05. All graphs were generated in GraphPad Prism (Version 8.0, San Diego, CA, USA).
Characteristics of subjects
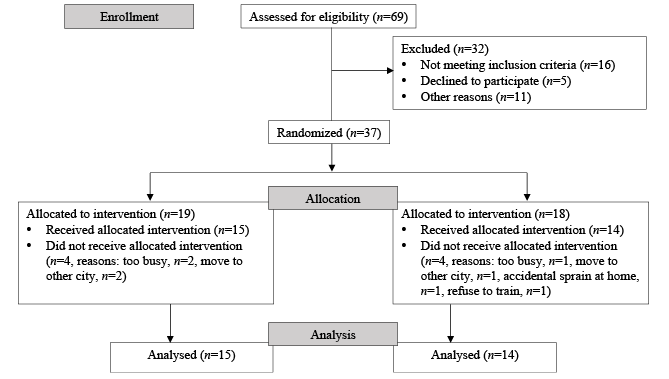
A total of 37 participants were enrolled in this study; 19 in the IET group and 18 in the IET+WPI group. During the intervention period, 8 participants (4 in each group) withdrew for personal reasons. Finally, 15 participants in the IET group and 14 participants in the IET+WPI group completed the intervention and were included in the analysis (Fig. 1). Some participants declined to undergo MRI as it was too time-consuming. Thus, only 6 participants in the IET group and 10 in the IET+WPI group completed both the pre- and post-test of MRI. All other outcomes, including isokinetic strength, Lysholm score, IKDC 2000 score, knee laxity, knee circumference, body composition, and VAS score for pain were assessed in all participants. There was no significant difference in baseline characteristics of participants between the 2 groups (Table I).
Fig. 1. Flow chart depicting the sampling and distribution of subjects.
Table I. Characteristics of participants
Changes in quadriceps cross-sectional area
The mean CSA of the quadriceps increased by 3.7% (SD 4.5) (p = 0.11) and 7.6% (SD 6.8) (p = 0.012) after the intervention in the IET and IET+WPI groups, respectively. However, the difference between the groups was not statistically significant (F = 1.647, p = 0.22). The mean ratio of the 2 sides increased by 3.9% (SD 3.7) (p = 0.050) and 4.8% (SD 3.4) (p = 0.002) in the IET and IET+WPI groups, respectively, with no difference observed between the groups (F = 0.015, p = 0.91). There was a mean increase in the CSA of the rectus femoris (14.1%), while the CSA was unchanged in the other 3 muscles in the IET group. In the IET+WPI group, the CSA of the rectus femoris, vastus lateralis, and vastus internus increased significantly by 12.0%, 8.6% and 9.6%, respectively (Fig. 2). Individual changes of CSA were shown in Fig. 3.
Fig. 2. Changes in the cross-sectional area of: (a) quadriceps, (b) rectus femoris, (c) vastus medialis, (d) vastus lateralis, and (e) vastus internus, shown by the size on the affected side and unaffected side and the ratio between the 2 sizes. Compared with pre-intervention within the group, *p < 0.05, **p <0.01. IET: isokinetic eccentric training; IET+WPI: isokinetic eccentric training and whey protein isolate supplement. Presented as means ± standard errors.
Fig. 3. Individual changes in the cross-sectional area of: (a) quadriceps, (b) rectus femoris, (c) vastus medialis, (d) vastus lateralis, and (e) vastus internus, shown by the size on the affected side and unaffected side and the ratio between the 2 sizes (n = 6 in IET, n = 10 in IET+WPI). IET: isokinetic eccentric training; IET+WPI: isokinetic eccentric training and whey protein isolate supplement; A: affected; U: unaffected; A/U: affected/unaffected.
Changes in quadriceps strength
After the 6-week intervention, the ES (at 60°/s) and CS (at 60°/s, 180°/s, and 300°/s) of the quadriceps increased by 27.9% (p < 0.001), 35.9% (p < 0.001), 34.3% (p = 0.002), and 24.1% (p = 0.007) in the IET group, respectively, and by 44.2% (p < 0.001), 42.3% (p < 0.001), 37.4% (p = 0.002), and 31.5% (p = 0.002) in the IET+WPI group, respectively. Although the IET+WPI group obtained a greater increase, there was no significant difference between the groups. The strength gap between the 2 sides was reduced (Table II).
Table II. Changes in peak torque of the quadriceps during eccentric and concentric contraction, and knee function scores (presented as mean (95% confidence interval; 95% CI))
Knee function and laxity
There was a numerical increase in the Lysholm score and IKDC 2000 score in both groups, whereas only the increase in the IET+WPI group reached statistical significance (p < 0.01) (Table II). There was no change in the laxity of the knee in both groups (p > 0.05).
Visual analogue scale and knee circumference, fat-free mass, physical activity, and dietary intake
The VAS for pain score, circumference of the knee, and FFM did not change in both groups (p > 0.05). There was no significant difference in physical activity (excluding training volume) between the groups before and after the intervention (p > 0.05).
The 3-day diet data showed that there was no difference in dietary protein intake between groups before and after the intervention (Table III). However, after taking the 22 g/day whey protein supplement into account, the mean total protein intake remained similar after the intervention between the 2 groups (IET vs IET+WPI, 1.1 g/kg/day (SD 0.4) vs 1.1 g/kg/day (SD 0.2)).
Table III. Three-day diet recording
A similar increase in quadriceps strength was found with ET alone and when combined with WPI supplementation, and an increase in quadriceps CSA and an improvement in knee function was found only when ET was combined with WPI supplementation. However, although better outcomes were found when IET was combined with WPI supplementation, these between-group differences were not statistically significant.
ET has been used after ACLR and is considered the most effective way of maintaining the quadriceps muscle strength (19, 20). Compared with CT (9, 21), ET may have produced larger effects in our study, because, in comparison with CC, EC results in greater muscle strength (22), induces greater nerve stimulation (10), and recruits more type II muscle fibres (2), while producing a lower rate of oxygen consumption and metabolic requirements (23). Preoperative training may be easier to perform and may produce a greater effect. Few studies have investigated preoperative training in patients with ACL rupture, and those that have used CT (21, 24). Despite the severe loss of muscle mass and strength observed in patients, there is hesitation in performing ET after ACL rupture. The current study demonstrates the safety and efficacy of preoperative ET. Nevertheless, it would be more robust to add a control group.
Resistance training (RT) in combination with protein supplementation is a common practice, used to enhance RT-induced gains in muscle mass and strength (25). Although conflicting results have been reported in previous studies (15, 26, 27), the 2 largest and most comprehensive meta-analyses (28, 29) have recently demonstrated relatively consistent findings, showing that protein supplementation augmented RT-induced increases in 1-repetition maximum strength and FFM. In this study, the comparably significant increase in muscle strength observed in both groups (27–44%) in this study is consistent with results of previous studies (28, 30), suggesting that ET is a more predominant stimulus, inducing a gain in strength, compared with the contribution of the additional protein supplementation. Protein supplementation plays a minor role, if any, in augmenting the RT-induced increase in strength. However, there was a 3.7% gain in the CSA of the quadriceps in the IET group and a 7.6% increase in the IET+WPI group, similar to the results of the previous study that evaluated CSA after 6 weeks (+4.1%) and 12 weeks (+8.9%) of ET following ACLR (11), suggesting that ET combined with WPI may result in a greater gain in muscle over a shorter period of time.
Most studies investigating the effect of RT in combination with protein supplementation focus on the effects in elderly and adult populations (28). The only study that investigated the effects of RT combined with protein supplement in patients with ACL rupture showed that 12 weeks of additional milk and soy protein intake augmented the increase in muscle mass and PT of the quadriceps following RT (24). However, in this study, no statistically significant between-group differences were observed after 6 weeks of ET with or without WPI supplementation.
There are several possible reasons for this discrepancy. First, the amount of daily protein intake and extra WPI provided to participants in this study may have been insufficient to induce the expected further benefits. Previous studies have shown that a daily protein intake of 1.6 g/kg/day had a greater effect on the adaptive changes produced by RT (28, 31). However, in this study, subjects from both groups did not consume enough dietary protein, with an even lower protein intake observed in the IET+WPI group (1.1–1.2 vs 0.8–1.1 g/kg/day). Moreover, only 22 g of daily WPI was provided to participants (equivalent to ~0.25 g/kg/day), which was lower than the optimal recommended amount (~35–40 g/kg/day) (28). The daily protein intake decreased in the IET+WPI group after the intervention, and the total daily protein intake including that contributed by the WPI supplement was comparable between the IET+WPI (1.1 g/kg/day (SD 0.2)) and IE groups (1.1 g/kg/day (SD 0.4)), both of which were insufficient. A reason for this may be that WPI ingestion suppresses appetite (32), or it may affect participants’ habitual dietary intake, such as milk intake.
However, albeit not significant, the greater increase observed in the IET+WPI group may suggest that WPI may be superior to other sources of mixed dietary protein (33, 34). WPI, known as “fast protein”, is rich in branched-chain amino acids, particularly leucine, which are easily absorbed. Leucine is a priming molecule in muscle synthesis, characterized by a dose-effect relationship (10–20 g) that promotes the synthesis of skeletal muscle protein through the mammalian target of rapamycin complex 1 (mTORC1) (15). Nevertheless, it was shown that the stimulation of muscle protein synthesis after WP ingestion might not be as sustained as that produced by milk protein (35).
Secondly, the 6-week intervention may not be sufficient time to observe the full effect of the intervention on muscle mass and strength (32). Previous studies investigating these effects after 8–12 weeks of training were more likely to report benefits (28, 29). Nevertheless, an extended preoperative training intervention may result in the optimal time for surgery being missed. In addition, the sample size may have been too small to identify the differences between groups.
The increase in muscle strength and mass of the quadriceps may have contributed to the improvement in lower-limb function. In our study, the ratio of the strength of the 2 sides increased (data not shown), suggesting an improvement in the symmetry of the quadriceps, which is beneficial to knee function (36).
No adverse events occurred during the trial, and the pain score was not affected. The results of the KT-2000 showed that the preoperative ET did not worsen knee laxity, suggesting that preoperative ET and WPI supplementation were safe and feasible.
To the best of our knowledge, this is the first randomized study that has applied IET and WPI supplementation preoperatively in patients with ACL rupture. Accordingly, it highlights preoperative rehabilitation and motivates for the initiation of IET and WPI supplementation. In addition, the effects of preoperative training may enhance the effects of postoperative rehabilitation and allow patients to return to sport activities much sooner. Supplementing with WPI can also be administered routinely to patients with ACL rupture to improve recovery and increase hypertrophy of the quadriceps.
This study has some limitations, including insufficient daily protein intake, relatively shorter duration of intervention, and small sample size. The daily dietary protein intake should be controlled to ensure that sufficient amounts are ingested in future studies. Postoperative follow-up is needed to observe the long-term effects of preoperative training and nutritional support on postoperative rehabilitation in patients with ACL rupture.
In conclusion, this study suggests that ET is an effective and safe preoperative intervention that can be implemented to increase the strength of the quadriceps in patients with ACL rupture. Although the additional ingestion of WP may augment the beneficial effects on the CSA of the quadriceps and knee function, no statistically significant differences were observed between the groups.
The authors acknowledge Stephen H. S. Wong for his guidance in thesis writing. The authors acknowledge the support received from the Clinical Epidemiology Research Center of Peking University Third Hospital. The authors also thank participants who volunteered and devoted their time to the study.
Funding. This research was funded by Key Technologies Research and Development Program (grant number: No.2016YFD0400603) and the Key Research Project of the State Sports General Administration (grant number No.2014B003).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize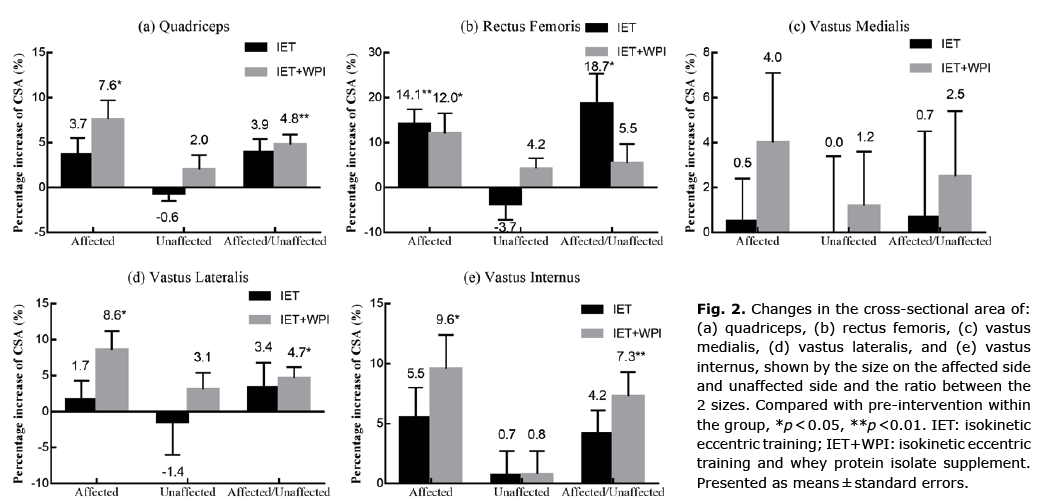 Click to show fullsize
Click to show fullsize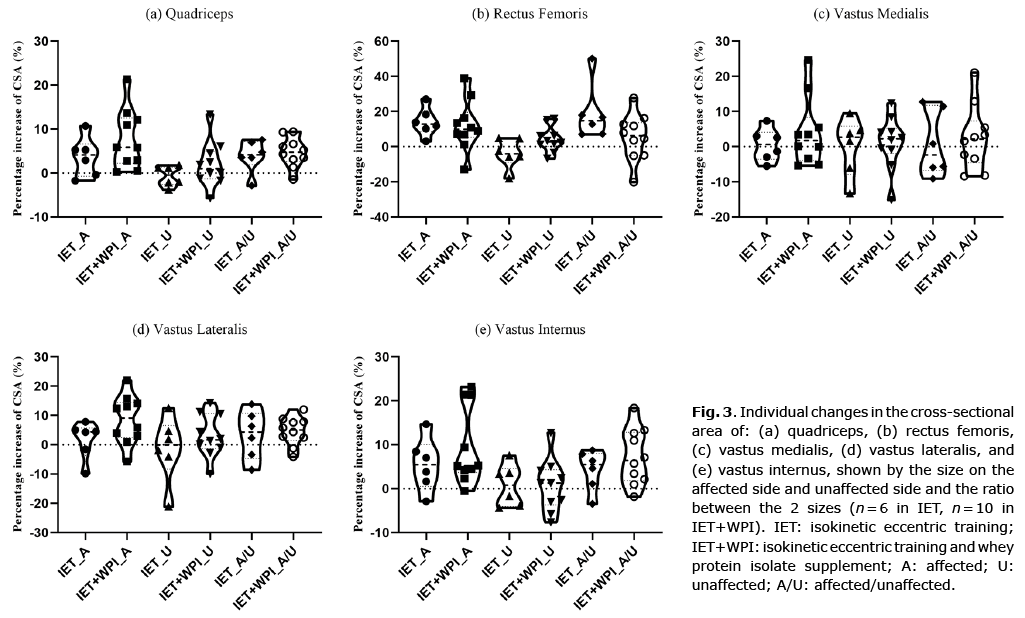 Click to show fullsize
Click to show fullsize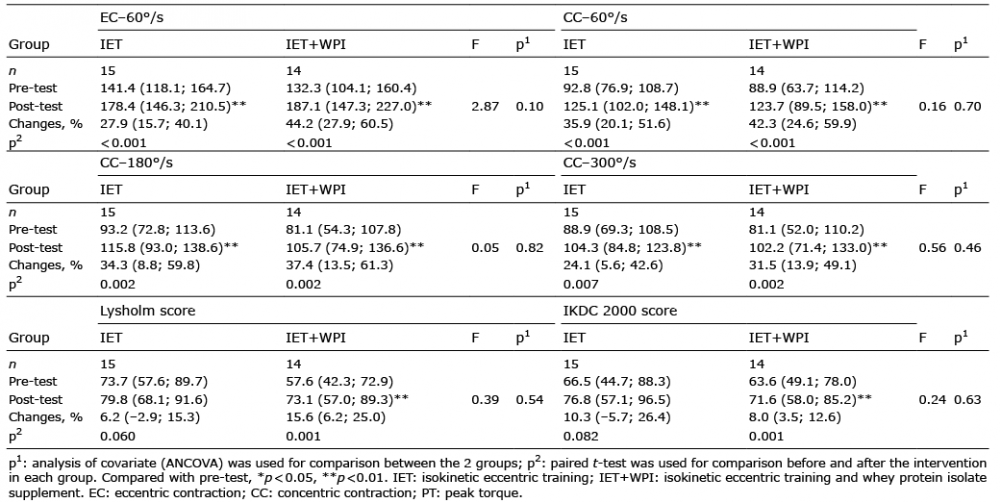 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize