
From the 1Health Sciences Research Centre, UCL University College, 2Department of Sports Science and Clinical Biomechanics, University of Southern Denmark, 3The Nordic Institute of Chiropractic and Clinical Biomechanics, Odense, and 4Private practice, University of Southern Denmark, Odense M, Denmark
Background: There is general agreement that non-specific low back pain is best understood within a biopsychosocial understanding of health. How-ever, clinicians and patients seemingly adhere to a biomedical model, which may introduce misperceptions of pain and does not inform treatment or prognosis.
Objective: To explore, from the perspective of health-care practitioners, how persistent non-
specific low back pain may be communicated in a way that moves beyond a biomedical diagnosis.
Design: An explorative qualitative investigation using a constructivist diagnostic framework.
Methods: Focus group and individual interviews of 10 purposefully selected chiropractors, physio-therapists and general practitioners were codified and thematically analysed.
Results: Four themes emerged: “Clinicians’ nuanced understanding of back pain”; “The challenges of shared decision-making”; “Cultural barriers to moving beyond biomedicine”; and “More than a label – individual explanations for pain”. Pain and disability were perceived as products of multiple bio-psycho-social factors. Clinicians identified the impact of multiple social actors, an unhealthy work culture, and the organization of the medical system on the notion of pain and suffering.
Conclusion: Clinicians perceived a need to communicate the complexity of non-specific low back pain in order to help patients make sense of their condition, rather than applying diagnostic labelling. There are multiple barriers to integrating a constructivistic diagnostic framework into clinical practice that need to be overcome.
Key words: low back pain; diagnosis; health communication; attitude of health personnel; culture, qualitative research.
Accepted Jan 29, 2020; Epub ahead of print Feb 25, 2020
J Rehabil Med 2020; 52: jrm00036
Correspondence address: Corrie Myburgh, Department of Sports Science and Clinical Biomechanics, University of Southern Denmark, Campusvej 55, 5230 Odense M, Denmark. E-mail: cmyburgh@health.sdu.dk
When presenting with persistent low back pain, more than 9 out of 10 patients cannot be given a structural cause of their symptoms. These individuals receive a diagnosis of non-specific low-back pain, which does little to inform them about the type of problem they have or how it might be remedied. This study used a social diagnosis framework, which considers multiple factors in relation to illness, to explore how physiotherapists, chiropractors and general practitioners might help us to identify a diagnosis (i.e. a label and the meaning we bring to it) alternative to non-specific low back pain. The aim being to enable better communication with patients about their condition. The study found that healthcare practitioners consider multiple biopsychosocial factors relevant to the condition, they consider it important to help patients make sense of their condition, and to engage patients in dealing with individual contributors to pain. Healthcare practitioners did not consider a new diagnostic label for non-specific low back pain to be a priority for their own practice.
It is generally acknowledged that persistent and recurrent low back pain (LBP) (1, 2) is inescapably connected not only to biological processes, but also to personal lived experiences, social context and cultural beliefs and practices relating to illness and health (2–4). In approximately 90% of people presenting with LBP, no specific structural cause of pain is identifiable (2, 5), resulting in the ubiquitous diagnosis of non-specific low back pain (NSLBP). However, this biomedically-derived diagnostic strategy fails to meaningfully inform either treatment or prognosis (6) and adds no value to patients’ understanding (7).
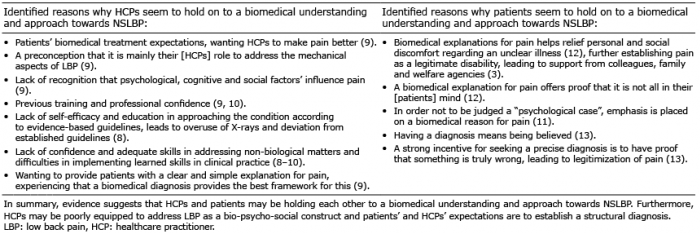
Notwithstanding the above, healthcare practitioners (HCPs) (8–10) and their patients (3, 11–13) still adhere to this traditional diagnostic approach (Table I), potentially leading to psychological harms of disease labelling (3, 11, 12, 14), overdiagnosis/medicalization (15, 16), and even iatrogenically induced chronicity (3, 8).
In an attempt to counter this ongoing problem, a constructivist approach, grounded in the co-creation of a shared narrative about LBP (3), has been suggested as an interesting alternative (4). Specifically, a social diagnosis (SD), as conceptualized by Brown et al. (17) offers an approach to diagnosis that moves beyond individual-level explanations; identifying an interplay between various actors, social structures, and societal illness beliefs and practices. In addition, this framework offers a broader understanding of extra-medical and macro-structural factors in illness (17). The key lessons of a SD framework are presented in Table II.
Table I. Identified reasons why patients and healthcare practitioners seem to hold on to a biomedical understanding and approach towards non-specific low back pain (NSLBP)
Table II. Key lessons of a social diagnosis (SD) framework (17)
With respect to persistent and recurrent NSLBP, the SD framework provides a way to articulate the complexity of elements affecting the condition. This is accomplished through the construction of a shared narrative, which may legitimize non-biomedical elements of pain, possibly providing HCPs and patients with a sense of coherence (16). Rather than viewing diagnosis as a medical tool, it could be seen as socially constructed, relational and changeable (17); a co-construction that serves to create how we interpret and understand illness and health.
This study was conducted within the context of the GLA:D® Back programme; a patient education and exercise self-management programme for patients with persistent NSLBP (18). In a bid to move away from language that entrenches biomedical explanatory frameworks, a need was identified for an alternative diagnostic label to NSLBP, in order to better communicate with patients about their back pain. However, a label would not be useful unless it carries a meaning that is helpful for understanding back pain.
The aim of this study was therefore to explore HCPs’ perspectives on diagnosing recurrent and persistent NSLBP in a way that might assist communication that moves beyond a biomedical diagnosis.
Study design
An exploratory, qualitative investigation was devised, grounded in a constructivist approach using a SD framework to explore communication around diagnosis, by gaining insight into the thoughts, experiences and actions of HCPs (17, 19).
Sampling strategy
A purposeful sampling strategy was used to solicit responses from physiotherapists, chiropractors and general practitioners (GPs) (20). Physiotherapists and chiropractors involved in the GLA:D® Back pilot project (21) were judged to possess extensive knowledge on the area of LBP and were all invited by e-mail to participate. Moreover, GPs with an interest in LBP were accessed through snowballing (22) the professional network of the first author (RL). Having respondents from these 3 professions was considered to provide rich and balanced perspectives on diagnosing persistent and recurrent NSLBP (23)). Based on the study design, and RL’s experience as a moderator, a sample size of 8 participants (n = 8, in 2 focus groups) was deemed appropriate (19).
Participants
The initial e-mail campaign resulted in responses from only 5 potential respondents. However, telephone invitations resulted in the inclusion of physiotherapists and chiropractors from 3 clinics. Due to interpersonal-power considerations (19), an additional respondent was prioritized in focus group 2, resulting in a 3- and 5-respondent split in the 2 focus groups; Focus group 1 (FG1) enclosing two chiropractors and one physiotherapist, focus group 2 (FG2) enclosing two chiropractors and three physiotherapists (see Table III).
Table III. Characteristics of included healthcare practitioners (HCP) and distribution across interviews
Data collection
Semi-structured focus group interviews were used, as they allowed for multiple perspectives to be elicited and interesting perspectives to develop during discussion (19). However, the GP respondents were unable to participate in the focus group interviews, thus individual interviews were used as a complementary method to further enrich the data (19).
Interviews were conducted by RL, a physiotherapist, working actively with patients with LBP, who is educated in the area of cognitive behavioural therapy (CBT).
To facilitate dialogue, an infogram was used as a vignette to introduce the case of interest prior to interviews (19). The SD framework was used to inform the development of a semi-structured interview guide (Table IV), using open-ended questions that would address the study aim (19). The respondents were not introduced to the SD framework, but were informed that the project was part of the GLA:D Back initiative, and that they could help develop a diagnosis alternative to NSLBP, in order to better communicate with patients about their back pain and back-related problems. As a moderator, RL strived to provide a supportive atmosphere, engaging equally with participants, allowing for personal, multiple and conflicting viewpoints to be elicited (19). Interviews were audio-recorded and notes were taken after the interviews for reflective purposes (19). All interviews were transcribed verbatim (24).
The interviews were conducted at private physiotherapy, chiropractic and GPs’ clinics in Denmark. The characteristics of the respondents and their distribution across interviews are shown in Table III.
Table IV. Semi-structured interview guide based on a social diagnosis (SD) framework
Ethical considerations
Prior to participation HCPs signed an informed consent form describing the purpose of the study and the interview, informing HCPs of data anonymization, data recording and the possibility of withdrawing consent at any time. Data were collected and stored according to the Danish Data Protection Agency stipulations (25, 26). No approval was required from the Science Ethics committee (27).
Data analysis
Data were analysed using an abductive, 6-phase flexible thematic analysis approach, as described by Braun & Clark (19). Deductive codes were derived from the key lessons of a SD framework to identify patterns relating to diagnosing NSLBP in a way that may assist communication beyond a biomedical diagnosis. As the key lessons of a SD framework are dynamic and open to interpretation (17) inductive codes were derived from meaningful units of text occurring naturally within the transcripts and identified during line-by-line coding (19). Thematic analysis was aided through the use of the NVivo 11 software package (QSR International Pty Ltd, Australia. (https://www.qsrinternational.com/nvivo/contact-us/contact-form)).
The process of coding was flexible and organic, with sections of interest to the aim extracted and given a code and code definition. Existing codes were changed if their content was expanded or contracted, splitting and collapsing codes as analysis evolved. As primary investigator, RL was closest to the data and therefore created the initial code list (28, 29), whereas CM acted as code checker. After receiving the list of codes and definitions, CM critically evaluated these for rigour and consistency against the original text, recommended changes and encouraged reflection and exploration of alternative explanations and interpretations of codes within the data. EB was also presented with the interpretations and encouraged alternative interpretation (19).
Codes were subsequently organized into higher-level patterns relating to diagnosing NSLBP in a way that might assist communication beyond a biomedical diagnosis. Emerging themes were discussed with CM, who encouraged reflection and explorations of alternative theme-names, in order for themes to optimally reflect data content. Themes, code names, and code definitions are shown in Table V.
Table V. Identified themes, codes, code- and theme definitions
The analysis resulted in 4 themes relating to diagnosing NSLBP in a way that may assist communication beyond a biomedical diagnosis, namely: “Clinicians’ nuanced understanding of back pain”; “The challenges of shared decision-making”; “Cultural barriers to moving beyond biomedicine’’; and “More than a label – individual explanations for pain”.
Theme 1: Clinicians’ nuanced understanding of back pain
In general, pain and the demands of life were seen as inextricably connected. Factors such as physical and mental stress, depression and anxiety, former trauma, pain acceptance, quality of sleep, muscular dysfunctions, inactivity and overweight, were all issues mentioned as associated with the condition. According to respondent C it is:
... their ability to cope with the pain, … with the path they are on. The length of it. The demands over time that their life is congested with both in terms of pain, in terms of work, and in terms of feeling good enough…”
Different explanatory models were utilized to operationalize this complexity, including the “onion model”, illustrating how pain and psychosocial loads invariably affect one another:
… it is the onion, right. The pain is in the middle… then there are all the psychosocial layers on top… in the end these things actually take up more space than the pain … they may initially be a result of the pain but may also be one of the reasons for pain onset… (I).
and the “extended biomechanical model”, describing how psychological and social factors can positively or negatively reinforce biomechanical pain:
… they kind of get the biomechanical model…then you can take all the other things too, and explain to them, that they also contribute. They affect how your body feels both negatively and positively (E).
Fear featured strongly as a factor that required elucidation and understanding, as fear was thought to directly affect pain and disability. Fear of getting fired, not being able to continue working and provide for the family (I, A, C), fear of movement (H, F) and the concerns/fears of relatives (J) were all reported as affecting pain and disability. Fearing “dangerous” reasons for pain and whether something was being overlooked also emerged as an important feature. In reflecting on this issue, respondent I stated:
One day she came to me and asked if it would be possible to do a scan. Can’t we do something? Because she was a little afraid of it, but her husband was really scared of what it was…
Anxiety was simultaneously seen as a consequence and an amplifier of the pain state:
… when she was very anxious, she also had more back pain (I).
A variety of work-related issues were mentioned as affecting the condition. In general, an inflexible and unbalanced work culture within society was reported as affecting the condition; demanding jobs and workload leading to stress on body and mind. This issue was illustrated as follows:
… very happy in their jobs, but actually… also a bit overloaded (I).
… we just have a culture that we have to be deadly ill lying in bed before we don’t show up (E).
One respondent noted that without work patients felt like
…a burden to our loved ones and to society, but … no one articulates this when we are speaking about the back (A).
Having access to the social benefit system was reported as sometimes paradoxically problematic. For example, when the social benefit system funnels people into job training that is too difficult or stressful;
…some are so stressed that they actually become more ill (I).
Theme 2: The challenges of shared decision-making
Respondents emphasized the importance of exploring what patients perceive as the most important problem and investigating their goal in terms of seeking treatment, rather than diagnosing elements of suffering that might not seem problematic or important to the patient. This point is illustrated as follows:
… back in the day you had a diagnosis and then you could say – it is this!…but first and foremost, I am actually very fascinated by the thought that it needs to make sense to the patient… (C).
And:
…What would you like…where would you like to end up with this? (C)
It was noted that patients presenting in consultations possessed knowledge of potential reasons for pain, however this was not always considered valid knowledge, rather an expression that patients take responsibility. Moreover, it was observed that a shared understanding did not always imply an understanding reached through dialogue and mutual agreement. This is illustrated by F, who stated in relation to a patient:
… you have pain from your back and whether it is exactly from cartilage or ligaments or muscles… it doesn’t matter that much to me and neither does it to you. We need to figure out how to get it to go away or how you can deal with it’. (F)
Under a perceived imperative that a well-formulated explanation is the tacit patient expectation, I noted:
… if I was to ask them what do you think is wrong?, then they would think ‘can’t you figure that out … that’s why I am here’… (I)
Respondents broadly engaged in interprofessional dialogue, seeking second opinions or communicating to each other what was wrong with the patient (I, J, A, B, C, D, H). These interactions were viewed as important, forming a shared understanding and collaboration regarding what is wrong with the patient, so that patients could perceive a sense of coherence within the medical system. However, this was not always reported as what occurs, as A reported:
… [when] it is [a case] more appropriately placed [with] a psychiatrist or psychologist, then I can write a discharge summary and hope for the best…(A).
In addition, A argued that differing explanations for pain are a source of patient frustration:
… how have they been told, and how many things have they been told, it really takes up a lot of space in their consciousness… (A)
As a group, the respondents expressed an enormous potential in having an extended interdisciplinary communication within the Danish medical system, so that diagnosing and treating NSLBP becomes an act of dialogue rather than a fragmented experience with different explanations and recommendations, which leaves patients frustrated;
…we must be better at communicating across [health] sectors and professions (A).
Lack of interprofessional knowledge (J), work pressure, work-related traditions (D) and patient permission (I), were reported as reasons for interdisciplinary communication sometimes lacking.
Theme 3: Cultural barriers to moving beyond biomedicine
Respondents argued that the continued use of biomedical explanations for pain is problematic.
…it makes patients continue to search for a reason and not accept that pain is there (J).
Despite this view and the nuanced understanding expressed, issues of time and the parameters of the current practice limit consideration of non-biomedical aspects of LBP conditions. Illustrative of this issue is an observation from focus group 2:
… I sometimes book a complicated patient … as the last patient, … so I have the possibility to stay a bit longer without feeling pressured (D).
Paradoxical to their nuanced understanding of the problem, some respondents appear to apply a limited biomechanical understanding to the problem when patients present with a new episode of pain. The rationale being that, in practice, there is only time to complete a physical examination, documentation, reassuring patients nothing dangerous is wrong and perhaps offering them various options for management, such as physiotherapy or a free mindfulness course.
… I can’t do more… I don’t have time to explain anything else (I).
One respondent stated explicitly that having time to do a proper examination in the first consultation, having time to listen to patients, would save a lot of money for society, as patients would gain a better understanding of what was wrong, feeling recognized and heard. However, suggests this is not possible in the current setting:
…we can actually [inadvertently] trap them and prolong the course…(J)
Addressing non-biomedical aspects of pain was thought to be dependent on whether patients were willing and ready to engage in such aspects. According to J:
…It all depends on the patient, what stage they are at and whether or not they accept that there are issues to address. (J)
In general, respondents reported leaving non-biomedical aspects alone if they sensed patients were not ready to talk about them. However, some actively encouraged discourse by:
…trying to ask the patient questions, so that they have a sense of reaching the answers themselves or being able to see the correlation. (A)
Respondents all reported engaging in psychological and social aspects of the condition, but there was variation in the degree to which they felt professionally comfortable and when to refer to other professions (D, B, G, E, H).
Societal readiness was stated as influential in routinely addressing non-biomedical aspects of back pain problems. According to G:
… it’s still a thorny issue to explain to [patients] that it is not just biomechanical…(G)
However, G also contends that with large-scale, biopsychosocial driven interventions, this status quo could shift rapidly:
… just look at GLA:D Back… a lot of people being educated and then they tell it to people … I believe it will come out more and more that there are a lot more factors to it than just a structure in the back. (G)
Focus group respondents described patients as being on a continuous search for a single reason for pain, seeking someone to fix it;
…they would like a quick fix (H).
However, respondents reported engaging in giving responsibility back to patients, explaining that there is not a quick fix for pain. This means that, to improve, patients need to take responsibility for aspects of their life that might be the cause of pain, rather than thinking it can be fixed by someone else.
…The most important thing is to get them [patients] to take responsibility. (G)
One HCP described that in the future:
…we will work much more for the patient. What experiences has [the patient] had? … I am a listener, but it is [their] problem. (J)
Theme 4: More than a label – individual explanations for pain
Respondents reported moving away from settling on and using a diagnosis, as no diagnosis tends to suffice (F), and instead developing a focused explanation for a nuanced problem with emphasis on the benign nature of the pain (A, F, G). In focus group 1 the need for a diagnosis was explicitly questioned and debated. C stating that he does not need a label to help patients. The following quote is illustrative of this discourse:
I don’t need anything to be wrong with them – I don’t need a word put to it, unless they need to have a word put to it…but if [a word should be put to it] …then it has to make sense to them [patients]. (C)
When providing a diagnosis, it was primarily to accommodate patients’ needs, and to illustrate what the cause of pain is not; for example, that arthrosis or signs of a prolapsed disc do not provide the answer as to the cause of the pain, as these are also found in non-symptomatic individuals. If a word was to be produced, words such as load-related, overload, lumbago and sciatica were suggested. One respondent stated that the word must describe the complexity (E), others stated that they just called it back pain (A), and J stated disliking the NSLBP diagnosis, as:
….it makes it so mysterious. (J)
As reasons for pain were considered individual, diagnosis was individualized;
…pain wise the picture is often the same… but their background [reason for pain] is often very different… (E)
Diagnosis was regarded as a process, since reasons for pain could not be identified until patients let down their guard, or were ready to accept that, perhaps, non-biomedical reasons for pain exist;
…it takes a few visits before we reach the core of what is worrying them. (C)
Thus, diagnosing was customized, in the sense that explanations differed from person to person; depending on identified reasons for pain and how patients react to different explanations;
…but it is just so individual who is in front of me…what they present with…and how they react. (H)
Moving forward, the most important aspect was perceived as patients getting a sense of coherence (E, C), or patients feeling recognized (A, D).
In summary, HCPs expressed a highly nuanced understanding of NSLBP, which moved beyond a biomedical diagnosis, identifying both the values and beliefs of patients, relatives, researchers, and society as affecting the condition, as well as an unhealthy work culture within our society and the structure of the Danish medical and welfare system as possibly affecting and prolonging suffering.
This study set out to explore HCPs’ perspectives on diagnosing NSLBP in a way that might assist communication that moves beyond a biomedical diagnosis. The initial reason for doing so was to identify a label to better communicate with patients about their pain and pain-related problems. However, our respondents did not seem to need a label. Rather, we identified 4 themes relating to diagnosing NSLBP in a way that may assist communication beyond a biomedical diagnosis. These described multiple elements of a diagnostic practice that goes beyond a biomedical diagnosis, assisting patients in understanding the complexity of pain and being engaged in disease management. It emerged that, within the confines of daily practice, a more simplistic biomedical model replaces the intended biopsychosocial approach.
Despite existing evidence to support that HCPs are holding on to a biomedical understanding of the condition, providing patients with a variety of unhelpful biomedical explanations for pain (8–10), this study indicates that there are HCPs who carefully consider the complexity of NSLBP and express a nuanced understanding of the condition.
HCPs included in this study identified the values and beliefs of multiple social actors and the culture within society as possibly affecting and prolonging suffering. These perspectives are well aligned with the SD framework and with existing evidence suggesting that the experiences, attitudes and beliefs of multiple stakeholders affect the condition, and how it is perceived and treated (3, 8, 11, 12, 30–32). The biomedical rhetoric of HCPs has previously been found to reinforce patients’ beliefs that the spine is vulnerable (33) and contributes to increased levels of fear (34). Evidence suggests that the discourse of HCPs may be the most common source for patients describing persistent LBP as a broken machine, permanent/immutable, very negative and complex (7). Aligned with this, interventions that address misconceptions about LBP amongst HCPs, patients, the media, and the general public have been recommended (4, 35, 36).
We observed that the nuanced understanding of NSLBP expressed by HCPs appeared difficult to translate into practice. HCPs identified elements, such as the timeframe of the medical consultation, patient expectations and work-related traditions, as reasons for sometimes not engaging in psychological or social elements of the condition. These aspects and the lack of interprofessional knowledge were also identified as barriers to shared interprofessional decision-making. HCPs pointed to the issues that patients want someone to fix their pain, that they may have difficulties in accepting or believing non-biomedical reasons for pain, and that HCPs leave psychological and social aspects alone if patients are not ready to talk about them. From a SD perspective, such practices could be understood as the product of a biomedical culture within society, which points to the importance of intervening not only at the patient level, but at the societal level, when treating the condition. Thus the medical system and the educational system of HCPs are sites of intervention. Similar arguments have recently been put forward that cultural and system changes must be initiated in order to prevent disabling LBP (4).
One of the implicit expectations of a biomedical paradigm is that HCPs are expected to possess the knowledge and ability to cure disease (37). Illich (38) argues that the medicalization of illness within a biomedical paradigm has the iatrogenic effect that people “lose the personal ability to cope with reality as a result of their gain in healthcare” (38); that a medically harmful effect happens to the individual if others take over responsibility for their health. Hence, arguing that patients’ expectations that NSLBP can be fixed by HCPs might be an iatrogenic effect of a biomedical paradigm. From a SD framework, it might be argued that in order to give back responsibility to patients and to empower them to cope with their condition, the implicit power-relations of a biomedical paradigm and the roles in which we are placed should be restructured (17).
HCPs in this study did not perceive a need for a diagnostic label, arguing rather for a dynamic model addressing individual contributors to pain, emphasizing that back pain should be understood and addressed individually. These perceptions align with the approach of cognitive functional therapy (CFT), and may, for some respondents, be inspired by CFT, in which the relative contribution from different biopsychosocial factors and their interaction is considered variable and unique from person to person and to vary on a temporal basis (39). It is argued by the developers of CFT, that explaining such individual and dynamic reasons for pain to patients will empower them to develop a clear understanding of their condition and factors contributing to pain (39). However, HCPs in the current, and other, studies, have pointed to the issue that different and unclear explanations for pain within the medial system might be a source of frustration to patients, possibly leading to psychological harms (11, 12) and overdiagnosis (15). More knowledge is needed to explore how individual explanations may be used in a way that empowers patients and helps them make sense of their condition, rather than in a way that is perceived as different conflicting explanations.
This study has some methodological limitations. First, in alignment with the paradigm of this study, the aim was not to find a single truth regarding the interpretation of HCPs’ perspectives on diagnosing NSLBP. Consequently, the results of this study are not considered generalizable, however they might be recognizable in similar contexts (19).
CM and EB engaged in critical scrutiny of the data analysis, critically encouraging RL to explore alternative interpretation of the data. Rather than trying to reach consensus on the interpretation of results, seeking to identify a single truth within the data, we sought to enhance the quality of the results by producing an audit trail allowing transparency, so that others can understand how concepts, codes and themes were developed (19, 29) . However, we acknowledge that the single source primary code list may be considered a limitation of the current study.
The lack of GPs in focus group interviews may have limited the generation of data, since GPs add heterogeneity to the group dynamic, possibly allowing for a wider variety of perspectives to be discussed. However, the focus group dynamics were good, which allowed for rich data production, and the use of individual interviews as a complementary method allowed production of in-depth knowledge from the GPs’ perspective.
Chiropractors and physiotherapists involved in this study had previously engaged in the GLA:D Back programme, which is informed by social cognitive theory and cognitive behavioural theory (18). This may have affected respondents’ perceptions of NSLBP, or the programme may simply have fitted well with their personal needs or way of viewing the condition. This will have affected the results of the study. However, the purposeful sampling strategy also allowed for generation of rich data relating to diagnosing NSLBP in a way that moves beyond a biomedical diagnosis.
HCPs included in this study were not offered the possibility to comment on the transcriptions or the interpreted results. If this had been enabled, it would have allowed for reflexive elaborations, critique and feedback, underpinning the production of knowledge as a continued creative co-construction. This would also have enhanced the credibility of the study (19), as would the use of observations of clinical practice as a complementary method (19). This could be a natural next step.
In conclusion, this study shows that HCPs perceive a need to communicate the complexity of recurrent and persistent NSLBP and to help patients make sense of this. However, a new label to replace NSLBP was not regarded as a priority; the focus being on ways to engage patients in dealing with their individual contributors to pain. There are barriers to integrating a SD framework in practice that still need to be overcome. To understand these barriers in more depth further research is needed into patients’ perspectives and the role of other stakeholders.
Conflicts of interest. AK’s position at the University of Southern Denmark is financially supported by the Foundation for Chiropractic Research and Postgraduate Education. GLA:D® is a non-profit initiative hosted at the University of Southern Denmark, and the GLA:D® trademark is the property of the University of Southern Denmark.


 Click to show fullsize
Click to show fullsize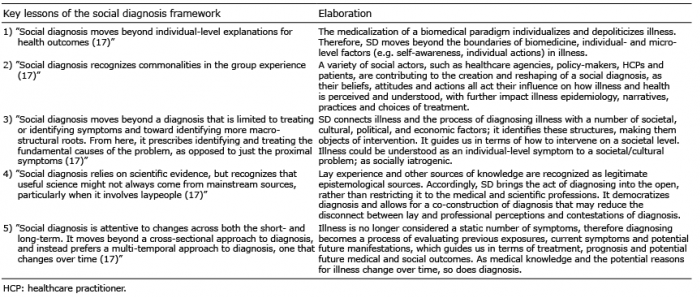 Click to show fullsize
Click to show fullsize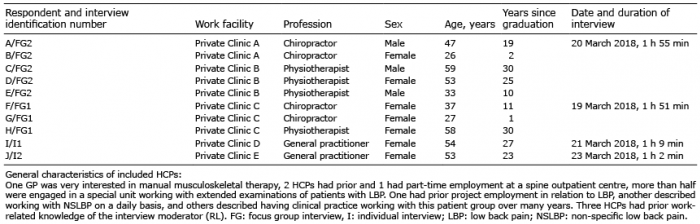 Click to show fullsize
Click to show fullsize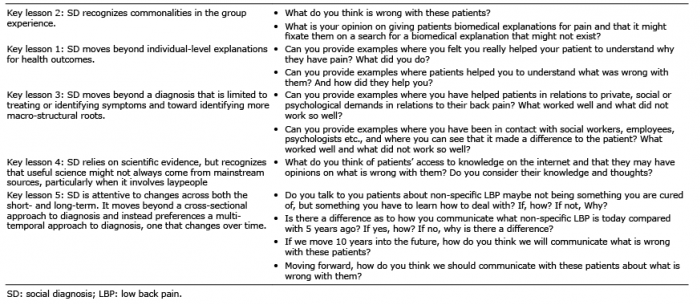 Click to show fullsize
Click to show fullsize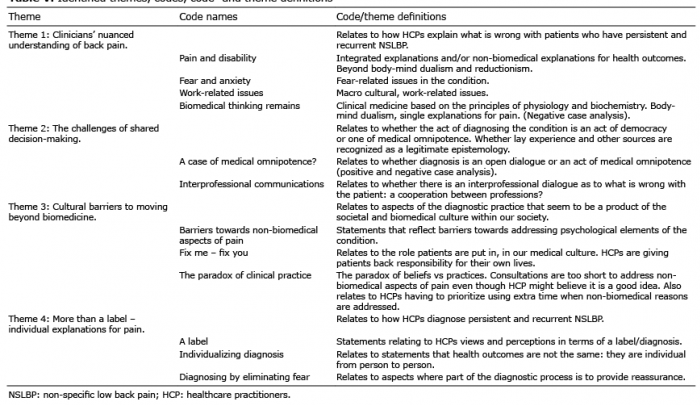 Click to show fullsize
Click to show fullsize